
Abstract
Objectives
This study aimed to resolve controversy regarding the effects of Helicobacter pylori eradication therapy and H. pylori infection in gastro-oesophageal reflux disease.
Design
A randomized, double-blind, multicentre trial was performed in patients presenting with reflux symptoms. H. pylori-positive patients were randomized to receive either antibiotics or placebo for 7 days. H. pylori-negative patient controls received placebo. All received esomeprazole 20 mg b.d. for 7 days, followed by 40 mg o.d. to complete an 8-week course, and were followed up for 32 weeks by telephone.
Results
In this study, 198/589 (34%) patients were H. pylori-positive and 113 H. pylori-negative patients served as controls. Baseline endoscopy revealed 63% Los Angeles grade 0A and 37% Los Angeles grade BCD oesophagitis with no difference between patient groups. Symptom improvement on esomeprazole was seen in 89%. H. pylori eradication was successful in 82%. H. pylori eradication had no effect on symptomatic relapse (hazard ratio 1.15, 95% CI 0.74–1.8; p = 0.5). Overall, H. pylori-positive patients had a lower probability of relapse compared to H. pylori-negative controls (hazard ratio 0.6, 95% CI 0.43–0.85; p = 0.004). Relapse hazard was modulated also by oesophagitis grade (BCD vs. 0A, hazard ratio 2.1, 95% CI 1.5–3.0).
Conclusion
Relapse of gastro-oesophageal reflux disease symptoms after a course of high dose acid suppression took longer for H. pylori-positive patients than H. pylori-negative controls; however eradication therapy had no effect on the risk of relapse; ClincialTrials.gov number, NCT00574925.
Introduction
Gastro-oesophageal reflux disease (GORD) is a common medical problem with a spectrum of symptoms and varying degrees of severity. It is estimated that 20–40% of the adult population experiences heartburn or other symptoms related to reflux and this can impact on quality of life and health costs. 1 Moreover, there is a strong relation between acid reflux and the development of oesophageal adenocarcinoma. 2 These concerns highlight the importance of identifying modifiable risk factors for GORD. One such factor may be gastric Helicobacter pylori infection.
There is an on-going debate about the appropriate management of H. pylori infection in GORD. Many authors recommend H. pylori eradication prior to the initiation of long-term proton pump inhibitor (PPI) therapy because the combination of H. pylori and acid suppression accelerates development of gastric mucosal atrophy and there is some anxiety that this may increase the risk of gastric adenocarcinoma. 3 Other experts caution against this approach,4,5 as most epidemiological studies indicate that reflux symptoms, mucosal disease, and oesophageal cancer are less common in patients with H. pylori infection.5–11 Clinical studies show that acid suppression is more profound and the healing of reflux oesophagitis during treatment with PPIs is more rapid in patients with than in patients without gastric H. pylori infection.12,13 Additionally, two case–control studies report an increased risk of developing GORD after eradication of H. pylori in patients with duodenal ulcer,14,15 although others find no significant effect.16–18 There are concerns, therefore, that treatment of H. pylori infection in GORD patients may exacerbate the disease.
Five prospective controlled trials have studied the effects of H. pylori infection and eradication in patients with GORD.19–23 For patients with reflux symptoms and normal mucosa or grade A oesophagitis on endoscopy, Moayyedi et al. 19 observed no difference in the relapse rate between the antibiotic, placebo, and H. pylori-negative control groups for up to 18 months of follow up. Negative results were reported also by Kuipers et al. 21 in H. pylori-positive patients with reflux oesophagitis. In contrast, Schwizer et al. in a study that recruited patients with all grades of endoscopic findings reported that H. pylori eradication delayed the time to relapse compared to the placebo group and H. pylori-negative controls. 20 These divergent findings are likely due to differences in patient populations or the failure to account for the pattern of gastric infection and inflammation in the H. pylori-positive treatment groups. The latter point may affect clinical outcomes as antral gastritis is associated with increased acid output, whereas corpus gastritis is associated with reduced acid output. 24 Thus, in principle, H. pylori eradication may increase or decrease acid secretion and so the likelihood of acid reflux and related symptoms.
This large, multicentre trial is designed to provide more definitive evidence whether H. pylori infection impacted on the severity or prognosis of GORD and to inform the clinical decision whether to eradicate H. pylori in patients presenting with reflux symptoms. Subjects are stratified according to the presence and grade of reflux oesophagitis at baseline to assess whether the impact of H. pylori eradication, if any, is observed across the spectrum of GORD. Additionally, gastric biopsies obtained before and after treatment assess whether the severity or pattern of gastritis, mucosal thickness, or parietal cell numbers is related to clinical outcome.
