
Abstract
Background
Current treatment of Helicobacter pylori consists of three or four drugs for 7–14 days with important associated cost and adverse events.
Aims
This study compared efficacy and safety of standard dose vs. half-dose concomitant nonbismuth quadruple therapy (NBQT) for 7 days. The standard dose consisted of twice daily rabeprazole 20 mg, amoxicillin 1 g, metronidazole 500 mg, and clarithromycin 500 mg.
Methods
This was a prospective randomized trial. 14C-urea breath test was performed ≥4 weeks after treatment and ≥2 weeks off acid suppressive therapy. Compliance and adverse events were monitored during treatment.
Results
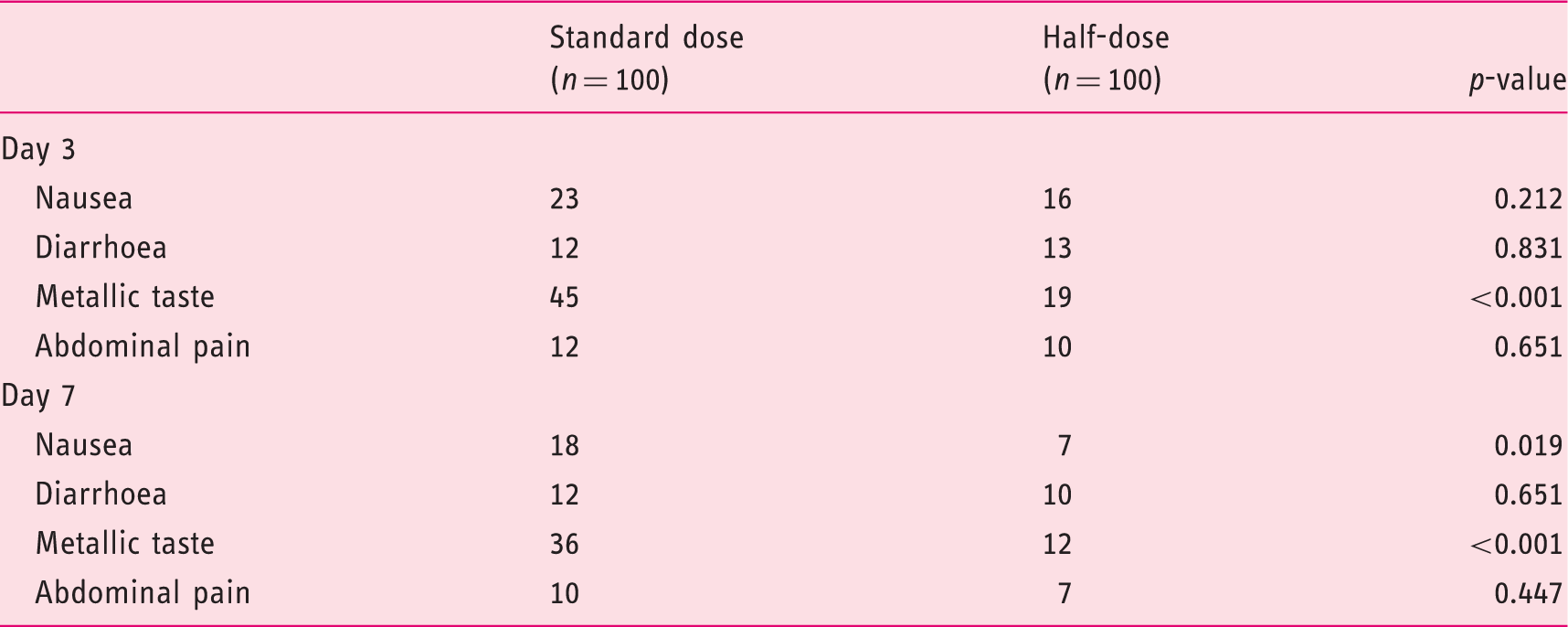
A total of 200 consecutive treatment-naïve patients were enrolled. Baseline characteristics were similar between groups, with 15.5% of subjects reporting prior macrolide use. Eradication occurred in 78% (95% CI 68.6–85.7%) in both groups on intention-to-treat analysis. Per-protocol rates were 82.1 vs. 83.9% for standard-dose patients vs. half-dose patients, respectively (p = NS). Adverse events (only mild) were reported in 57 vs. 41% of standard-dose patients vs. half-dose patients (p = 0.024), with metallic taste and nausea notably less frequent in the latter (36 vs. 12% and 18 vs. 7%, respectively; p < 0.05 for both). Overall, eradication failed in 38.7% of prior macrolide users vs. 18.9% without such exposure (p = 0.019). On multivariate logistic regression, prior macrolide exposure was the only factor associated with failed eradication (OR 2.60, 95% CI 1.06–6.39; p = 0.038). Treatment was cheaper with the half-dose regimen.
