
Abstract
Background
The MRI scanner environment induces marked psychological effects, but specific effects on pain perception and processing are unknown and relevant to all brain imaging studies.
Objectives and methods
We performed visceral and somatic quantitative sensory and pain testing and studied endogenous pain modulation by heterotopic stimulation outside and inside the functional MRI scanner in 11 healthy controls and 13 patients with irritable bowel syndrome.
Results
Rectal pain intensity (VAS 0–100) during identical distension pressures increased from 39 (95% confidence interval: 35–42) outside the scanner to 53 (43–63) inside the scanner in irritable bowel syndrome, and from 42 (31–52) to 49 (39–58), respectively, in controls (ANOVA for scanner effect: p = 0.006, group effect: p = 0.92). The difference in rectal pain outside versus inside correlated significantly with stress (r = −0.76, p = 0.006), anxiety (r = −0.68, p = 0.02) and depression scores (r = −0.67, p = 0.02) in controls, but not in irritable bowel syndrome patients, who a priori had significantly higher stress and anxiety scores. ANOVA analysis showed trends for effect of the scanner environment and subject group on endogenous pain modulation (p = 0.09 and p = 0.1, respectively), but not on somatic pain (p > 0.3).
Conclusion
The scanner environment significantly increased visceral, but not somatic, pain perception in irritable bowel syndrome patients and healthy controls in a protocol specifically aimed at investigating visceral pain. Psychological factors, including anxiety and stress, are the likely underlying causes, whereas classic endogenous pain modulation pathways activated by heterotopic stimulation play a lesser role. These results are highly relevant to a wide range of imaging applications and need to be taken into account in future pain research. Further controlled studies are indicated to clarify these findings.
Keywords
Introduction
The perception and processing of pain is highly individualized and powerfully influenced by cognitive and emotional mechanisms, with genetics and physiologic factors also playing important roles.1,2 Attention, expectation, distraction, hypervigilance, reappraisal, anxiety and mood can affect pain intensity or cause painful experiences without any nociceptive input. 3 These mechanisms play an important part in chronic functional pain syndromes, where an organic cause is not obvious. Irritable bowel syndrome (IBS) is one of the most prevalent functional pain disorders associated with changes in bowel habits and affecting approximately 10–15% of many populations. 4 These patients often have co-morbid psychological disorders such as depression and anxiety, 5 influencing central processing of pain and resulting in sensory hypersensitivity, sensitization and abnormal endogenous pain modulation (EPM).6–9 The symptom presentation in IBS can be affected by experimental manipulation of the psychological state, such as emotion induction and pharmacologic intervention.10–13 The hypersensitivity in IBS is also highly responsive to the expectation and anticipation effects underlying placebo and nocebo manipulations.14,15 Emotions have been shown to modulate experimentally-induced pain perception in healthy subjects, with negative emotions increasing and positive emotions decreasing pain perception. 16 Moreover, various cognitive processes can bias pain perception and processing in the healthy brain. 17 Therefore, the consideration of psychological factors in the interpretation of pain processing data is of paramount importance.
Brain functional magnetic resonance imaging (fMRI) is used to study pain processing by evaluating the haemodynamic response of the brain in relation to neural activity and has shown aberrant sensory processing in various pain disorders, including IBS.9,18,19 Areas consistently affected include those integrating and governing psychological responses and EPM, such as prefrontal regions, cingulate cortices, insula, amygdala, cerebellum and the dorsal brainstem.3,20 Good concordance was reported between the psychological abnormalities in chronic pain disorders and abnormal brain activation patterns in these regions. This has been shown especially for the important modulatory factors of anxiety, hypervigilance and expectation.14,21–24 To avoid artefacts in these sensitive imaging measures, a neutral and standardized testing environment is important. However, the highly artificial brain fMRI scanning environment itself, on which the definition of processing abnormalities is based, has received surprisingly little scrutiny despite undisputed induction of many psychological modulations known to affect pain processing. MRI examination is known to induce anxiety- and stress-related reactions. These reactions may involve the fear of enclosed places, and distress induced by the hammering noise and the temperature inside the tunnel, the expectation of being hurt, the worry of the unknown, and the stress of coping with the unusual environment.25–28 Patients who suffer from mood disorders are particularly vulnerable to the stressful properties of the MRI scanner environment. 29 The effect of the fMRI environment on pain perception has to the best of our knowledge never been reported. Therefore, the current study investigated whether the fMRI scanning environment induces alterations in visceral and somatic pain testing, as well as in the endogenous modulation of pain, in IBS patients and healthy controls, and whether the IBS patients are affected differently from controls.
Materials and methods
This was a retrospective investigation of an imaging study performed in IBS patients and healthy controls in a single centre at the National University Hospital of Singapore (NUH), from February 2009 to December 2010. All patients included in the original imaging study were also included in this data re-analysis.