Methods
Erastrat is a randomized, controlled, double-blind, multicentre clinical trial of H. pylori eradication therapy in patients presenting with typical reflux symptoms of at least moderate severity as defined by a score of >25 on the Eraflux questionnaire.20,25 Three parallel groups are studied. Patients in the randomized groups were H. pylori-positive and assigned to eradication treatment or placebo. Patients in the non-randomized control group were H. pylori-negative and received placebo. Patients were stratified by endoscopic classification of reflux disease according to the Los Angeles (LA) system. 26
Patient recruitment
A total of 19 hospital- and office-based gastroenterology practices participated in the study, from Austria (n = 2), Germany (n = 10) and Switzerland (n = 7). Patients aged above 18 that met the inclusion criteria were recruited: (i) present with heartburn or acid regurgitation; (ii) at least 8 weeks duration; (iii) at least three times a week; and (iv) with at least moderate intensity, corresponding to mild impairment in daily life and need for medication. Exclusion criteria include history of previous oesophageal or gastric surgery, alcohol or drug abuse, severe organic or psychiatric disease, pregnancy or lactation, women with child-bearing potential without contraceptive measures, allergy or contra-indication to study medications, or need for concomitant medication. Prior knowledge of H. pylori status and previous treatment with PPIs were not exclusion criteria. The trial was approved by ethical committees at each centre and written informed consent was obtained.
Study participants underwent endoscopy. Patients with Barrett oesophagus, malignancy, or peptic ulceration on endoscopy were excluded. Endoscopy and biopsy were repeated at the end of the study. H. pylori status was assessed by a 13 C urea breath test at recruitment and at the end of the study. 27 Gastric biopsies (author MV) and breath test samples (author AL) were forwarded to reference laboratories. Local investigators remained blind to the H. pylori status throughout the study.
Randomization
Computer-controlled inclusion and randomization of patients were operated by an independent study monitor (PharmaPart, Thalwil, Switzerland). Patients that met entry criteria were randomized by a dynamic, centralized procedure that ensured blinding to H. pylori status and treatment group allocation. Probability of rejection was computed such that the projected fraction of patients in each group was constant at each point in time during the study. This system ensured that the appropriate numbers of patients with LA grade 0, AB, or CD oesophagitis on endoscopy were recruited and that a balanced sample of patients was entered at each site.
Patients with evidence of H. pylori infection on 13 C urea breath test were randomized either to the antibiotics group for eradication or placebo (gastric histology was not considered). H. pylori-negative control patients all received placebo. Because of the higher prevalence of H. pylori-negative compared to H. pylori-positive patients, a computerized early random rejection scheme was applied that accepted one-third initially and was dynamically adjusted to ensure balanced recruitment throughout the entire study. Prior to transferring data for analysis, monitors removed all information on drug randomization and H. pylori status from the database.
Study protocol
Once the centralized system had rejected or accepted the patient, the local investigator was informed by fax. If accepted, study medication was dispensed and a central call centre was informed so that telephone interviews could be arranged (no clinical details were transferred). As outlined in the flow chart (Figure 1), patients were contacted by the call centre to assess symptom severity before and after 8 weeks treatment with esomeprazole and subsequently at 2-week intervals until recurrence of reflux symptoms on two subsequent occasions (relapse) or the completion of 32 weeks of follow up. At the end of the study (i.e. relapse or 32-week follow up), the patient underwent repeat endoscopy and