Interpretation
A 50% reduction in antibiotic dosage does not diminish efficacy of concomitant nonbismuth quadruple therapy but leads to significant reduction in cost and adverse events. Seven-day concomitant NBQT is suboptimal for H. pylori independent of prior macrolide exposure.
Introduction
Helicobacter pylori is a common infection worldwide, particularly in developing countries. 1 H. pylori infection is associated with chronic gastritis, peptic ulcer disease, and gastric adenocarcinoma and non-Hodgkin's mucosa-associated lymphoid tissue lymphoma of the stomach.2,3 Eradication of this organism has been shown to improve gastric inflammation, accelerate ulcer healing, eliminate ulcer diathesis, and even reverse early mucosa-associated lymphoid tissue lymphoma.4–6 Several treatment regimens for the eradication of H. pylori have been adopted in different regions of the world with varying results, but the search continues for a safe, tolerable, cheap, and highly effective regimen. To be considered effective, a treatment regimen should achieve at least an 80% eradication rate, 7 with some experts suggesting that the target eradication rate should be closer to 90–95%. 8 The most commonly used regimen worldwide is the so-called triple regimen consisting of a proton pump inhibitor (PPI) and clarithromycin in combination with amoxicillin or, in the case of penicillin allergy, metronidazole.6,7 Despite recent evidence that the efficacy of this ‘heritage’ clarithromycin-based triple therapy is waning – to unacceptably low levels in some populations – it remains the most commonly used first-line therapy for eradication of H. pylori. 8
The addition of metronidazole to legacy triple therapy, whether part of the sequential or concomitant regimen, as so-called nonbismuth quadruple therapy (NBQT), has been shown to improve eradication rates of H. pylori, including clarithromycin-resistant strains.9,10 A meta-analysis by Essa et al. 11 comparing all three aforementioned regimens concluded that sequential and concomitant quadruple therapy are equally effective and superior to standard triple therapy (STT). The concomitant regimen was found to be less complex than the sequential regimen and was therefore recommended in regions where STT was rendered ineffective. A recent study from Spain and Italy, 12 regions of relatively high clarithromycin resistance (19–20%), suggested that more than 90% of H. pylori infections can be eradicated with a 14-d course of concomitant or hybrid (PPI and amoxicillin for 14 days with addition of clarithromycin and nitroimidazole for the final 7 days) NBQT including high-dose PPI (omeprazole 40 mg b.i.d.).
We have recently shown that a 10-day half-dose triple regimen – where the dose of all three components of the STT is reduced by 50% – can achieve similar eradication rate as its standard-dose counterpart but with significant reduction in adverse events and cost. The overall eradication rate was, however, suboptimal (77.6% with standard-dose therapy and 77.2% with half-dose triple therapy on ITT), signalling a 13.8% decline in eradication rate of the exact standard-dose regimen over a 6-year period within the same geographic area and institution. 13,14 Based on the reported superiority of NBQT and the promising concept of reduced-dose combination therapy, this study was designed to investigate the efficacy and safety of 7-day standard-dose vs. half-dose concomitant NBQT regimen for the eradication of H. pylori infection.
Materials and methods
Study design
From December 2011 to August 2012, 200 consecutive adult patients with H. pylori infection, documented by either urea breath test (UBT) or rapid urease assay, were enrolled in the study. Patients were excluded if they were allergic to any of the drugs used, had taken antibiotics recently (within 2 weeks of enrolment), had severe ulcers or bleeding, gastric perforation or obstruction, previous gastrectomy, or gastric cancer, were pregnant or lactating, had received prior eradication therapy for H. pylori, or had severe concomitant disease or a condition making the treatment unlikely to be effective (e.g. alcoholism or drug addiction). The study was approved by the Institutional Review Board at the American University of Beirut and registered at clinicaltrials.gov (ID: NCT01219764).
After informed consent, patients were randomized using a computer-generated random-numbers table into one of two treatment groups. Patients in the standard-dose group were assigned to receive rabeprazole 20 mg b.i.d. (before meals), amoxicillin 1 g b.i.d. (with or after meals), clarithromycin 500 mg b.i.d. (with or after meals), and metronidazole 500 mg b.i.d. (with or after meals) for 7 days. Patients in half-dose arm received all four drugs but at 50% posology. A brief questionnaire was filled out for each patient regarding demographics including age, sex, height, weight, smoking status, previous use of clarithromycin or azithromycin, and current use of PPIs. All study participants were contacted by telephone on days 3 and 7 of the treatment period to evaluate compliance and inquire about possible adverse events. Patients were specifically asked if they experienced nausea, diarrhoea, abdominal pain, or metallic taste during the course of treatment. 14 C-UBT were performed a minimum of 4 weeks after therapy or use of any antibiotic and a minimum of 2 weeks off any acid-suppressive therapy.
