
Abstract
Background
Concerns about the risk of bowel perforation for same-day computed tomography colonography (CTC) following an incomplete colonoscopy with polypectomy may lead to unnecessarily postponing the CTC.
Objective
The objective of this article is to describe the complications including colon perforations associated with same-day CTC in a cohort who had polypectomies but an incomplete colonoscopy.
Design
We conducted a retrospective study.
Setting
Our study took place in a single, tertiary referral center.
Patients
We studied consecutive patients who had CTC the same day as an incomplete colonoscopy with polypectomy.
Interventions
Interventions included optical colonoscopy (OC), endoscopic polypectomies, and same-day CTC.
Results
A total of 3% of patients undergoing colonoscopy from January 2008 to December 2012 had same-day CTC following incomplete OC, and 72 polypectomies were performed in 34 (or 17%) of these patients. Incomplete colonoscopies were due to colon tortuosity and looping (25), severe angulations (five), colon mass (two), colon stenosis (one), bradycardia (one). Fifty-three percent of the OCs were screening for colon neoplasia, 29% diagnostic and 18% were surveillance of colon polyps. Most polyps were ≤ 5 mm, and found in the left colon. There were no reported complications or perforations associated with same-day CTCs during short- and long-term follow-up.
Limitations
Limitations of our analysis included retrospective single-center design, small number of patients for the occurrence, referral to same-day CTC was not standardized, inability to establish safety of CTC for specific scenarios such as after complex polypectomies, strictures, or advanced IBD.
Conclusions
Radiologists’ apprehension to perform a CTC the same day as an incomplete colonoscopy following polypectomies because of perceived risk of perforation may be unfounded. More data are needed to determine the safety of same-day CTC in patients with high-risk findings during colonoscopy such as a stricture, severe IBD, and after complex polypectomies.
Keywords
Introduction
Colonoscopy is a preferred screening method for colorectal cancer (CRC) but may be incomplete in up to 10% of cases. 1 Reasons include colon redundancy, angulation of loops, severe diverticulosis, benign or malignant strictures, body habitus, patient tolerance, and adhesions. Adjunct modalities to complete visualization of the colon lumen after an incomplete colonoscopy include double contrast barium enema (DCBE) and more recently computed tomography colonography (CTC).2,3
The rate of colon perforation for colonoscopy is 0.03 to 1% for diagnostic and 0.2% for therapeutic procedures with 0.0009% mortality, and 0.02 to 0.24% for DCBE with 0.07% mortality.4–18 A recent meta-analysis by Bellini et al. of the rate of CTC perforation in 103,399 patients indicates a perforation rate of 0.04% (95% confidence interval (CI) 0–0.10; I2 = 29.1%) or one in 2500 studies. 19
Some centers wait days to perform a DCBE following an incomplete colonoscopy with biopsy because of concerns about causing a perforation as a result of the pneumatic pressure and resultant tension on the colon wall from the injection of barium, even though data to support this concern are not robust.20–22
CTC is being used more frequently as an adjunct for colon polyp detection following an incomplete colonoscopy, and test performance appears to be adequate. Some CTC protocols include rapid-dose fecal and fluid tagging, which requires oral ingestion and/or rectal enemas. Generally, patient acceptance of the same-day CTCs following an incomplete colonoscopy has been good, in part possibly due to not needing to repeat bowel cleansing. Centers may be unable to perform same-day CTCs following an incomplete colonoscopy because of inability to schedule it or have the CTC interpreted the same day.23–27 The perforation rate of CTC after an incomplete colonoscopy is similar to screening CTC.6,28 However, as happened with DCBE, waiting up to two weeks to perform the CTC following an incomplete colonoscopy has been suggested owing to concerns about potential complications including colon perforations.15,29 There are no data regarding the outcomes of same-day CTC following an incomplete colonoscopy with biopsies/polypectomies.