13
C urea breath test. Further management decisions were based on clinical discretion.
Schematic flow chart of Erastrat study procedures.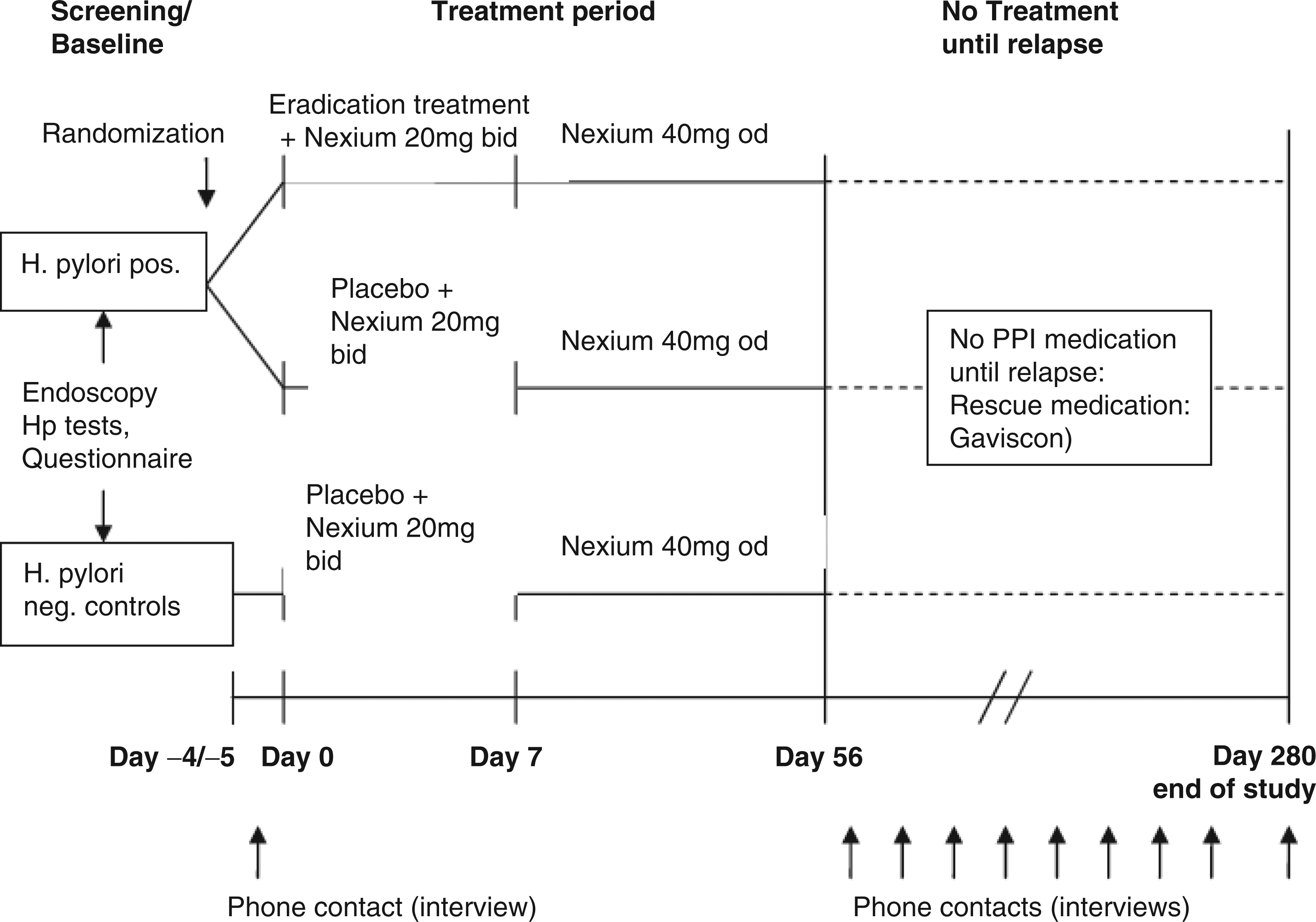
Study medications
For H. pylori eradication, patients were randomized to receive either amoxicillin 1000 mg, and clarithromycin 500 mg, administered twice daily for the first 7 days (antibiotics group), or identical placebo tablets (placebo group). Treatment of GORD with esomeprazole (Nexium; AstraZeneca, Zug, Switzerland) was not randomized. All patients received 20 mg b.d. for 7 days from study start, followed by 40 mg o.d. for 49 days to complete an 8-week course of esomeprazole. This management has been proven effective for H. pylori eradication, 28 oesophagitis healing, and symptom resolution. 29 After acid suppression was withdrawn, patients were provided with an alginate preparation (Gaviscon; Reckitt Benckiser, Slough, UK) as rescue medication for recurrent symptoms.
Symptom assessment
The Eraflux questionnaire measures the frequency, duration, and intensity of reflux symptoms: heartburn, regurgitation, chest or retrosternal pain, and dysphagia. 20 Relapse was defined as recurrence of GORD symptoms to an Eraflux score of 25 at two consecutive interviews. 25 The day of the first interview was taken as date of relapse.
Outcome measures
The primary objective of this study was to assess whether H. pylori eradication treatment extends the time to symptomatic relapse after withdrawal of PPI therapy in patients with a clinical diagnosis of GORD. In addition, the time to relapse in the two H. pylori-positive study groups with the non-randomized H. pylori-negative control group was compared. Data analysis was performed with patients stratified according to oesophagitis grade at inclusion. Secondary objectives were to compare the effect of H. pylori infection and eradication on reflux oesophagitis and to compare the pattern of gastric inflammation and atrophy in the two H. pylori-positive treatment groups with the H. pylori-negative control group at relapse. Outcome data was analysed by ‘intention-to-treat’ (ITT) and ‘as treated’, defined by H. pylori status at relapse or the end of the study (eradicated, non-eradicated, negative control).
Histology
Biopsies were obtained from the oesophagus, gastric antrum, and corpus (midportion at the greater curvature) with standard forceps at recruitment and at the end of the study. Specimens were fixed in 10% neutral buffered formalin and stained with haematoxylin and eosin and Alcian blue periodic Schiff. Histology was assessed by independent investigators (MV, RG) for determination of H. pylori infection, presence of gastritis, mucosal thickness, and density of parietal cells. H. pylori gastritis and mucosal atrophy were graded according to the Sydney System. 30 Histologists were not aware of clinical and endoscopic findings or treatment allocation.
Data analysis
Clinical data was entered manually into an on-line database. Data from early dropouts within the first 8 weeks (i.e. during treatment with esomeprazole) were not used. Data from dropouts during the 32-week follow up (off treatment) are censored to the date of the last telephone interview. Statistics were computed with R. 31 Two-sided tests were used throughout the study; results are reported as significant for p < 0·05. Cross-tabulations were tested with a χ2 test. Cox-proportional hazard regression was used for estimation and comparison of survival curves and to test the effect of covariates. 32 95% confidence intervals (CI) of estimates were calculated. To test the hypothesis that reduced inflammation in the gastric corpus is related to reduced relapse hazard, a three-level variable was defined for each patient, with 0 for no change, 1 for improvement, and −1 for deterioration, and was analysed by a generalized linear model.