Statistical analysis
The primary end point of the study was the rate of H. pylori eradication. The sample size calculation for a noninferiority trial, assuming an eradication rate in the standard and half-dose groups of 90% and a noninferiority limit of 10–11% with 80% power, was 93 to 112 patients per arm. Secondary end points included adverse events and overall cost, factoring in the cost of failed therapy (i.e. use of a second-line eradication regimen and repeat UBT testing). All data entry and statistical analysis were carried out using SPSS version 16.0 for Windows (SPSS, Chicago, IL, USA). Chi-squared and Fisher exact tests were used to compare the major outcomes between these groups. A p-value <0.05 was considered statistically significant.
Eradication rates were evaluated by both intention-to-treat (ITT) and per protocol (PP) analyses. The ITT analysis included all study participants who took at least one dose of the study medications. Patients who were subsequently lost to follow up after starting treatment or whose infection status was unknown after treatment were considered treatment failures for the purpose of the ITT analysis. The PP analysis included only patients who completed a full course of therapy according to study instructions and returned for a post-treatment UBT. Differences in adverse events were compared between groups using Chi-squared and Fisher exact tests. Univariate testing using Chi-squared and Fisher exact tests was also used to determine whether any of the patient’s characteristics obtained from the patient questionnaire were significant factors affecting the response to treatment in both groups.