Our institution has the ability to perform same-day CTCs following incomplete colonoscopy, and having a polypectomy or biopsy has not been considered an exclusion criterion. The aim of this study was to determine any complications, including bowel perforations, after performing same-day CTC following an incomplete colonoscopy in a group of patients who underwent polypectomies during their procedure.
Methods
A retrospective, single-center chart review from January 2008 until December 2012 was performed for all colonoscopies, and those reported as incomplete were identified. All colonoscopies were performed by board-certified gastroenterologists and colorectal surgeons with or without fellows in training after informed consent. Fujinon high-definition colonoscopes (Fujifilm Corporation, Minato-ku, Tokyo, Japan) were used. Except for aspirin all anticoagulation was stopped according to referring physician instructions. All procedures were performed under monitored anesthesia care using propofol sedation. About half the procedures were performed using room air and the others using CO2 for colon insufflation. The majority of the patients had split or single-dose polyethylene glycol-based bowel preparations. 30 The study was approved by the Cleveland Clinic Institutional Review Board as a minimal risk protocol not requiring patient consent.
At our institution most incomplete colonoscopies defined as inability to reach cecum or an entero-colonic surgical anastomosis are immediately sent to CTC, which is usually performed within two hours. CTCs are not performed in patients with poor bowel preparation. Incomplete colonoscopies that underwent same-day CTC were reviewed, and patients who had a polypectomy comprised the study cohort. The reason for incomplete colonoscopy was recorded. Polyp size, location, histology, and polypectomy techniques were recorded for each individual. Patient age, gender, body mass index (BMI), and previous history of inflammatory bowel disease (IBD), intestinal obstructive/occlusion lesions, carcinoma, and presence of diverticulosis or hernias were captured. To make certain that no delayed perforations or complications occurred, follow-up clinic visits were reviewed in the electronic medical record (EMR) to determine if there was a record of admission following the incomplete colonoscopy or CTC, or of colon perforation. These data were available for all patients in the cohort up to the writing of this manuscript. Descriptive statistics were calculated using Microsoft Office Excel 2010 (Microsoft Corporation, USA), and statistical software JMP 8 (SAS Institute Inc, Cary, NC, USA). Continuous data were analyzed by means, standard deviation and range and statistical significance was established by Student t-test. Categorical variables were analyzed by Fisher’s exact probability test and statistical significance was set for p < 0.05.
This was an investigator-initiated protocol with no external funding.
CTC protocol
No additional bowel cleansing or oral contrast was administered before CTC.
A scout scan was performed to rule out the presence of free air as a complication of the optical colonoscopy and to confirm adequate bowel distention after CO2 insufflation. After informed consent, a soft-tip catheter was inserted into the rectum and the colon was insufflated using CO2 via a pump at constant pressure to a minimal volume of 4 l, and additional volume was administered in 2-l increments at the radiologist’s discretion. Multi-detector row CT scan was then performed with the patient in supine and prone positions in a single-breath hold for each position. Images were reconstructed in the axial phase with section thickness of 1 mm, and sent to an advanced three-dimensional (3D) workstation for interpretation. Intravenous (IV) contrast was not administered. Image interpretation was performed using both two-dimensional (2D) multi-planar images and 3D renderings including prone and supine fly-throughs by a single radiologist (AP).31–34
Results
A total of 198 patients out of 6260 colonoscopies (3.1%) performed during the study period had a same-day CTC after an incomplete colonoscopy, and 34 of the 198 patients (17%) who had a same-day CTC had one or more polypectomies. Reasons for incomplete colonoscopy were colon tortuosity and colonoscope looping (25 cases), severe angulation (five cases), colon mass (two cases), colon stenosis (one case), and bradycardia (one case).