Baseline characteristics of patients recruited into Erastrat study
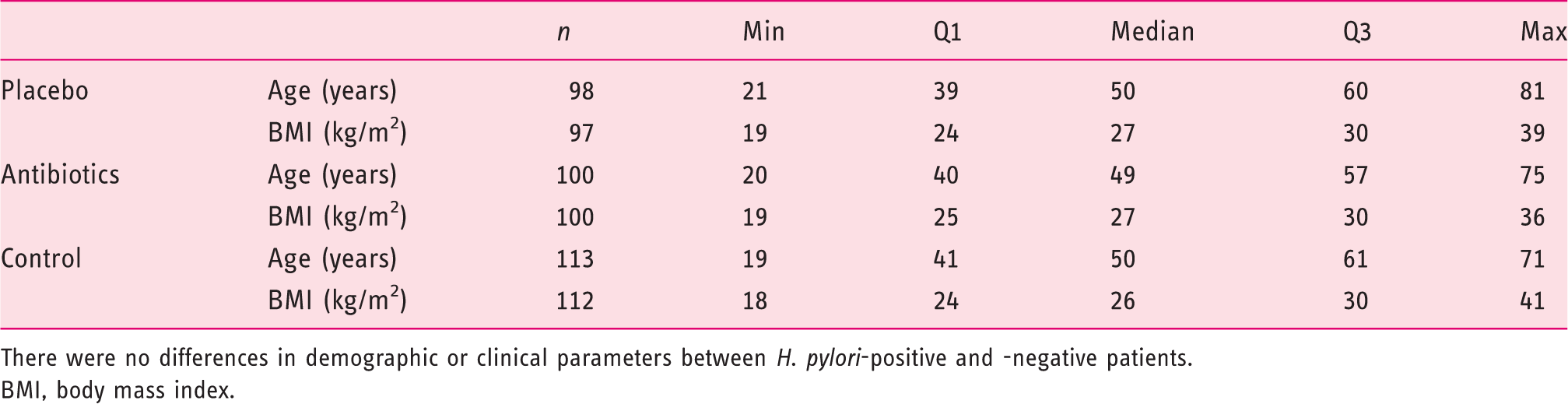
There were no differences in demographic or clinical parameters between H. pylori-positive and -negative patients.
BMI, body mass index.
The sample size was based on a Monte Carlo resampling of the patients enrolled in the Eraflux study. 20 These calculations determined that with 60 patients in each study group and a hazard ratio (HR) of symptomatic relapse of 1.5 between the patient groups, a test power of 0.9 at an type I error rate of 0.05 can be achieved for the primary endpoint. Based on these calculations and allowing for a 40% dropout rate, the study aimed to recruit 318 patients.
Results
This multicentre trial involved eight teaching hospital- and 11 office-based practices or district hospitals. The median number of patients assessed and recruited per type of centre was 18 and 10 patients, respectively. When terminated because of time constraints, 589 patients had been assessed of whom 581 were eligible. After randomized exclusion of excess H. pylori-negative patients, 311 were recruited (62% from office-based practices or district hospitals).
Study population
The baseline statistics of 311 patients included in the ITT analysis are in Table 1. In the study, 169 females and 142 males (54 and 46%) participated.Median age was 50 years (range 19–81), and six patients were older than 70 years. At study entry, endoscopy revealed LA grade 0 (41%, n = 127), A (23%, n = 71), B (25%, n = 77), and CD (11%, n = 36) reflux oesophagitis.
Patient progression
Of 581 eligible patients, 198 (34%) were H. pylori-positive on
13
C urea breath test. Of 383 H. pylori-negative patients, 113 were randomly selected to serve as controls. The progress of the 311 patients recruited through the Erastrat study is detailed in Figure 2. Initial treatment with 8-week esomeprazole did not improve reflux symptoms in 35 (11%) patients. There was no indication that the likelihood of treatment failure was influenced by oesophagitis grade, baseline H. pylori status or allocation to study treatment. Adverse events were reported by 76 patients (antibiotics 25, placebo 23, control 28), leading to the withdrawal of 20 patients. Of these 13 were considered due to the study medication, most commonly nausea or diarrhoea during H. pylori eradication therapy. Following withdrawal of esomeprazole, in the 223 patients that had an initial response to acid suppression and continued in the study, symptomatic relapse was reported by 134 patients (60%) during the 32-week follow-up period. The success of H. pylori eradication was 82% by
13
C urea breath test at time of relapse or at 32-week follow up. At the end of the study (as treated), 84 patients were H. pylori-positive (placebo and failed eradication), 55 were H. pylori-negative (successful eradication), and 59 were H. pylori-negative controls.
