
Abstract
Background
Inflammatory conditions affecting the gut may cause motility disturbances, and ulcerative colitis – one of the main disorders among the inflammatory bowel diseases – may display abnormal colonic motility.
Aim
To review the abnormalities of the large bowel in ulcerative colitis, by considering the motility, laboratory (in vitro) and pathological studies dealing with this topic.
Methods
A comprehensive online search of Medline and the Science Citation Index was carried out.
Results
Patients with ulcerative colitis frequently display colonic motor abnormalities, including lack of contractility, an increase of propulsive contractile waves, an excessive production of nitric oxide, vasoactive intestinal polypeptide nerves, interleukin 1 beta, neurotensin, tachykinins levels and the weaker action of substance P, likely related to a neuromuscular dysfunction due to the inflammatory process.
Conclusions
A better understanding of the pathophysiological grounds of altered colonic motility in ulcerative colitis may lead to a more in-depth knowledge of the accompanying symptoms and to better and more targeted therapeutic approaches.
Introduction
Defecation, that is, the expulsion through the anus of the residual contents following digestive processes, is a physiological phenomenon for all human beings. 1 This complex function is under strict voluntary control, involves appropriate neuromuscular circuitries, and it grants an effective elimination of the faecal matter. 1
Colonic motility displays a circadian trend, and it is mostly present during daylight hours, with significant peaks after morning awakening, sudden awakening and after meals. 2 In healthy individuals, the colon receives semi-solid contents from the terminal ileum and, by means of both segmentation (also helped by the peculiar anatomic aspect represented by the haustrae) and propulsion, it compacts and propels these contents aborally.1,2 Colonic propulsion is mainly represented by two kind of waves: the so-called high-amplitude propagated contractions (HAPC, 2 the manometric equivalent of the mass movements described by radiological means at the beginning of the last century) that mainly move large quantities of solid contents aborally and start the defecatory reflexes, 2 and the low-amplitude propagated contractions (LAPC), whose function is principally devoted to the transport of liquid contents and gas, and which is associated with the emission of flatus and is often elicited by colonic distension.2,3
Once the colonic contents reaches the rectum, the distension of the rectal ampulla and the sampling reflex of the anal sphincter send the relevant stimuli to the subject’s brain and, if socially appropriate, he/she will decide whether to evacuate. 2
All the above functions may be altered or disrupted by inflammatory conditions of the gut, of both low- and high-grade intensity.4,5 Thus, it is not surprising that colonic motility is more or less deranged in ulcerative colitis (UC), a pathological condition characterised by different degrees of inflammation of the colonic mucosa that may be limited to the rectum or extend proximally and develop into pancolitis. 6
Colonic motility studies in UC patients
Methods
We conducted a comprehensive online search of Medline and the Science Citation Index using the keywords ‘colon’, ‘colitis’, ‘dysmotility’, ‘enteric nervous system’, ‘inflammatory bowel disease’, ‘large bowel’, ‘motility’, ‘motor activity’, ‘myenteric plexus’ and ‘ulcerative colitis’ in different combinations with the Boolean operators ‘and’, ‘or’ and ‘not’. We primarily included articles that related to human studies. Articles on experimental animal models were considered only when relevant, to strengthen concepts. We performed manual cross-referencing, and selected articles published in English between January 1965 and February 2014. However, a search of non-English language articles and among journals older than 1965 was also performed in our library. Letters were excluded, and abstracts were reviewed only when the full papers were unavailable.