Results
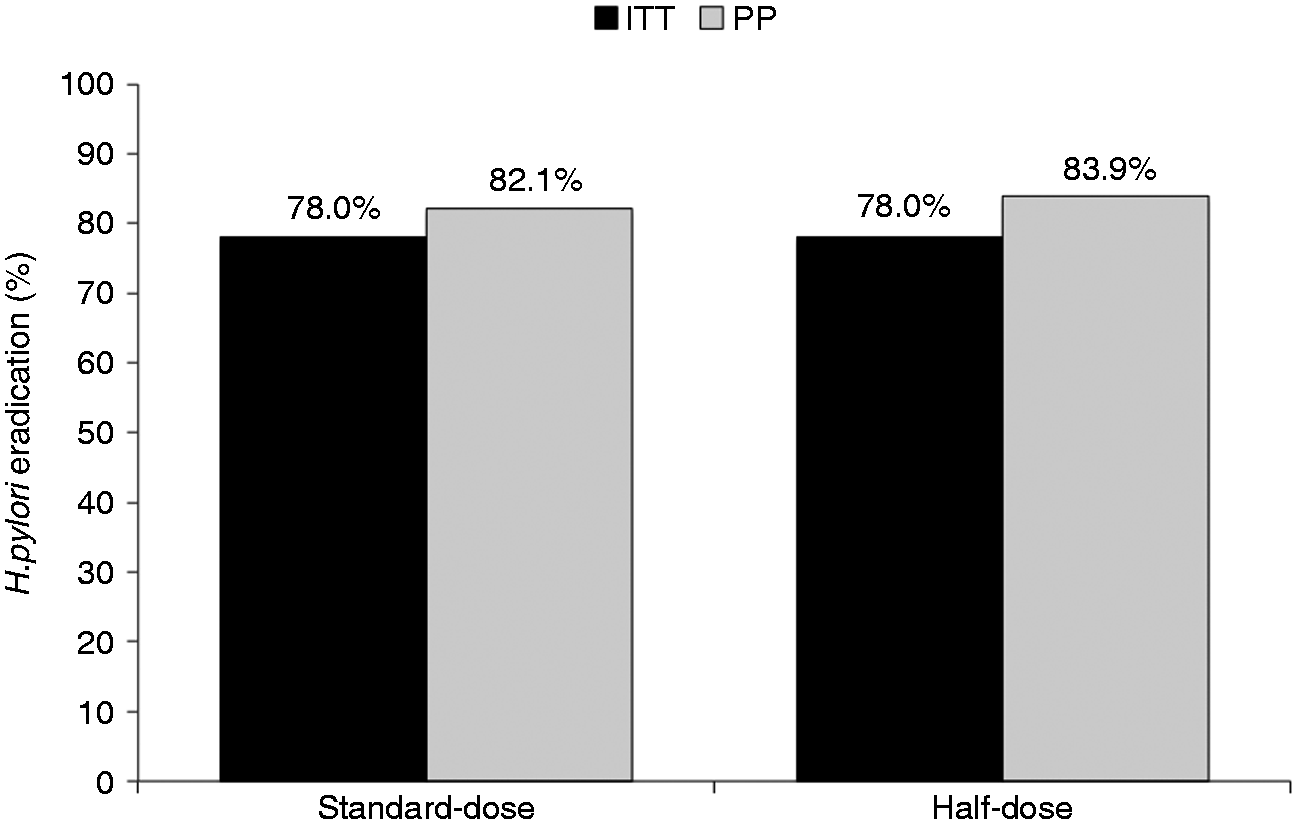
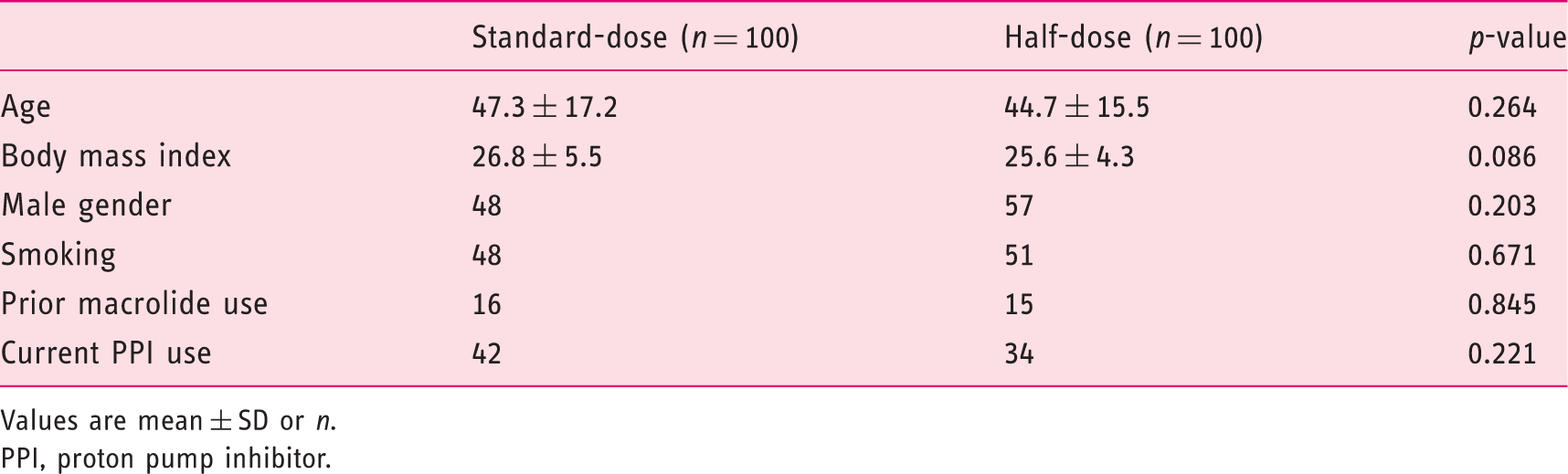
A total of 200 patients infected with H. pylori were randomized to either standard-dose (n = 100) or half-dose arm (n = 100). The clinical and demographic characteristics of the study subjects are summarized in Table 1. There was no significant difference in age, sex, body mass index, smoking status, previous use of macrolides, or current use of PPIs between the two groups. Of the study patients, 181 had oesophagogastroduodenoscopy and 43 (23.8%) had documented peptic ulcer disease: 21/92 (22.8%) in the standard-dose arm vs. 22/89 (24.7%) in the half-dose arm, respectively (p = 0.54). Overall, 10 patients (three in the standard-dose group and seven in the half-dose group) did not complete the study and/or return for UBT after treatment; two patients from the standard-dose group stopped treatment on day 3 and then resumed 2 days later because of severe nausea (Figure 1). On ITT analysis, the eradication rate for both groups was 78 out of 100 (78.0%, 95% CI 68.6–85.7%) and on PP analysis, the eradication rate was 78/95 (82.1%, 95% CI 72.9–89.2%) in the standard-dose group vs. 78/93 (83.9%, 95% CI 74.8–90.7%; p = 0.71) in the half-dose group (Figure 2). There was no difference in H. pylori eradication rates between those with or without endoscopically proven peptic ulcer disease.