CONSORT diagram of Erastrat study: ITT analysis.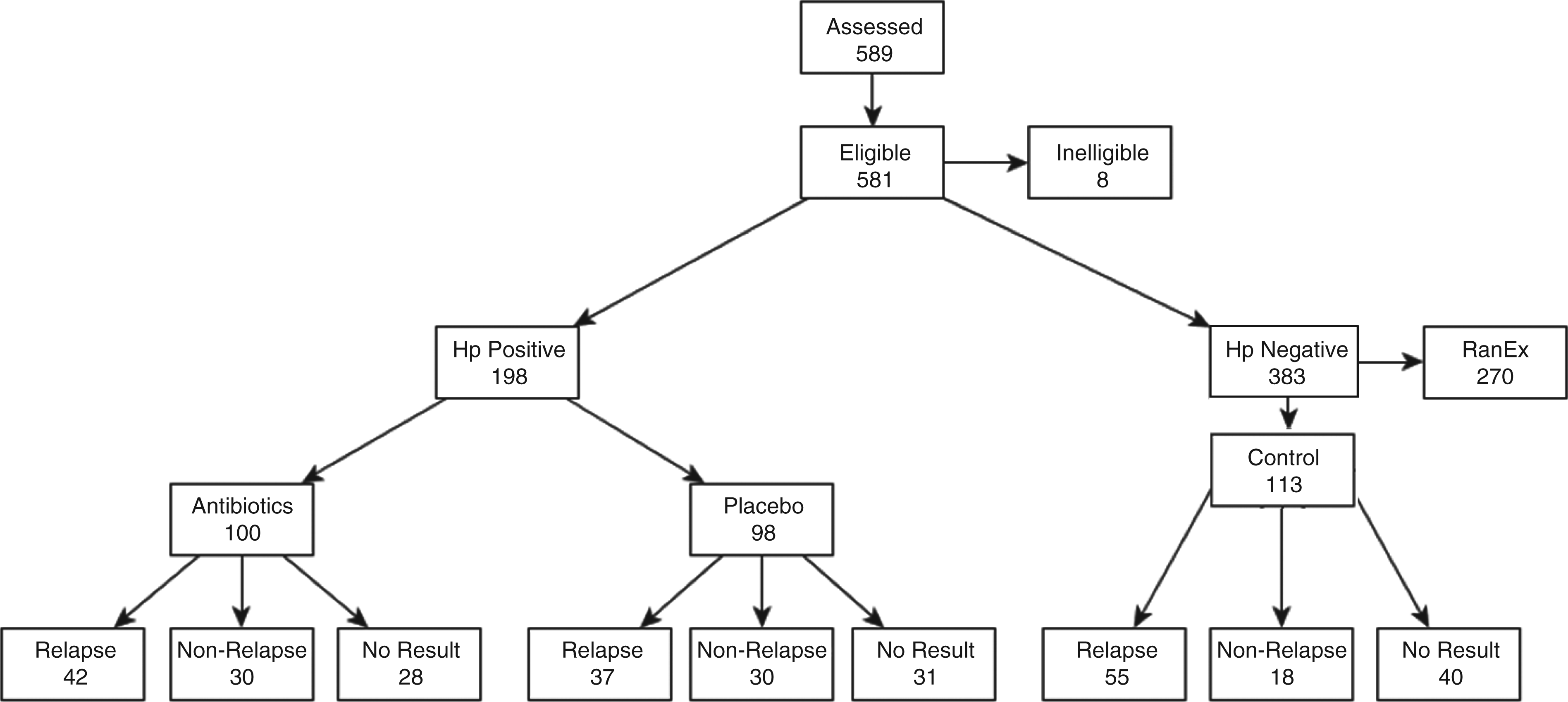
Effect of H. pylori status and eradication therapy on relapse of reflux symptoms
Patients in the two H. pylori-positive groups had a similar rate of relapse at 32-week follow up (Figure 3). H. pylori eradication therapy had no effect on relapse hazard during the 32-week follow up (HR antibiotic vs. placebo 1.15, 95% CI 0.74–1.8; p = 0.5). H. pylori-positive patients, treated by antibiotics or placebo, had a lower probability of relapse compared to the H. pylori-negative control group (HR 0.6, 95% CI 0.43–0.85; p = 0.004). Subgroup analysis showed that the non-randomized H. pylori-negative control group had an increased risk of relapse compared to both H. pylori-positive groups (HR against placebo 1.79, 95% CI 1.18–2.70; against antibiotics 1.54, 95% CI 1.03–2.33). This result is not altered by correction for age and sex. Time to relapse from the smaller as-treated subset of patients is not different from that of the ITT subset.