Inclusion and exclusion criteria
Thirteen male and female IBS patients diagnosed according to the Rome III criteria 30 and aged 21–70 years were recruited from the NUH gastroenterology and colorectal clinics or by public advertising. Study inclusion criteria for IBS were an IBS symptom rating of at least 175 using the IBS severity scoring system (IBS-SSS; moderate intensity) 31 in the last two weeks before study inclusion, with discomfort or pain due to IBS as the most prominent symptom. Main exclusion criteria included any organic gastrointestinal or other significant systemic disease, including cardiovascular, psychiatric, neurological and endocrine diseases, chronic or acute pain conditions, abdominal operations except appendectomy or hysterectomy, a history of brain disease or brain surgery, pregnancy or lactation, any medication known to affect nociception, drug abuse, claustrophobia or metal implants in the body. Eleven healthy volunteers matched for age and without any gastrointestinal pathology or history of significant abdominal pain, bowel disorders, bloating or discomfort during the last three months, as well as the above exclusion criteria and the absence of any ongoing medication were recruited by word of mouth. None of the patients or controls had previously participated in clinical trials or undergone MRI scanning.
Ethics approval and consideration
The study protocol was approved by the Institutional Review Board and Domain Specific Review Board of the National Healthcare Group, Singapore. All participants gave written informed consent and were remunerated for their participation. The trial was registered at Clinical Trials.gov with the number NCT00693732.
Study procedure
Subjects were seen on two occasions. At the first visit the IBS-SSS score, average abdominal pain and discomfort intensities in the past week on a computerized, anchored, horizontal visual analogue scale (COVAS; 0 = none, 100 = maximum bearable), average pain and discomfort duration, the Perceived Stress Scale 10-item questionnaire (PSS-10), 32 the Hospital Anxiety and Depression Scale (HADS) 33 and general demographic data were completed and subjects were familiarized with the study procedures. Patients then completed the two-week observation run-in period for prospective assessment of symptoms and pain. The actual experimental procedures were performed two weeks after the first visit. The sensory tests were always performed in the same time window in the morning to minimize diurnal rhythm influences and within 7–14 days after the end of the menstrual period in women to standardize the influence of the menstrual period. Identical instructions were given before each test and ambient test conditions were standardized and similar for the sessions inside and outside the scanner. Participants first underwent a series of stimulations lying in a supine position on an examination bed outside the scanner, in the preparation room connected to the MRI scanner room. The ambient conditions, including temperature and humidity, were identical to those within the scanner room. Rectal distension, foot heat, and simultaneous rectal distension with foot heat heterotopic stimulation were performed in randomized order (see below for details). Heterotopic stimulation, also described as conditioned pain modulation, is a standardized method for induction of EPM.34–36 Participants were then transferred to the scanner room, and moved into the MRI scanner magnet in supine position with the head coil and restraint in situ. They were instructed that they would experience rectal, foot, and rectal with foot stimulations in random sequence, exactly as had been performed outside the scanner, after a relaxation period of 30 min. Brain scanning was performed in subsequent sessions, but these data are not reported as part of this paper.
Rectal stimulation protocol
An enema of 300 ml of warm water was instilled for evacuation of the rectum. After testing for leakage by inflating with air under water, a lubricated 400 ml polyethylene bag (Mui Scientific, Toronto, Canada) attached to the top of a flexible catheter was inserted 5 cm into the subject’s rectum in left lateral position. The bag was slowly inflated with air to a pressure of 5 mmHg to ensure good contact between the bag and the rectal mucosa. The subject was positioned on a bed in a comfortable supine position with legs slightly apart, covered with a light sheet with the knees flexed and supported on pillows. After a 5-min acclimatization period, the preliminary quantitative sensory tests described below were commenced.
First sensation, first pain and pain tolerance rectal distension thresholds were determined using an ascending methods of limits (AML) protocol with incremental steps of 5 mmHg, 30-s distension and intermittent rest periods applied by a barostat (G&J Electronics Inc., Toronto, Canada), which was programmed to an inflation speed of 40 ml/s and a cut-off pressure of 60 mmHg. Additionally, within the AML protocol the pain intensity ratings were recorded by COVAS at the end of every stimulus step. Rectal distension thresholds were measured twice with a 30-s break and the results from the second run were used for analysis to avoid novelty effects. Five minutes later, the stimulation pressure which induced a moderate pain intensity (VAS 30–55) at the end of the 30-s distension was determined from the second stimulation run and used as the tonic rectal distension pressure, which was applied separately for 30 s. The pain intensities were recorded before and after the stimulation procedure on the COVAS scale.