Study consort flow diagram. Rates of eradication according to group assignment. ITT, intention-to-treat; PP, per-protocol. Patient characteristics Values are mean ± SD or n. PPI, proton pump inhibitor.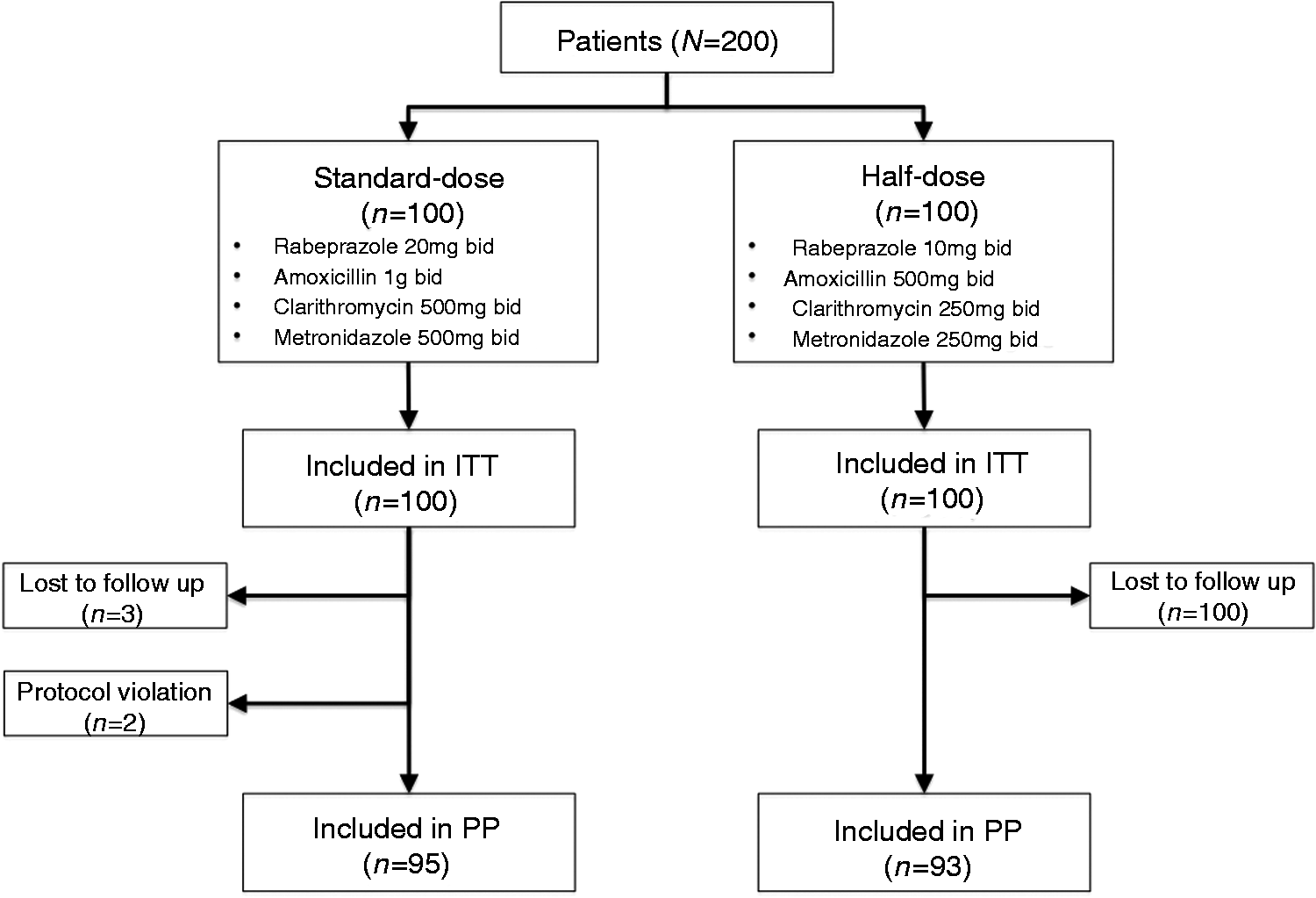
Side effects reported during treatment
Treatment failure was noted in 12/31 patients (38.7%) who reported prior macrolide use compared to 32/169 (18.9%) patients who did not (ITT; p = 0.019) (Figure 3). On multivariate analysis, age, sex, body mass index, smoking status, peptic ulcer disease, and use of PPIs before treatment did not have any significant impact on the observed eradication rates. Previous macrolide use was the only variable significantly associated with an increased risk of ineffective eradication (OR 2.60, 95% CI 1.06–6.39; p = 0.038). Given absolute parity in the eradication rate in both groups, the cost of treatment (based on local retail price) was significantly less in patients receiving the half-dose regimen (ITT analysis; p < 0.05).