Cox regression.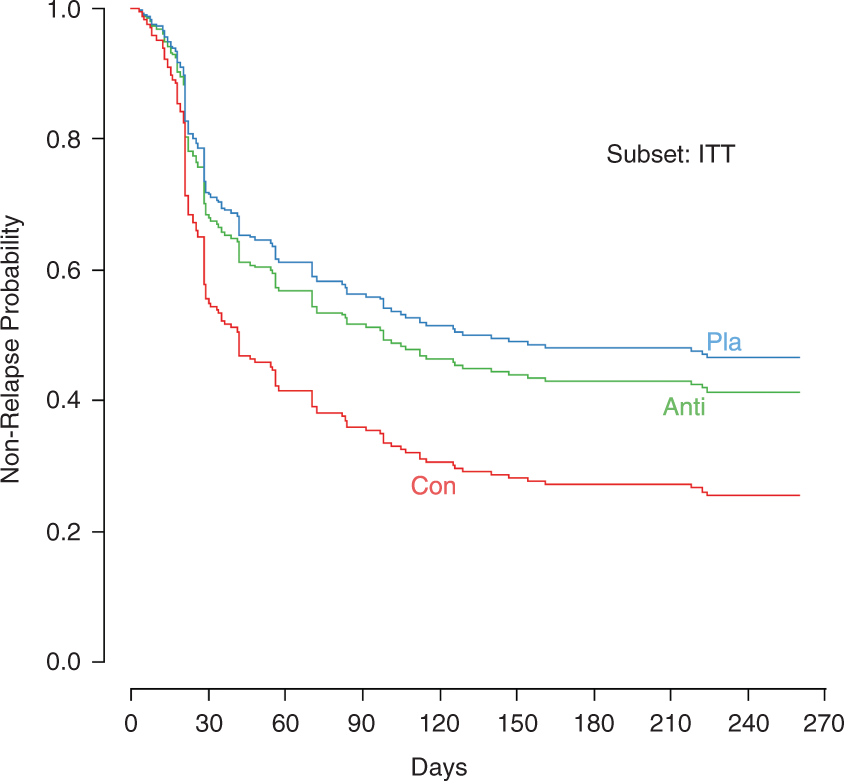
Effect of oesophagitis status on relapse of reflux symptoms
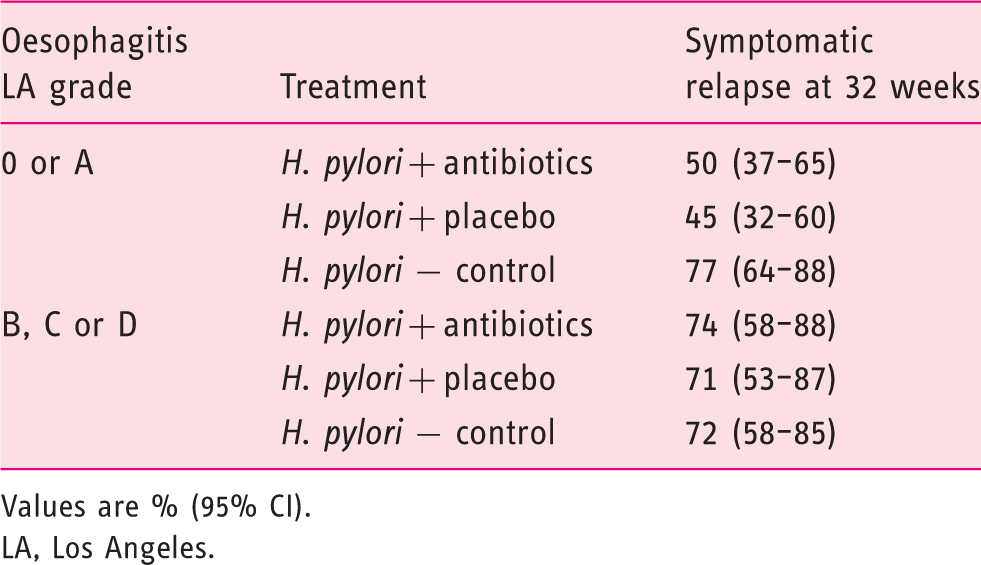
Stratification of time to relapse analysis by endosopic findings reveals two distinct patterns (Figure 4, Table 2).: All patients in the H. pylori-negative control group and patients with moderate-severe oesophagitis (LA grade BCD) had a probability of relapse at 32 weeks of 71% or above. In contrast, irrespective of eradication (p = 0.6), H. pylori-positive patients without oesophagitis or with mild oesophagitis (grade A) had 50 and 45% probability of relapse, respectively (Table 2). The HR for relapse between patients with oesophagitis BCD compared to 0A was 2.1 (95% CI 1.5–3.0). Increased time to relapse in non-eradicated H. pylori-positive compared to H. pylori-negative controls was observed for patients with LA OA (HR 0.41, 95% CI 0.23–0.71; p = 0.002), but not those with LA BCD (HR 0.97, 95% CI 0.52–1.80).
Cox regression stratified according to endoscopic findings. Probability of relapse at 32 weeks by degree of oesophagitis and patient group Values are % (95% CI). LA, Los Angeles.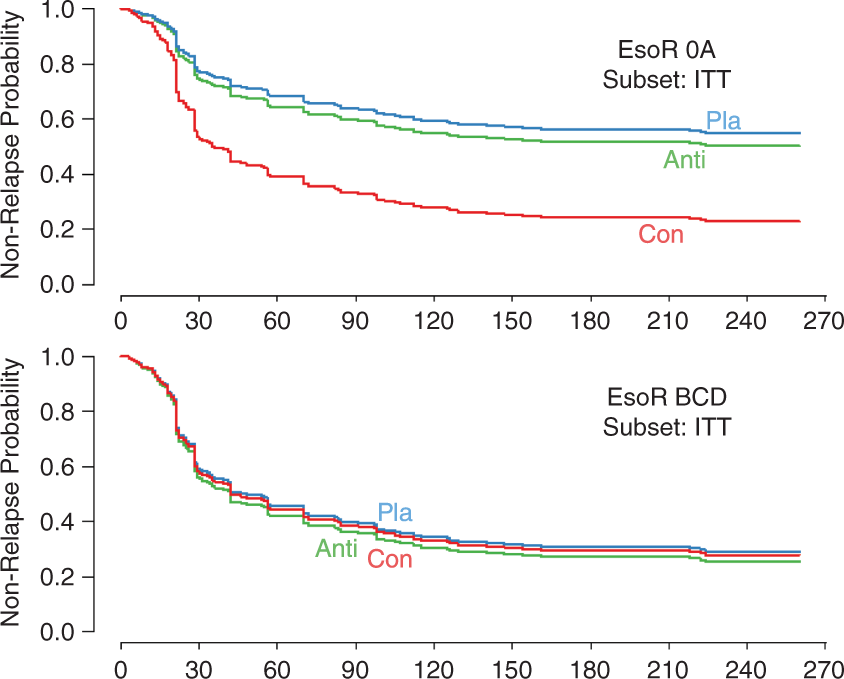
In the patient group with oesophagitis, repeat endoscopy at the end of the study revealed that LA grade had improved for 59 (34%), deteriorated for 22 (13%) patients, and was unchanged for 91 patients (53%). The improvement was greater in the patients with severe reflux oesophagitis. Comparing patients with and without a symptomatic relapse, those that remained symptom free tended to have a greater improvement in oesophagitis grade at the end of the study (p = 0.089).