Foot heat stimulation protocol
After a break of 10 min, a contact thermode (Medoc Pathway model, ATS/CHEPS system, Ramat Yishai, Israel) was placed halfway along the dorsum of the left foot and fastened by an elastic rubber strap. The first heat sensation, first pain and pain tolerance thresholds were determined using an AML protocol with incremental steps of 1℃ (beginning at 36℃ and with a maximum temperature of 48℃) and 30-s stimulation and rest periods. Pain intensity ratings were recorded by COVAS at the end of every stimulus step. Five minutes later, the stimulation temperature inducing moderate pain intensity (VAS 30–55) at the end of the 30-s stimulation was determined and used as the tonic foot heat pain stimulation, which was separately applied for 30 s. Pain intensity was recorded by COVAS before and after the stimulation.
Heterotopic (rectal plus foot) stimulation protocol – activating EPM
After a break of 10 min, foot heat pain and rectal distension pain at the titrated moderate intensities determined above were performed simultaneously (heterotopic stimulation for EPM) for 30 s. Subjects were instructed to focus on only their rectal pain during heterotopic stimulation. Rectal pain intensity was rated after 30 s on the COVAS scale.
Statistical analysis
Data were analysed using SAS 9.3 (SAS Institute, Cary, NC, USA). Continuous variables were expressed as the arithmetic mean with 95% confidence intervals (CIs), and categorical variables were expressed as frequencies and percentages. Significance thresholds of p < 0.05 were applied. EPM was defined as the rectal pain intensity rated after 30 s during heterotopic foot stimulation minus the rectal pain intensity rated after 30 s without heterotopic foot stimulation.
The sensory and pain thresholds measured outside of the scanner were compared between IBS patients and healthy controls by unpaired Student’s t-test. To compare mean pain ratings in response to tonic pain stimulation outside and inside the scanner, as well as between IBS patients and controls, a two-way mixed ANOVA with ‘group’ (IBS versus controls) as the between-subject factor and ‘scanner’ (inside versus outside scanner) as the within-subject factor, was used. To test for a differential effect of the scanner environment between IBS patients and controls, a ‘group’-by-‘scanner’ interaction effect was included.
Analysis of covariance with ‘group’ and ‘pain ratings inside the scanner’ as categorical and continuous independent variables, respectively, and ‘pain ratings outside the scanner’ as the dependent variable was estimated; the ‘group’-by-‘pain ratings inside the scanner’ interaction effect was tested to check whether the relationship between pain ratings inside and outside the scanner differed significantly between IBS patients and controls.
Results
Participants
Subject characteristics
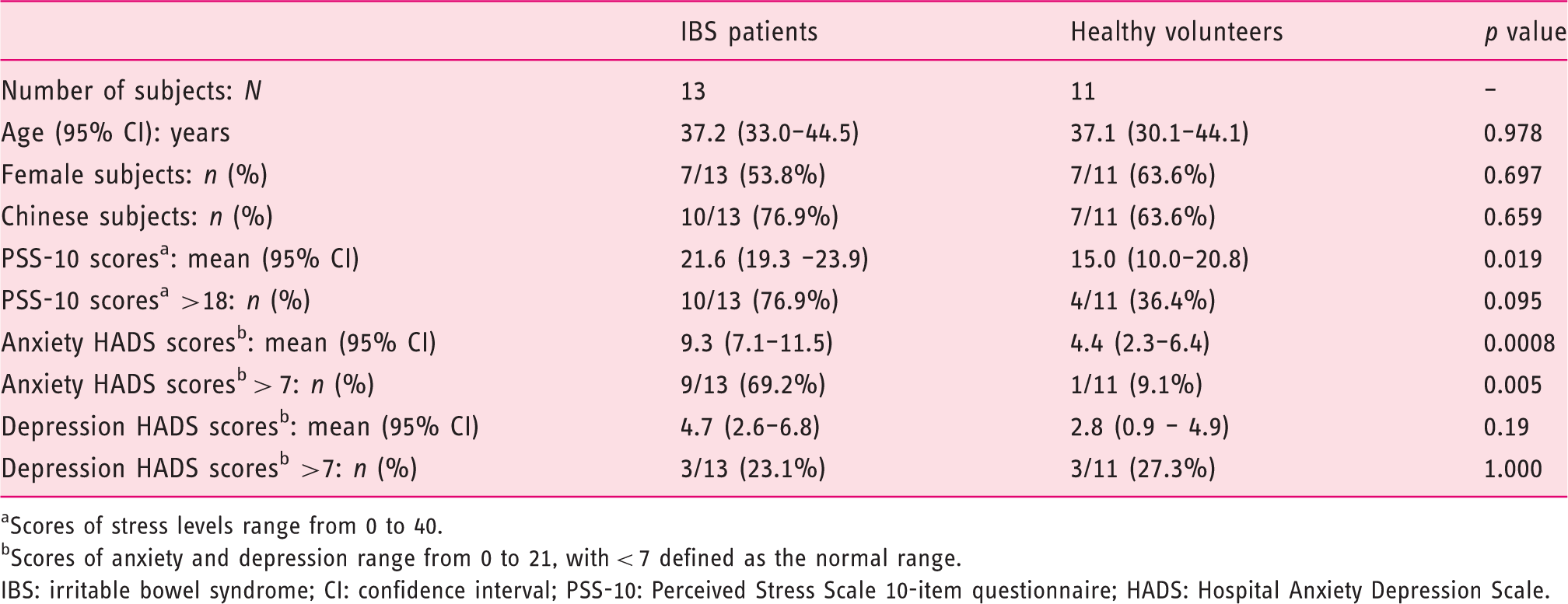
Scores of stress levels range from 0 to 40.
