
Abstract
Extra-oesophageal symptoms of gastro-oesophageal reflux disease (GORD) are often studied, but remain a subject of debate. It has been clearly shown that there is a relationship between the extra-oesophageal symptoms chronic cough, asthma, laryngitis and dental erosion and GORD. Literature is abundant concerning reflux-related cough and reflux-related asthma, but much less is known about reflux-related dental erosions. The prevalence of dental erosion in GORD and vice versa, the prevalence of GORD in patients with dental erosion is high but the exact mechanism of reflux-induced tooth wear erosion is still under review.
Gastro-oesophageal reflux (GOR) disease is very common in the Western world, with a prevalence ranging from 20% to 40% and increasing costs to health care providers. 1 GOR disease (GORD) can be divided into erosive reflux disease, with oesophageal lesions like oesophagitis and even Barrett’s oesophagus, and non-erosive reflux disease (NERD), with the absence of macroscopic lesions in the oesophagus. Typical symptoms of GORD are heartburn and regurgitation, but many extra-oesophageal symptoms (EOSs) have been associated with GORD, although the existence of a causal relationship between GOR and several EOSs still remains controversial. In this issue of United European Gastroenterology Journal, a study by Wilder-Smith et al. characterizes reflux parameters objectively measured by 24-hour pH-impedance monitoring in a large group of patients with dental erosion as EOS of reflux disease. 2
The Montreal classification describes chronic cough, asthma, laryngitis and dental erosions as established extra-oesophageal associations with GORD (Figure 1).
3
The literature is abundant concerning extra-oesophageal respiratory symptoms (EORSs) such as chronic cough and asthma; however, much less is known about the relationship between reflux and dental erosions.
The Montreal classification (adapted from Vakil et al.3).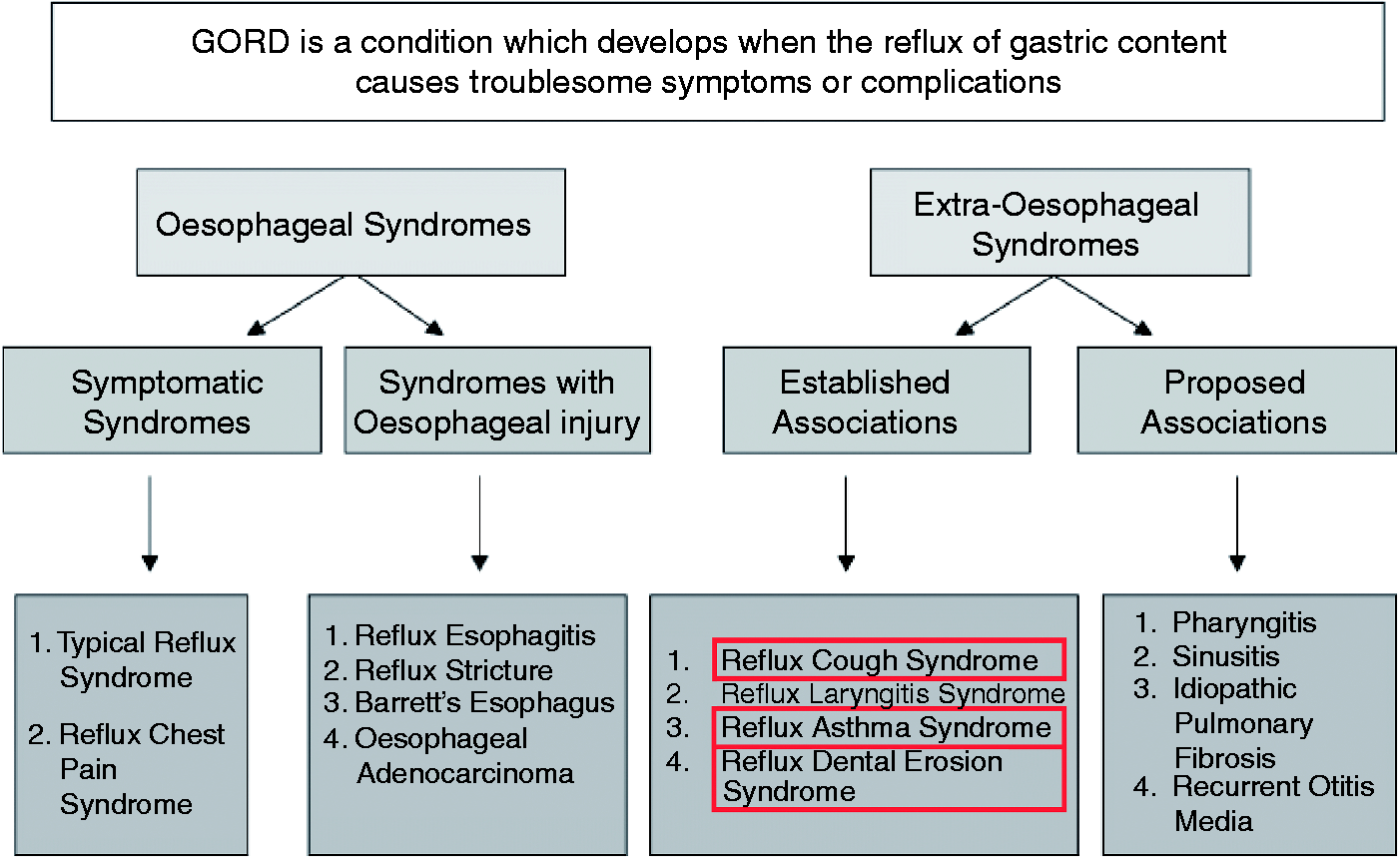
GOR is one of the three most common causes of chronic unexplained cough, besides asthma and post-nasal drip syndrome.4,5 Chronic unexplained cough is defined as a cough that persists for more than eight weeks and it affects roughly 11% to 20% of the adult population. 6 It is common both in erosive (30.5%) as well as non-erosive (34.9%) reflux disease and occurs predominantly during the day, in the upright position, when rising from the bed and with eating.7,8 A study by Poe and Kallay state that GOR is the single causal factor of chronic cough in 13% of their study population, and a contributing factor in 56%. 9 Patients with chronic cough often do not experience typical symptoms of GORD: heartburn and regurgitation occur in approximately 25% of patients with reflux-related cough, which highlights the importance of silent reflux in this population.10,11 There is even less evidence for a relation between the presence of oesophagitis and reflux-related chronic cough: a study by Baldi and colleagues showed that only 15% had endoscopy proven oesophagitis. 