Failure of eradication according to macrolide exposure history.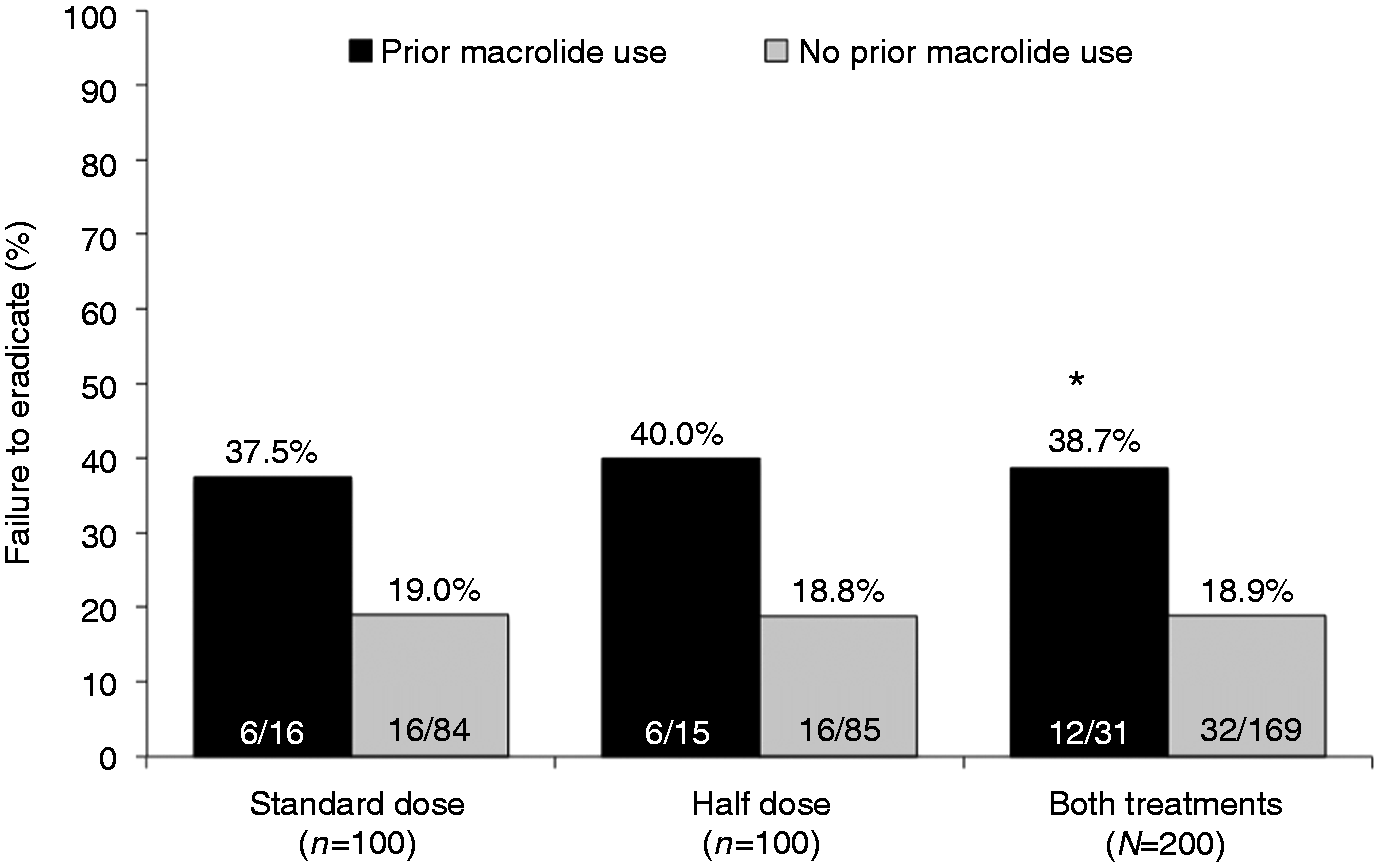
Discussion
Trials published since 2010 investigating concomitant NBQT
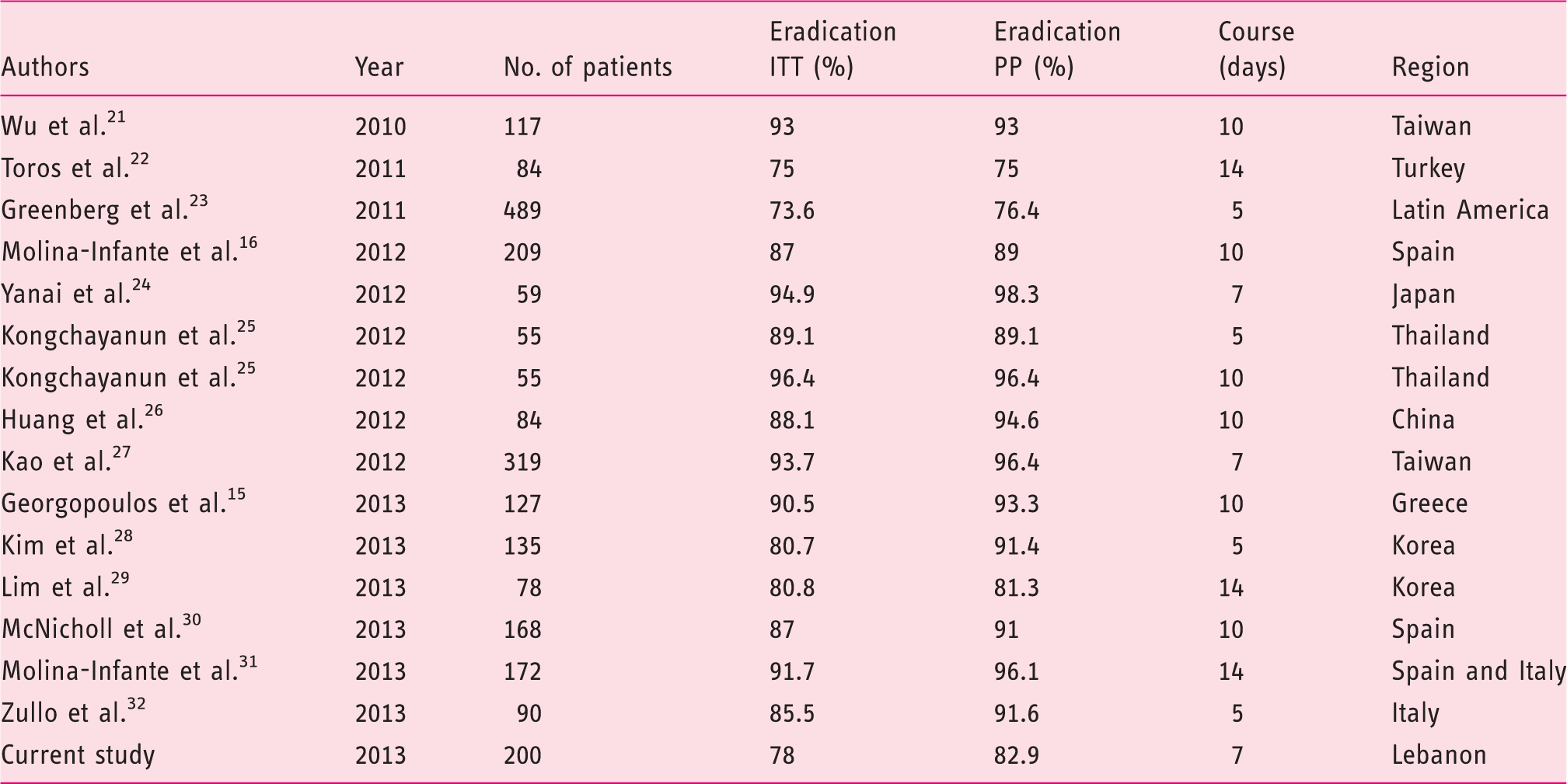
ITT, intention-to-treat; PP, per-protocol.
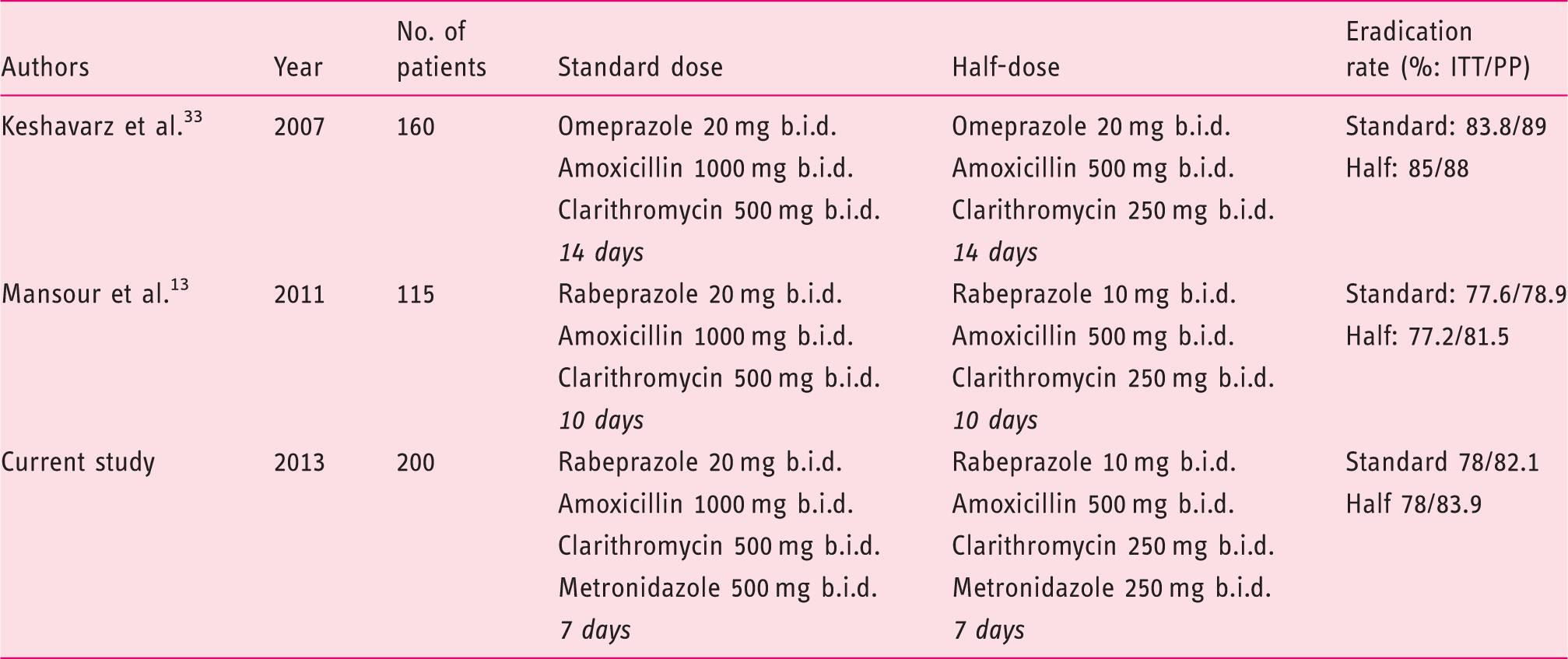
Randomized controlled trials examining standard-dose vs. half-dose antibiotic therapy for H. pylori infection
An important result of this study is the significant reduction in cost and adverse events with the half-dose concomitant NBQT. Although adverse events are often mild with first-line H. pylori regimens, they remain frequent and are an important cause for noncompliance and suboptimal adherence with detrimental clinical outcomes. In H. pylori clinical trials, approximately 5–10% of enrolled subjects drop out or are excluded from per-protocol analysis because of adverse events, poor compliance, or adherence 36 and this number increases with longer duration of treatment. 37 In the recent trial by Moline-Infante et al., 12 patients receiving the hybrid version of the 14-day NBQT (diminished pill burden by reduced exposure to clarithromycin and metronidazole to the last 7 days) had less adverse events (47 vs. 56%; p = 0.06) and greater compliance (98.8 vs. 95.2%; p = 0.05) than the concomitant NBQT version. Despite the long duration of therapy in that study, a heavy pill burden (112 tablets) and frequent, albeit mild, adverse effects, a remarkable 93.5% of 343 patients were ‘fully compliant’ with the prescribed concomitant NBQT and only 6% withdrew because of adverse events. 