Histology
All 311 patients enrolled into the study had biopsies obtained from the oesophagus, gastric antrum and gastric corpus at baseline, and 173 (56%) had histology samples also taken at the end of the study.
Oesophageal histology reveals no difference at baseline between H. pylori-positive and -negative patients in terms of inflammation, dilated intracellular spaces, length of regenerative papillae, or thickness of the basement membrane (all p > 0.1). Neutrophilic (p = 0.093) and eosinophilic (p = 0.011) infiltration increased with severity of reflux oesophagitis. Oesophageal histology did not predict primary treatment outcome (i.e. response of reflux symptoms to 8 weeks of esomeprazole treatment).
At baseline moderate or marked gastritis defined by the Sydney Classification was much more prevalent in H. pylori-infected patients than in H. pylori-negative controls (143/198, 72%, vs. 4/103, 4%; p < 0.0001) and the gastric mucosa was thicker (difference 130.9 µm, 95% CI 27.2–158.1 µm; p = 0.0063). There was no difference in the number of parietal cells per high-powered field (hpf) between H. pylori-positive and -negative patients (difference 5.3/hpf, 95% CI −1.9 to 3.4/hpf; p = 0.56). After successful H. pylori eradication and 8 weeks of esomeprazole, the number of patients with moderate or marked gastritis fell from 77% to none, whereas 66% had persistent gastritis in those H. pylori-positive patients that either failed eradication or received placebo (p < 0.001). There was a trend between the improvement in gastritis following H. pylori eradication and the risk of symptomatic relapse (p = 0.09) but there was no evidence that the number of parietal cells per high-powered field is a predictor of relapse (p = 0.39)
Discussion
This large, multicentre trial evaluated the effect of H. pylori infection and eradication on reflux symptoms and endoscopic findings in patients presenting with symptoms of GORD. Patients received H. pylori eradication therapy or placebo with esomeprazole followed by 8 weeks of PPI therapy using methodology of proven efficacy,28,29 which is consistent also with guidelines for treatment of these conditions.1,34 At the end of this treatment period, effective relief of reflux symptoms was achieved in 89% of patients and a repeat 13 C urea breath test confirmed successful H. pylori eradication in 82%, both consistent with previous reports from similar populations.28,29 The primary outcome of the randomized controlled trial is that H. pylori eradication therapy has no effect on the relapse hazard (i.e. cumulative probability of relapse) for reflux symptoms during 32 weeks of follow up after withdrawal of acid suppression (Figure 3). The risk of symptomatic relapse is reported as 50 and 45% in the antibiotic and placebo groups, respectively, with no difference between groups (HR 1.15, 95% CI 0.74–1.8; p = 0.5). This result was not altered by correction for age, sex, or other potential confounding factors included in the analysis.
Important additional information was obtained when patients were stratified according to grade of oesophagitis (Figure 4). For patients with endoscopy-negative reflux disease or mild oesophagitis (grade 0 or A, n = 196), the relapse hazard in the H. pylori-negative control group was significantly greater than that of the eradicated patients (HR 2.13, 95% CI 1.23–3.70; p = 0.006), with a relapse hazard at 32 weeks of 77 and 50%, respectively. Whereas for patients with moderate to severe oesophagitis (grade B, C, or D, n = 115), symptomatic relapse was rapid and H. pylori status had no effect on relapse hazard (HR 0.93, 95% CI 0.52–1.69; p = 0.8). The findings were not altered by H. pylori eradication in either subgroup. Thus, the presence of H. pylori infection prolongs the time to symptomatic relapse in patients with absent or mild endoscopic disease, but other factors, likely related to disruption of the oesophago-gastric junction and high levels of oesophageal acid exposure, 1 determine the natural history of disease in patients with more severe reflux oesophagitis.
These findings are in agreement with epidemiological reports that the risk of reflux symptoms and mucosal disease is reduced in H. pylori-positive patients. Raghunath et al. 9 undertook a systematic review of 20 studies including more than 4000 patients and found that the odds ratio for H. pylori prevalence in GORD patients was 0.60 (95% CI 0.47–0.78). However, the results differ from previous randomized controlled trials which report little or no difference in time to relapse between the H. pylori-positive and –negative groups.19,20 The current study had a similar design but important strengths. First, a much larger study population. Second, inclusion of patients across the spectrum of GORD allowed stratification of results with severity of oesophagitis. Third, recruitment of patients with typical reflux symptoms from multiple centres, with the majority from office-based practices and district hospitals. Patients presenting to tertiary care have a high rate of somatization and psychosocial morbidity and these factors may be more closely related to treatment outcomes than disease activity. 35 The excellent response (∼90%) to initial PPI therapy and the high ‘ongoing remission’ rate at 32 weeks (∼50%) off medication in the current study is higher than that reported by previous randomized controlled trials based in tertiary care and may be more representative of those sampled in epidemiological and community-based studies in which similar effects of H. pylori infection in GORD were found.