12 Objectively measuring reflux parameters using 24-hour pH- or pH-impedance monitoring has a specificity of only 66% in reflux-related cough, and it is of great relevance to mention that presenting with normal reflux parameters does not exclude the existence of a relationship between reflux and cough.4,13–16 Symptom association probability or symptom index can be useful in finding a one-to-one association with cough; however, it is still debatable to what extent these parameters are applicable for EOS. 14
Estimates of prevalence of GORD in asthma range from 30% to 90%. Havemann et al. reviewed 28 epidemiological studies and showed a 59.2% weighted average prevalence of GORD symptoms in asthmatic patients compared with 38.1% in controls. 17 Similar to chronic cough, several studies demonstrated the importance of silent reflux in patients with reflux-related asthma, hence having increased reflux parameters without any signs of heartburn and/or regurgitation.18–20
Dental erosion is the result of a chemical dissolution of the enamel by acids not of bacterial origin. The origin of these acids is often extrinsic, mostly of dietary origin, but they can also be of intrinsic cause, such as vomiting, GOR, regurgitation and rumination. Dental erosions are permanent, potentially disfiguring and occur predominantly in children. When confining to the adult population, the prevalence of dental erosions in GORD patients ranges from 5% to 47.5%, with a mean of 32.5%.21–26 Similar to other EOSs, prevalences are highest when defining GORD on the basis of symptoms and the lowest when using endoscopic criteria.21,25 To date, there has been no study evaluating the relationship between dental erosions and GORD using the gold standard for reflux measurements, namely 24-hour pH-impedance monitoring. This technique allows quantification not only of acid reflux but also of weakly acidic and non-acid reflux, and, importantly, it is possible to measure the proximal extent of reflux, which might be a determining factor in the pathogenesis of reflux-related dental erosions. Wilder-Smith et al. studied a large cohort of 374 patients presenting with dental erosions of which 349 patients underwent a 24-hour pH-impedance monitoring. The majority of patients (73%) reported reflux symptoms less than once a week, but abnormal reflux parameters were found in 69%, suggesting the presence of silent reflux in a large proportion of patients with dental erosions. These data are in line with the Montreal classification. 3 However, less expected was the lack of correlation between the severity of dental erosions and any of the reflux variables. Similar to other EOSs, applying classic GORD parameters might not be the gold standard and the authors state clearly that reflux with pH<5.5 already has an impact on tooth wear erosions.