Scores of anxiety and depression range from 0 to 21, with < 7 defined as the normal range.
IBS: irritable bowel syndrome; CI: confidence interval; PSS-10: Perceived Stress Scale 10-item questionnaire; HADS: Hospital Anxiety Depression Scale.
Rectal thresholds and pain intensity during stimulation outside and inside the scanner
Titration of visceral and somatic thresholds and moderate pain outside scanner
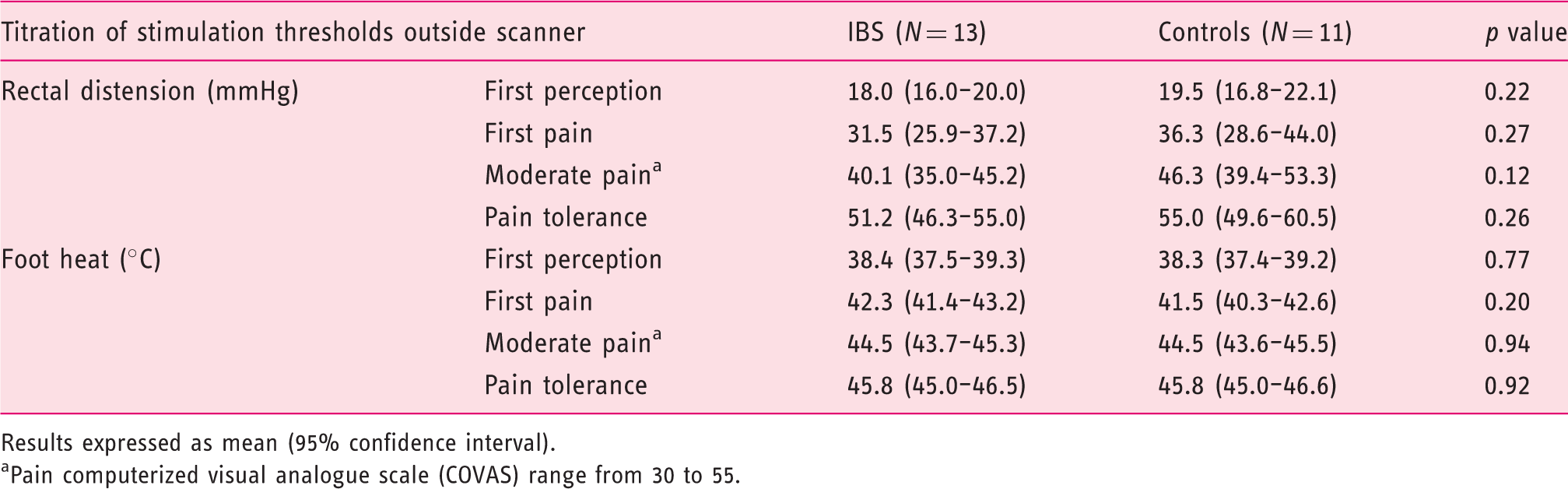
Results expressed as mean (95% confidence interval).
Pain computerized visual analogue scale (COVAS) range from 30 to 55.
Two-way mixed ANOVA analysis showed a significant main effect of ‘scanner’ (F1,22 = 8.78, p = 0.006), due to significantly higher rectal pain ratings inside versus outside the scanner, but no significant main effect of ‘group’ (F1,22 = 0.01, p = 0.92), indicating similar pain ratings between groups over both measurements (Figure 1). Furthermore, there was no significant scanner-by-group interaction effect (F1,22 = 0.66, p = 0.43), indicating that the effect of the scanner environment did not differ significantly between IBS patients and healthy controls.