There were 13 males (mean age 67, SD 10.7; mean BMI 29.7, SD 4.9), and 21 females (mean age 64.3, SD 13.4, (p = 0.05 vs males); mean BMI 27.2, SD 6.9, (p = 0.05 vs males)). Fifty-three percent (18/34) were screening, 29% (10/34) were diagnostic and 18% (6/34) were surveillance colonoscopies.
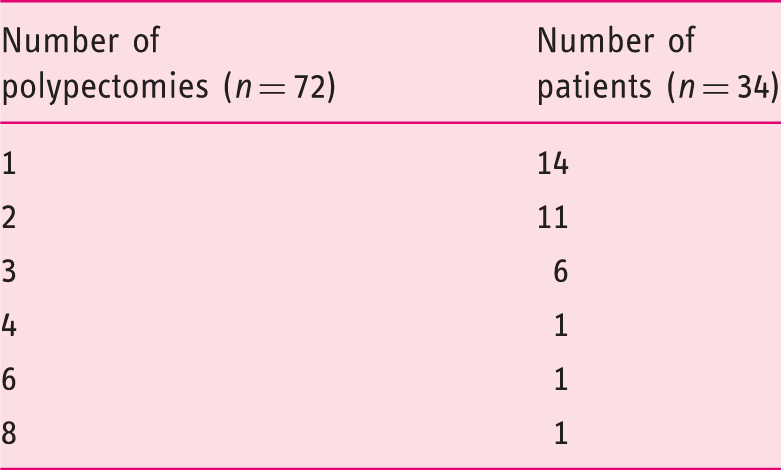
Number of polypectomies performed per patients
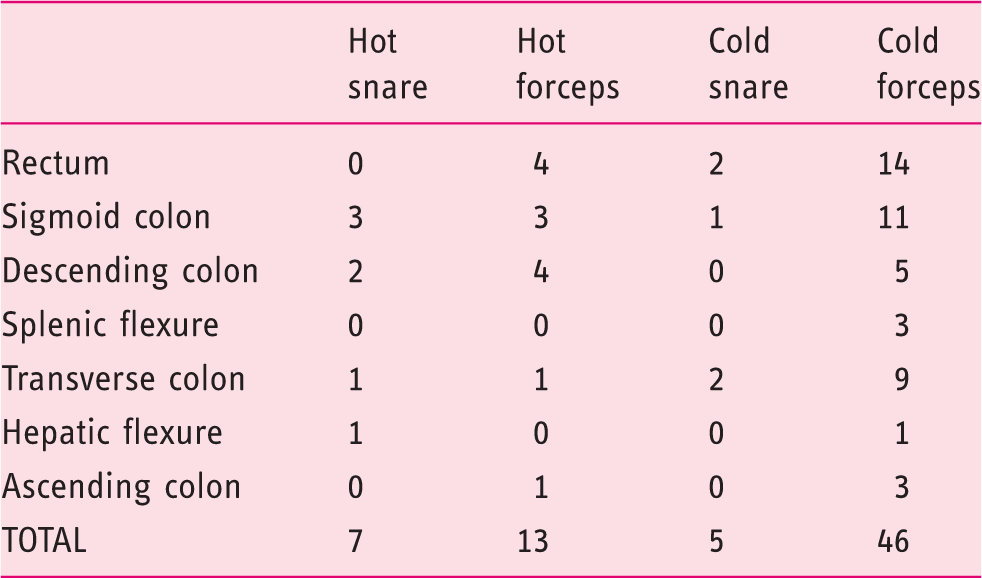
Type of polypectomy performed by location (data were not recorded in one patient)
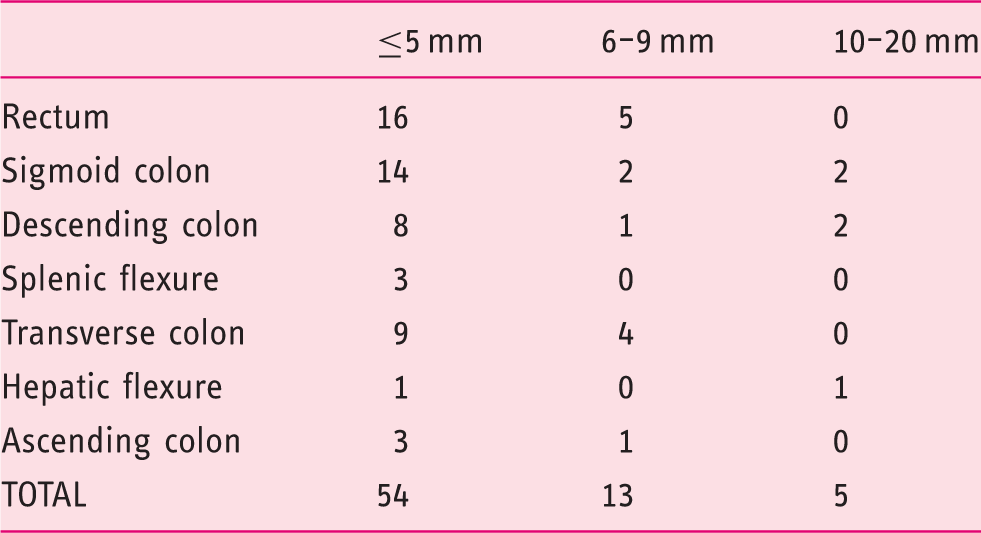
Number of polyps by location and estimated size
Twenty-one patients had colon diverticulosis on CTC. There were three suspected masses seen by colonoscopy, and CTC was recommended to evaluate for presence of synchronous neoplasia or other lesions. These patients then underwent another colonoscopy or surgery. No mass lesion was noted on CTC in one of these patients, confirmed by repeat colonoscopy. A distal transverse colon sessile lipoma was seen during repeat colonoscopy in the second patient, and the last patient had an ulcerated strictured mass in the sigmoid colon that was seen by CTC, which at time of surgical resection showed diverticulitis, and peri-diverticular fibrosis.
The EMR was reviewed and all patients in the cohort had follow-up visits at our institution for unrelated reasons. There was no mention of complications from the colonoscopy or same-day CTC, or admissions for colon perforations through August 2014.
No other colon pathology has been reported in the EMR in this cohort through August 2014.
Discussion