Colonic motor abnormalities in UC: early motility studies
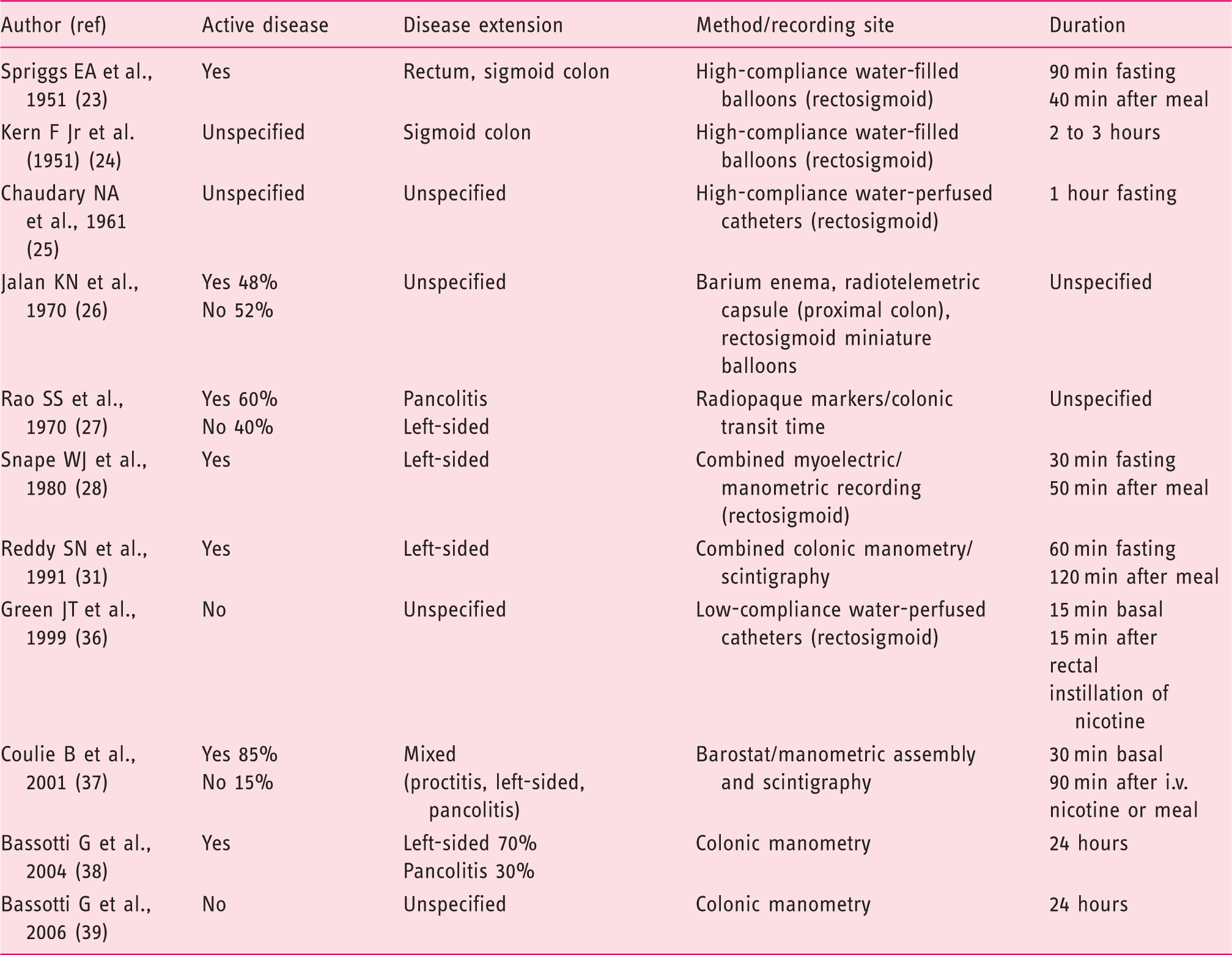
The first studies on this topic were carried out for short time periods in the rectal or rectosigmoid area, mostly with suboptimal techniques such as high-compliance water-filled balloons or perfused catheters. These studies reported that UC patients usually display decreased up to absent motor activity,7–9 sometimes accompanied by low-amplitude propulsive waves. Thus, similar to what happens for other conditions characterised by diarrhoea, the authors hypothesised that their findings might justify the acceleration of intestinal transit often found in these patients through a mechanism involving loss of colonic haustration and decreased resistance to the flow of contents (‘paradoxical motility’).
Later on, a combined radiological–radiotelemetric study reported proximal faecal stasis and decreased motor activity in the proximal colon in a subgroup of patients, suggesting that multiple mechanisms may play a role, 10 However, this study included miscellaneous and poorly defined subjects, and the motor aspects were investigated mostly by barium enema, with radiotelemetry (to investigate proximal motility) being carried out in a smaller (8/399) subgroup of patients, and pressure studies (to investigate distal motility) in another smaller (5/399) subgroup.