Scanner environment effect on visceral pain in irritable bowel syndrome (IBS) subjects and controls.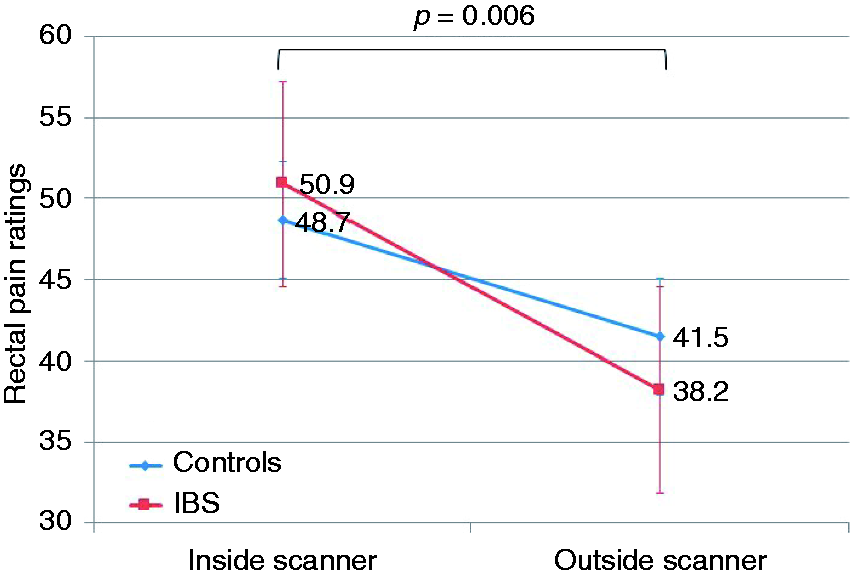
A trend for the ‘group’-by-‘pain rating inside the scanner’ interaction effect in the analysis of covariance (β = 1.30 ± 0.68, p = 0.07) indicated a divergent relationship between pain outside and inside the scanner in IBS patients versus controls.
The difference in rectal pain outside versus inside the scanner (Δ rectal pain, calculated as VASrectal_pain_outside – VASrectal_pain_inside) correlated highly significantly with the stress (r = −0.76, p = 0.006), anxiety (r = −0.68, p = 0.02) and depression scores (r = −0.67, p = 0.02) in controls, but not in IBS patients (r = 0.35, p = 0.25; r = 0.43, p = 0.14; r = 0.48, p = 0.10, respectively). These divergent group effects were confirmed by analyses of covariance with Δ rectal pain as the dependent variable, which showed significant ‘group’-by-‘anxiety’, ‘group’-by-‘depression’ and ‘group’-by-‘stress’ interaction effects (β = 5.77 ± 1.82, p = 0.005; β = 5.85 ± 1.79, p = 0.004 and β = 3.20 ± 1.20, p = 0.015, respectively).
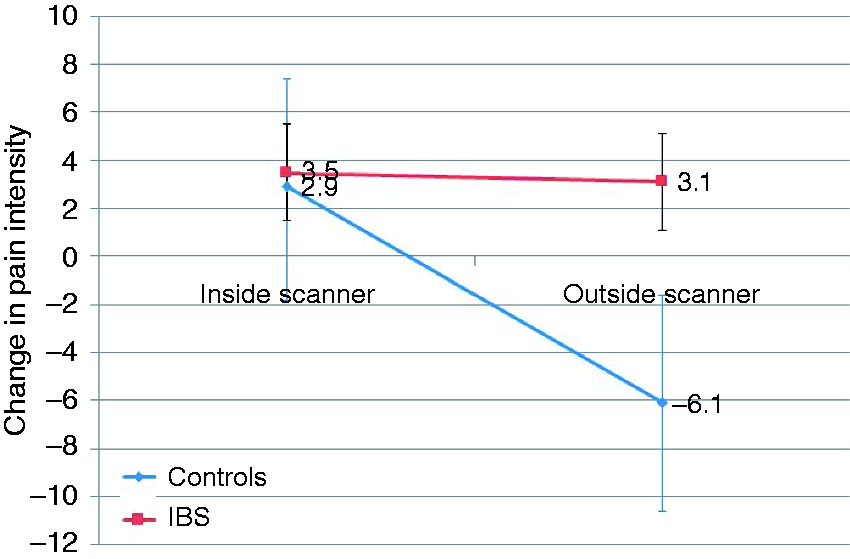
Endogenous visceral pain modulation outside and inside the scanner
EPM in IBS patients and controls is shown in Figure 2. The difference between IBS patients and controls in the change in rectal pain intensity during induction of EPM outside the scanner showed a trend (p = 0.09). The lack of significance may be due to the small sample size, and the effect size was large (Cohen’s d = 0.81). The mean change in pain intensity during EPM outside the scanner was an increase of 8% (3–20%) in IBS patients and a decrease of 9.6% (–75.4–56.1%) in controls. Two-way mixed ANOVA analysis showed neither a significant main effect of ‘scanner’ (F1,22 = 3.15, p = 0.09), due to insignificant effects on EPM outside versus inside the scanner, nor of ‘group’ (F1,22 = 3.01, p = 0.10), indicating largely similar EPM between groups over both measurements. The ‘scanner’-by-‘group’ interaction effect with EPM was also insignificant (F1,22 = 2.64, p = 0.12), demonstrating that the effect of the scanner environment did not differ significantly between IBS patients and healthy controls (see Figure 3). It should, however, be noted, that the ‘scanner’, ‘group’ and their interaction effects clearly yielded trends, which may be insignificant due to the small sample size. Figure 2 illustrates the divergent individual and group effects, with an overall switch from inhibition to facilitation of EPM in controls from outside to inside the scanner (Cohen’s d = 0.78, i.e. medium–large effect size), whereas IBS patients as a group maintained facilitation both outside and inside the scanner (Cohen’s d = 0.06, small effect size).