Nocturnal reflux has been shown to be associated with more severe complications of GORD and with a poor quality of life. Protective mechanisms that are of importance during the waking hours are absent or less active during sleep: saliva production is decreased, there is less voluntary and involuntary swallowing after a reflux episode, gastric emptying is slower and pressure of the upper oesophageal sphincter is decreased during the night. 27 Currently, there are no data available on the role of nocturnal reflux in patients with chronic cough. Young adults with nocturnal reflux symptoms, however, appear to have a higher prevalence of asthma and other respiratory symptoms as compared with patients without any nocturnal reflux symptoms and Moazzez et al. showed that there was a significant correlation between acid reflux on the one hand and the proportion of supine time when pharyngeal pH was below 5.5 on the other and tooth wear erosion.28,29
Acid reflux occurs more in patients with a hiatal hernia, and it has been shown that the size of the hernia is strongly correlated with the degree of oesophagitis. 30 Baldi et al. described the presence of a hiatal hernia in 18% of patients with chronic cough. 12 In patients with asthma, the presence of a hiatal hernia is very common, with a prevalence ranging from 37.1% to 61.7%. 17 In a very recent study by Karamanolis et al., it has been shown that patients with a hiatal hernia were more likely to display nocturnal typical reflux symptoms compared with those without a hiatal hernia. 31 The relationship between a hiatal hernia and nocturnal EOSs of GORD has yet to be evaluated.
The pathophysiology of EOSs of GORD remains poorly understood. So far, two important mechanisms have been implicated in the existence of EORSs: 1) reflux theory = reflux with a high proximal extent with irritation of the pharynx and/or larynx or even micro-aspiration of (duodeno)-gastric contents in the airways; 2) reflex theory = activation of a (vagal) oesophago-respiratory reflex pathway originating from reflux confined to the distal oesophagus. The hypothesis of irritation and/or macro-aspiration remains controversial, and several studies even indicate that a high proximal extent of reflux does not play a major role in the genesis of cough.14,32–34 On the other hand, it has been shown that infusion of acid into the distal oesophagus increases not only the frequency of coughing but also the cough reflux frequency, supporting the reflex theory.10,35
Lately, new techniques have been sought to detect reflux reaching up to the larynx and even pharynx, which is considered to be important in laryngo-pharyngeal reflux. It might, however, also be relevant in patients with chronic cough and asthma, but especially in patients with dental erosion, where acid exposure of the teeth seems to be the trigger. The new Restech device consists of a nasopharyngeal pH catheter, and it has been suggested in uncontrolled studies that is could predict response to both medical as well as surgical therapy. However, a very recent study by Desjardin et al. showed that pharyngeal drops in pH are seldom associated with pharyngeal reflux. 36 This suggest that there is an unmet need for new technologies to detect pharyngeal reflux.
Acid exposure time is considered as the main factor in the pathogenesis of both typical and atypical symptoms and the development of proton pump inhibitors (PPIs), reducing gastric acid secretion, was a major break-through in GORD treatment.37,38 Similar to oesophageal manifestation of GORD, patients with EOSs are often treated with PPIs. To date, there are no studies showing a good gain effect of PPIs above placebo in EORSs. A recent review by Kahrilas et al. could not definitely state a beneficial effect of acid suppressive therapy in patients with chronic cough. 39 However, as excellently marked by the authors, outcome tests used in EOSs are far from perfect. A recent meta-analysis from Chan et al. showed that treatment of asthma patients with PPIs resulted in a small improvement in morning peak expiratory flow; however, there was no overall improvement in lung function or in asthma symptom score. 40 They conclude that PPI treatment in patients with asthma is unlikely to be of meaningful clinical significance. However, a study by Kiljander et al. suggested that a subgroup of asthmatics, in particular those with nocturnal reflux, might benefit from acid suppressive therapy. 41
It has been suggested that intake of antacids is effective in stopping the progression of dental erosions. In a recent study by Wilder-Smith et al. it has been shown that treatment of patients with advanced dental erosions and an abnormal acid exposure with esomeprazole significantly diminished progression of dental tissue demineralization compared with placebo. 42 But, similar to other EOSs, more studies are warranted to investigate the effect of PPIs on the progression of dental erosions.
In conclusion, it is clear that there is an association between several EOSs, amongst others dental erosion and GORD. However, in comparison with other EOSs of GORD, much less is known about the pathophysiology and treatment guidelines of reflux-related dental erosion. The study conducted by Wilder-Smith et al. demonstrates that silent reflux is very important in patients with dental erosion. A second message of this study, and maybe of even more importance, is the lack of correlations between dental erosion scores and reflux parameters, meaning that criteria used in oesophageal symptoms of GORD are not necessarily applicable in EOSs. These data show that there is a high need for further investigations.
Footnotes
Funding
The author receives funding from the Research Foundation – Flanders (FWO – Vlaanderen).