A subsequent transit study carried out with radiopaque markers revealed that, in comparison to controls, mouth-to-cecum transit was significantly slower in UC patients with both active and quiescent disease. Patients with active colitis also displayed proximal colonic stasis with rapid transit across the rectosigmoid area, whereas those with quiescent colitis had normal transit. 11
A combined rectosigmoid myoelectric/manometric study showed that UC patients maintained an intact colonic smooth muscle slow wave activity, whereas the colonic contractile response to eating was abnormally decreased (actually, no motor response was present) despite an initial transient increase of post-prandial myoelectrical rapid spiking response. The authors concluded that this lack of colonic contractility, by a paradoxical mechanism of inhibited motility, contributes to the increase in diarrhoea that occurs in these patients after eating. 12 By means of in vitro studies (see also below), this decreased response was thought by the same group to be caused by an abnormality in the intrinsic contractile mechanism of colonic smooth muscle, consisting in either a defect in electromechanical coupling or an inability of the smooth muscle to contract fully. 13
Colonic motor abnormalities in UC: prolonged motility studies
The introduction of prolonged recordings of colonic motility, even in proximal segments of the large bowel, allowed a better definition of the various colonic motor patterns in both the basal state and after food ingestion. 14 Thus, it was possible to obtain data in pathological conditions as well.
In a study comparing colonic motility and transit (by a combined manometric/scintigraphic technique) in healthy volunteers and UC patients, Reddy et al. showed that controls displayed a post-prandial increase in motility that was significantly higher in the descending colon than in other colonic segments. In UC, motility was reduced in all regions compared with healthy subjects, with no significant pressure gradient among different regions. In controls, transit was quiescent during fasting, and eating stimulated both antegrade and retrograde propulsion. In UC, transit was variable before as well as after the meal, with more rapid emptying from the splenic flexure into the sigmoid than into the transverse colon observed in both groups. Low-amplitude, post-prandial propagating contractions occurred more frequently in UC than in controls, had always antegrade direction and caused a rapid shift of the tracer into the sigmoid colon. 15 The authors concluded that these findings might accentuate the diarrhoea in UC. Interestingly, similar motility findings (including overall decrease of colonic motor activity and an increase of propulsive contractile waves) were reported in a canine model of acute colitis mimicking UC.16,17
Since there is some evidence that UC is less prevalent in smokers, a possible role for nicotine as anti-inflammatory agent in this condition has been postulated. 18 Therefore, it is not surprising that investigations also appeared concerning the possible effects of nicotine on colonic motor activity in these subjects. A first study carried out (but only in the rectosigmoid area) in patients with UC in remission did not show significant differences between patients and controls with respect to motility and smooth muscle tone. These variables were reduced in both groups by rectal instillation of nicotine (1.2 mg in 20 mL saline at pH 4.5). 19 Another study, performed in the descending colon by a combined motility/barostat technique in patients with active UC, showed an increased fasting colonic motility and a decreased response to a meal, but not differences in colonic compliance compared with controls. Low-dose nicotine, at a dose mimicking a transdermal patch, did not affect colonic motor activity in UC patients. 20
Subsequent studies investigated colonic motility in UC patients for prolonged (24 hours) periods. In a first study, it was shown that patients with moderate disease display an overall increased propulsive (of both high- and low-amplitude) activity compared with controls, and similar to that found in diarrhoea-predominant irritable bowel syndrome patients. 21 In another study carried out in patients with UC in remission, no differences were found between patients and controls with respect to high-amplitude propulsion and the response to ingestion of a meal, whereas there was a significant increase of low-amplitude propulsive activity in patients. 22
Colonic motor abnormalities in UC: in vitro studies