Individual endogenous pain modulation inside versus outside MRI scanner. (Individual data are indicated by round symbols, whereas mean values are signified by squares. The difference in mean values inside and outside the scanner is not significant in controls or in irritable bowel syndrome (IBS) patients.). Scanner environment effect on endogenous pain modulation in irritable bowel syndrome (IBS) subjects and controls.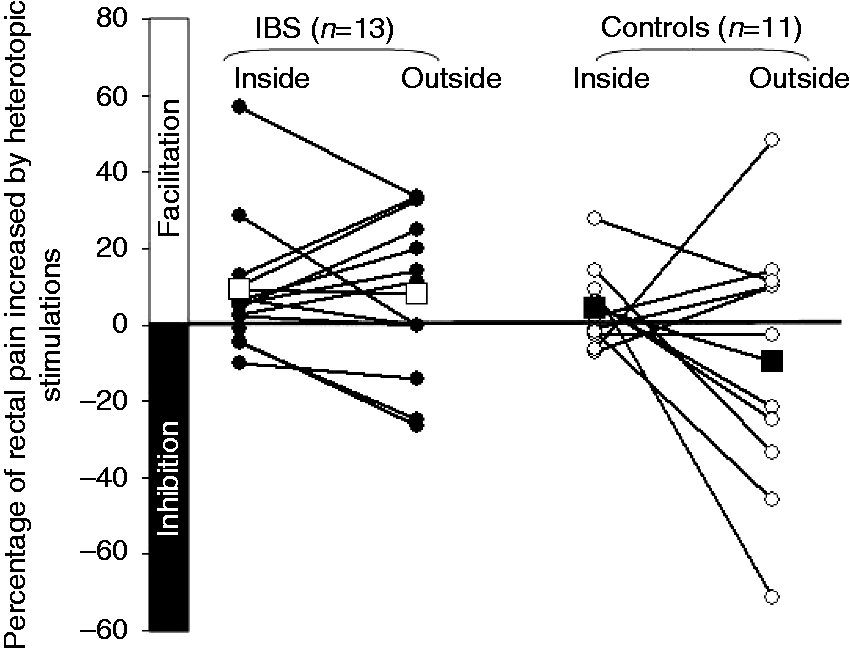
The change in EPM outside versus inside the scanner (Δ EPM, calculated as EPMoutside – EPMinside) correlated strongly and significantly in IBS patients (r = 0.65, p = 0.02), but only weakly, inversely and non-significantly in controls (r = –0.33, p = 0.32). The significant effect in the ‘group’-by-‘EPM scanner’ interaction in the analysis of covariance (β = 0.64 ± 0.22, p = 0.009) confirmed the divergent relationship between EPM outside and inside the scanner in IBS patients versus controls suggested by the correlation results above.
The difference in EPM outside versus inside the scanner did not correlate significantly with the stress (r = 0.15, p = 0.66), anxiety (r = 0.03, p = 0.93) or depression scores (r = 0.29, p = 0.39) in either controls or IBS patients (r = 0.18, p = 0.55; r = −0.08, p = 0.79; r = 0.11, p = 0.72, respectively).
Somatic thresholds and pain intensity during stimulation outside and inside the scanner
Foot heat sensation, first pain, moderate pain and pain tolerance thresholds were similar in both subject groups (Table 2). No difference was observed in the titrated temperature for induction of moderate foot heat pain between the two groups and the induced mean pain intensity outside the scanner was similar in IBS (44.8 (39.0–50.5)) and control subjects (40.9 (29.3–52.5))(p = 0.52). Two-way mixed ANOVA analysis confirmed the absence of significant main effects for ‘scanner’ (F1,22 = 0.87, p = 0.36) and for ‘group’ (F1,22 = 1.10, p = 0.31) on somatic pain. Furthermore, there was no significant ‘scanner’-by-‘group’ interaction effect (F1,22 = 0.10, p = 0.76), indicating that the effect of the scanner environment on somatic pain was similar between IBS patients and controls (Figure 4).