Initial studies involving same-day DCBE following a colonoscopy suggested increased diagnostic accuracy and efficiency when performed the same day, possibly because of the colon cleansing, but the risk of perforations became a concern with the ability to perform colon biopsies and polypectomies.35–37 Barium enema pressures of around 40 mmHg are necessary to perform an adequate double contrast study.20,22,38 Human studies have shown that the luminal pressure needed to perforate the colon is higher than that: lowest in the cecum, and highest in the rectum. The risk increases with biopsies that involve the muscularis propria, which is unusual for routine biopsies.39–41 The perforation risk returned to the rate of controls three to six days after the deep biopsies, which led to the general recommendation to wait at least that long before performing a DCBE. 37 Interestingly, Culp and Carlson showed asymptomatic extravasation of barium following polypectomies (fulguration and/or biopsy) in four of 883 patients, but resection of the suspected perforated sites showed no actual perforation, which suggests that DCBE may over-diagnose micro-perforations that may be clinically irrelevant. 42 Despite this evidence many centers imposed a wait of at least a few days to a week before performing a DCBE following a colonoscopy, and this approach appears to have migrated to CTC also.
In this single-center analysis of patients undergoing same-day CTC following incomplete colonoscopy with polypectomies, all patients had routine long-term clinic visits at our institution that were unrelated to the colonoscopy or CTC, and no complications pertaining to these procedures were mentioned. It is possible that some patients were treated for complications from CTCs at another facility, but this was not mentioned in the EMR as would have been expected.