There have been several laboratory investigations carried out in patients with UC that provide evidence that numerous mechanisms may be responsible for the colonic abnormal function described in these patients. For instance, a series of studies evaluating colonic function in vitro showed that an excessive production of nitric oxide (NO) by a NO-synthase, induced by inflammatory stimuli, may be involved in the mucosal vasodilatation and increased vascular permeability of active UC,23,24 and could also contribute to the impaired motility that accompanies toxic dilation of the large bowel. 25 Moreover, since NO has been shown to be a neurotransmitter in the non-adrenergic non-cholinergic (NANC) inhibitory nerves of the human gut, some authors investigated the enteric nerve responses of colonic tissues from UC patients and showed that both NO and NANC inhibitory nerves play an important role in the impaired motility observed in UC patients.26,27 This impairment might also be enforced by the increase of vasoactive intestinal polypeptide nerves and the weaker action of substance P and neurotensin nerves in UC colons compared with controls. 28 Another study investigated the effect of tachykinins. These substances exert gut contractile effects of similar strength as acetylcholine, predominantly through activation of neurokinin 2 receptors. These responses were greatly reduced in colonic strips from patients with UC,29,30 suggesting that tachykinins probably play a role in the neuromuscular dysfunction leading to colonic dysmotility in these patients. This dysfunction may be enforced by the reduction of intracellular calcium stores mediated by hydrogen peroxide. 31 In addition, interleukin-1 beta levels were increased in colonic circular muscles, and the authors hypothesised that these findings may contribute to motor dysfunction in UC. 32 An increase of motilin receptors in colonic smooth muscle of UC patients has also been reported, 33 although its significance in the colonic motor dysfunction is uncertain.
Colonic motor abnormalities in UC: studies on full-thickness specimens
The abnormalities of colonic motility documented in UC patients have also been studied from a pathological point of view, with the purpose of providing some organic ground to the above-reported motor disfunctions. Indeed, the fact that UC patients sometimes undergo mayor colonic surgery has often provided the researches with surgical (i.e. full-thickness) specimens that represent an optimal substrate to document possible neuromuscular colonic alterations. 34
Electron microscopic studies, for instance, revealed that in patients with severe UC, ultra-structural abnormalities of the pacemaker cells – the so-called interstitial cells of Cajal (ICC) – are present in the sub-muscular pacemaker region 35 and the myenteric area 36 of the colon. Subsequent immunohistochemical investigations documented that, compared with controls, colonic specimens of UC patients express cyclo-oxygenase 2 in the myenteric neurons, suggesting that this expression, through an increased prostaglandin synthesis at this site, may contribute to the dysmotilty seen in this condition. 37 The motility disturbances of UC have been also variably related to an increased number of mast cells and nerves containing inflammatory mediators, 38 to remodelling of the chemical codes (from mainly cholinergic to more substance P-positive) of the myenteric neurons, 39 to down-regulation of proteins involved in smooth-muscle contractility, 40 to abnormalities of the main cell populations (neurons, glial cells) of the enteric nervous system,41,42 the latter associated or not to the presence of myenteric plexitis, 43 and to the strict interactions between eosinophils and nerve fibres of the large bowel. 44
Concluding remarks
Colonic motor activity is frequently abnormal in patients with UC, even when the inflammatory process is mild or moderate. Overall, the available data suggest that an active disease leads to rapid transit and increased propulsive activity, probably due to the failure to absorb salt and water 45 and to the mucosal inflammatory condition which increases the intraluminal load of the large bowel. This in turn, by distending the bowel wall, may elicit colonic propulsion. 3
Although the gross motor abnormalities may be easily documented, the pathophysiological mechanisms responsible for these abnormalities still remain unclear due to the complexity of the physiological mechanisms involved in the control of large bowel motility. However, it is increasing clear, as also observed in other pathological conditions (e.g. irritable bowel syndrome, colonic diverticular disease), that even low-grade inflammation may cause colonic motor neuromuscular dysfunction,46,47 and that specific cell subtypes (e.g. the enteric glial cells) may play important roles in this setting. 48 This and other observations may be important for a better knowledge of the complex pathophysiological aspects underlying the symptoms, in particular diarrhoea, complained of by patients with UC. This better knowledge might also be useful in the future to search for more targeted therapeutic approaches to this condition.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgements
GB ideated the project and wrote the draft of the manuscript. EA, VV, MB and MPD contributed for important intellectual concepts and reviewed the text. All authors reviewed and approved the final form of the manuscript.