Scanner environment effect on somatic pain in irritable bowel syndrome (IBS) subjects and controls.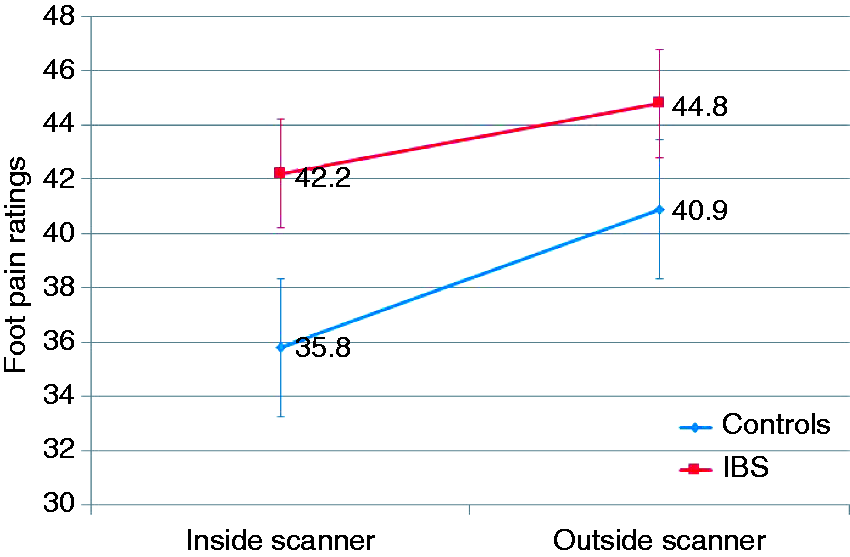
A significant ‘group’-by-‘pain’ rating inside the scanner interaction in the analysis of covariance (β = 1.32 ± 0.56, p = 0.03) suggested divergent correlations between IBS patients versus controls.
The difference in foot pain outside versus inside the scanner did not correlate significantly with the stress (r = −0.49, p = 0.12), anxiety (r = −0.58, p = 0.06) or depression scores (r = −0.28, p = 0.41) in controls or in IBS patients (r = 0.28, p = 0.36; r = −0.04, p = 0.91; r = −0.09, p = 0.78, respectively).
Discussion
The fMRI scanner environment significantly increased experimentally induced visceral pain intensity in patients with IBS and in healthy controls, whilst somatic pain was not affected. The increase in visceral pain in the scanner correlated closely with the trait anxiety, stress and depression scores in healthy controls, but not in IBS patients with ab initio increased anxiety and stress. There were trends towards differences in EPM between IBS patients and controls both outside and inside the scanner (‘group’ effect), as well as between outside and inside locations (‘scanner’ effect), which fell short of significance. These data suggest psychological processes underlie the selective visceral hyperalgesia induced by the scanner environment.
The scanner setting has previously been shown to enhance anxiety as well as other psychological factors in healthy subjects and in patients with pre-existing panic disorder and agoraphobia, to precipitate unintended mood alterations and to increase levels of the stress hormone, cortisol, in healthy volunteers.25,37 Anxiety levels are increased in anticipation of scanning and in the scanner, and it is recognized that augmented anxiety, as well as anxiety sensitivity – the fear of anxiety-related sensations and its perceived harmful consequences – are associated with enhanced pain and worsened pain outcomes. 38 The expectation of pain is a proven principle factor in determining the intensity of subsequently experienced pain and is influenced by positive or negative mood and anxiety.14–16,39,40 The majority of evidence has indicated that negative mood or the expectation of increased pain significantly exacerbate pain, whereas positive mood, good coping skills or the expectation of reduced pain prominently attenuate pain.41–47 These factors may explain the increased pain reports inside the scanner. Several studies also examined the effect of MR scanner-associated noise on brain activation patterns. There was not only activation in the auditory processing regions, but also interference with the stimulation presentation and altered attentional demands.48–50
The ANOVA analysis indicated a divergent effect of the scanner environment between IBS patients and controls, which did not reach significance. However, the covariance analysis revealed a strong trend for the interaction of ‘group’ with ‘pain rating inside the scanner’, with a medium-large effect size, indicating significance would be reached with a larger sample size. Stress and anxiety responses vary considerably inter-individually and are related to underlying neuroendocrine and psychological factors, including the cortisol response, the level of arousal and the impact of individual trait differences. 51 In our healthy controls a close correlation existed between trait anxiety, stress and depression levels and increased visceral pain inside the scanner, in accordance with the above-mentioned susceptibility factors. Such a correlation was not evident in IBS patients, who already had elevated anxiety and stress scores outside the scanner. The a priori elevated psychological arousal levels may explain the lack of linear relationship between background anxiety and stress and further pain changes in the scanner.35,52–55 The recording of state anxiety and anxiety sensitivity measures inside and outside the scanner and personality traits for characterization of further pain endophenotypes would have yielded additional useful information, but they were not available in this study. 56
The increase seen in visceral pain inside the scanner was not reproduced for somatic pain and there also was no correlation between anxiety, stress and depression and somatic pain changes in either subject group. The psychological modulation of visceral and somatic pain consequently appears to be differentiated. Psychological variables in IBS have been extensively explored in visceral hyperalgesia, but not in somatic hyperalgesia. In one recent study in IBS, patients’ skin thermal hypersensitivity was considerably less associated with psychological factors than visceral hypersensitivity. 15 A possible explanation for a selective visceral modulation could be a selective hypervigilance towards visceral stimuli based on the subjects’ awareness of the gastrointestinal focus of the study. In a recent psychophysiological study participants showed greater responses to an expected pain modality than to an unexpected one. 57 An underlying mechanism for the selective effects may be the more extensive involvement of autonomic and affective brain modulation in visceral stimulation and the bias towards spatial encoding in somatic stimulation.58,59 An illustration of this is the greater activation of the nucleus cuneiformis, a nucleus of the brainstem reticular formation, during visceral pain than during somatic pain in a recent human fMRI study. 