The majority of our patients were 50 or older, and many had two or more polypectomies, some as large as 20 mm. Perforations associated with DCBE usually involve the rectum and are frequently attributed to the rectal balloon, but CTC studies have noted that the recto-sigmoid junction is also a common area for perforations.6–8 In this study 39 polyps ranging from 1 mm to 10 mm were removed in the recto-sigmoid area without subsequent risk of perforation during CTC. The number of polypectomies >10 mm was small in this study, so it is possible that CTCs could be associated with a higher perforation risk in a larger cohort with larger polypectomies. Three patients had suspected malignancies that ended up being benign, and one of these patients had a diverticular stricture. The numbers are too small to suggest that same-day CTC is safe in these particular scenarios. A recent meta-analysis showed a general CTC perforation rate of 0.04% but only a small number of those patients required surgery (0.008% or 1:12,500) and there was no related mortality. 19 Interestingly, when they excluded patients who had biopsies (14%), hernias, active ulcerative colitis or issues related to colon insufflation, the CTC-related perforation rate dropped to 0.02% (21/103,399). This contrasts with our study, in which same-day CTC after failed colonoscopy with biopsies and snare polypectomies was not associated with colon perforation.
There are benefits to having a same-day CTC after incomplete colonoscopies. There are fewer burdens for a patient to miss a day from work, and no need to repeat a bowel preparation, and in those with a negative CTC another screening or surveillance procedure can be performed at appropriate intervals.33,43 A CTC with positive findings would require another endoscopic or even surgical evaluation.44–48
There are several study limitations. This is a non-randomized, single-center study, and a patient selection bias cannot be ruled out, as there were no criteria for referral to same-day CTC. While at our institution most patients undergo same-day CTC following an incomplete colonoscopy, we are unable to determine the actual number of patients who may have been sent to CTC who did not have the procedure owing to poor bowel preparation, inability to schedule the CTC (such as lack of insurance coverage), had restrictions to CTC, or other unidentified barriers. It is also possible that same-day CTC patients were healthier and thus more likely to be referred for the procedure. This is supported by the fact that the majority of the patients in this study did not have high-risk criteria for CTC perforation, including severe IBD, sigmoid colon cancer, luminal obstruction (except for one patient with a diverticular stricture), elderly age or resection of polyps >20 mm in diameter, but we believe that the study cohort is representative of what most endoscopy units will see in usual practice.6,7 About half the procedures were performed using room air insufflation rather than CO2, so it appears that this was also not a risk factor for CTC-associated complications as confirmed by a recent meta-analysis. 19
Mucosal biopsies and routine polypectomies do not involve the muscularis propria and are thus unlikely to result in perforation. In this study the majority of the polypectomies were performed using a biopsy forceps, but even snare polypectomies of polyps up to 20 mm were not associated with same-day CTC complications. Polyp size was reported by the endoscopist and could have been over-estimated as measurement was not standardized. Different results could be expected for larger polypectomies, especially following endoscopic mucosal resection or submucosal dissection techniques. We currently wait at least a week to perform CTCs in patients who have had complex polypectomies.
A much larger study or a meta-analysis would be needed to show the true incidence of CTC complications, especially perforations, associated with endoscopic biopsies and polypectomies but could require a significant amount of resources and time, may not reach the end-point, and thus may not be practical. 49
This study shows that although radiologists may be apprehensive to perform a CTC the same day as an incomplete colonoscopy with polypectomy, the decision should be tailored to the patient.
This study does not identify risk factors for complications of same-day CTC after an incomplete colonoscopy with tissue sampling but based on published CTC and DCBE outcomes, and until more data are available, we avoid same-day CTC in the presence of a stricture especially when suspected to be malignant; active IBD, especially severe; or after resection of a complex polyp. More studies are needed to understand patient characteristics and risk factors for CTC-related complications, especially colon perforations.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgment
The authors acknowledge Cassandra Yoder, medical student from Florida Atlantic University, for her assistance with the chart review and data gathering during her summer internship.