The biological mechanism underlying the relatively rapid relapse of reflux symptoms in H. pylori-negative controls compared to H. pylori-positive patients is not established. One explanation for the ‘protective’ effect of H. pylori infection in GORD is persistent reduction in gastric acid secretion. Rebound acid hypersecretion and reflux symptoms have been reported in healthy H. pylori-negative subjects and also H. pylori-negative reflux patients after discontinuation of omeprazole;36,37 in contrast, many H. pylori-positive patients show persistent acid suppression after eradication. 36 Direct measurements of acid secretion were not performed; however, the results are consistent with these observations. H. pylori status has no effect on the success of initial PPI therapy and yet, during 32 weeks of follow up after withdrawal of acid suppression, H. pylori-negative patients have a higher risk of relapse than H. pylori-positive patients irrespective of allocation to eradication therapy or placebo. Histology shows a dramatic improvement in gastritis in H. pylori-positive patients following successful eradication therapy and resolution of corpus inflammation is associated with a trend to symptomatic relapse. Over time, recovery of acid-secreting capacity may occur in patients with gastric mucosal atrophy as parietal cell mass recovers;38,39 however, in this study, very few H. pylori-positive patients had mucosal atrophy and there was no difference in mucosal thickness or parietal cell numbers between H. pylori-positive and -negative patients at baseline or at the end of the study. These results imply that the reduction in acid secretion with H. pylori infection is caused by other mechanisms; for example, downregulation of parietal cell H,K-ATPase expression in gastric mucosa by H. pylori cag gene products that significantly inhibiting acid secretion.40,41
The study population was under 70 years old. It is possible that results may be different in an older population with a greater proportion of gastric atrophy, and also in specific patient groups, such as those with duodenal ulcer14,15 and with strains of H. pylori infection or host inflammatory responses (e.g. interleukin 1β) that powerfully inhibit acid secretion. 42 Patients were diagnosed and recruited on the basis of typical reflux symptoms rather than ambulatory pH-impedance monitoring; however, symptom-based diagnosis and the response to therapeutic trials are considered acceptable surrogates in most clinical settings. 34 Overall, slightly less patients entered the study than planned (311/318, 98%); however, sufficient numbers were attained for a robust ITT analysis of primary and secondary endpoints. Nevertheless, it should be noted that the confidence intervals of the ITT analysis are fairly wide, thus a small effect of eradication therapy on treatment outcome cannot be excluded or could become apparent with longer follow up. Findings from the as-treated analysis were not qualitatively different; however, the differences between groups were less pronounced because repeat 13 C breath tests and gastric histology were available for only 56% of the total study population. Incomplete data collection also reduced the statistical power to determine the effects of changes in histological biomarkers following H. pylori eradication on relapse hazard.
In conclusion, H. pylori eradication therapy has no impact on the success of PPI therapy for GORD or the risk of symptomatic relapse after withdrawal of acid suppression. Instead, the presence of H. pylori infection at study entry decreases the risk of symptomatic relapse, especially in patients with absent or mild mucosal disease. This is the first time that the protective effect of H. pylori infection in GORD described by epidemiologists has been demonstrated in a prospective, clinical study.
These findings have direct implications for practice. Clinicians and patients can be reassured that the short- to mid-term management of GORD patients can be focused on symptom control, independent of the decision to investigate and treat H. pylori infection. Indeed, it will often be easier to discontinue PPI therapy in reflux patients with H. pylori infection. If long-term PPI therapy is required, then H. pylori infection can be identified and eradication therapy prescribed; however, again, this can be performed without undue concern that this will exacerbate GORD symptoms or mucosal disease.
Footnotes
Acknowledgements
We are grateful for the Clinical Monitoring Services of A Schwarz at PharmaPart, Thalwil, Switzerland and for the excellent work of study nurses B Stutz and R Eisenring at the telephone follow-up centre at the University Hospital of Zürich.
In addition to authors, the following were participating investigators: Switzerland: H Frühauf (University Hospital, Zurich), P Netzer (Inselspital, Bern), M Essig (Bezirksspital, Zweisimmen), H Schlauri (Wil); Germany: E Bästlein (Köln), M Buchner (Ribnitz), C Haferland (Görlitz), T Simon and B Cyrus (München), E Meier (Amberg), R Vogt (Mannheim), M Neumeyer (Oldenburg), J Habbig and D Klein (Köln), J Zeus and J Schenk (Erlangen); Austria: G Brandstätter (Landeskrankenhaus, Graz-West).
Funding
This research was sponsored by AstraZeneca, the makers of esomeprazole (study code D9612L00201).
Conflict of interest
The authors declare that there is no conflict of interest.
Clinical Trial registration
NCT00574925