59 This nucleus receives emotive, autonomic and executive input and has a potential facilitatory role in the development of central visceral sensitization.59,60 Activation in the periaqueductal grey, a brainstem area strongly implicated in pain modulation, was also shown to be correlated with anxiety during visceral stimulation but not somatic stimulation. 59 We, therefore, speculate that psychological and affective factors involved in the expectation of visceral pain are more likely to influence visceral pain processing than somatic pain.
Hypersensitivity in IBS is associated with dysfunctional EPM, as was also evident outside the scanner in the current study,15,54,55,61 where trends, albeit falling short of significance, for ‘scanner’ or ‘group’ effects on EPM, as well as their interaction, were demonstrated. The effect size analysis indicated that these insignificant trends are likely due to the small sample size. The pain facilitation seen in the majority of IBS patients was similar outside and inside the scanner, whilst in controls there was a net change from pain inhibition to facilitation from outside to inside the scanner, with considerable intra-individual variability. This variability is unlikely to be due to poor test reproducibility, as heterotopic stimulation has been validated as a reproducible method for induction of EPM in healthy volunteers.35,62 Our data show that trait stress, anxiety and depression do not play a major role in EPM, although state psychological factors may contribute to the variability in EPM. 61 However, recent evidence in healthy controls indicates the predominant effect of anxiety or anxiety sensitivity on pain is relayed via cortical pathways and not via those assessed by heterotopic stimulation, which include major spinal and brainstem components.9,55,61,63 Within this context it appears probable that EPM is involved in the scanner-induced effects, but that the anxiety–expectation–fear network, constituted mainly by the amygdala, prefrontal and cingulate cortices, is the main driver of the response.64–67
This study has several limitations. The numbers of subjects included in the study are relatively small, as it was primarily powered and designed for imaging comparisons. For this reason, no subgroup analysis, including that between the IBS subtypes or genders, was performed. The lack of a randomized test sequence is a potential issue, which arose from this being an extended analysis of existing study data. However, we feel that this is unlikely to significantly compromise the results for the following reasons. In the case of an order effect, habituation or a training effect with resultant decreased pain perception would be assumed with repetition of pain testing. 68 However, despite the MRI session consistently being the second session, a significant increase in visceral pain was observed. Sensitization is highly unlikely with a resting period of 30 minutes between sessions and would have affected both somatic and visceral pain perception, which was not the case in the current study. Interaction and order effects have been previously described between imaging and non-imaging environments and consequently a standardized test session sequence was chosen for the current study to reduce variability. 68 The significant changes in sensory findings despite the limited sample size attest to the robustness of the effects of the scanner environment. Future studies must integrate more specific psychological assessment tools used at repeated time-points.
In conclusion, the results of the present study suggest that an fMRI environment significantly influences the outcome of pain processing compared with a non-scanner setting. The scanner environment affected visceral pain in both IBS patients and healthy controls in a protocol specifically aimed at investigating visceral pain. Anxiety and stress are the likely underlying modulating causes, whereas classic EPM pathways activated by heterotopic stimulation play a lesser role. These results are highly relevant to a wide range of imaging applications and need to be taken into account in future pain research. Although further controlled studies are warranted, these results are likely to have salience in the design of future neuroimaging studies of visceral pain.
Footnotes
Funding
This work was supported by the Singapore National Medical Research Council, Individual Research Grant (grant number: NMRC/1086/2006).
Conflict of interest
The authors have no competing interests or relevant financial conflicts to declare.
Acknowledgements
We wish to thank Ms Tung Siew Lai, the research assistant for this study, for her expert help in study coordination and subject recruitment. We also wish to thank Mr Christopher Au and Ms Regine Teo, for their expert help with the fMRI scanning.