12 The real-world scenario is, however, different and is likely to be worse. Drug therapies often possess different performance characteristics in controlled clinical trials compared to the real world (effectiveness vs. efficacy). Outcomes in clinical trials are often favoured because of the homogeneous nature of the study population, close patient follow up, the presence of well-defined protocols, adherence controls (e.g. pill counts, phone calls), financial incentive (free drug supplies, tests, and follow up), and patient motivation. Patient adherence is thus a critical variable that influences the ultimate effectiveness of treatment and adverse events are an important determinant to such adherence.
In our study, both standard-dose and half-dose concomitant NBQT for 7 days resulted in suboptimal eradication rates (<80%). Despite limited direct comparative data, a longer duration of NBQT is likely to result in improved eradication (Table 3). Prolonging the duration of therapy may add what amounts to 0.5–1%-per-day benefit in eradication rates but is expected to result in significant increase in adverse events and cost, as well as diminished compliance and adherence.
Whether the added benefit with respect to eradication rates is consistent in the case of clarithromycin-resistant strains is largely untested. In the absence of shorter, simpler, and safer alternatives, the use of 14-day NBQT may be an acceptable option in the era of increased resistance to clarithromycin. However, in our study, 38.7% of patients with a history of prior macrolide use failed to eradicate H. pylori compared to 18.9% of those with no such history. A history of prior macrolide use leads to more complex resistant strains and the rates of resistance are directly proportional to the courses of macrolides used.38,39 A recent multicentre European survey study showed a steady increase in clarithromycin resistance, with almost doubling over a 10-year period from 9.8 to 17.5%.40,41 Studies have suggested that this global increase in clarithromycin resistance appears to correlate with increase prescription usage of clarithromycin, roxithromycin, and azithromycin.41,42 Although we did not perform in vitro susceptibility testing, the high rate of treatment failure noted in prior macrolide users in our study appears to support this conclusion. Data from IMS Health show a steady increase in the usage of clarithromycin in Lebanon, with approximately 75% growth over a period of 5 years (Figure 4).
Clarithromycin sales in Lebanon 2008–2013 (data with permission from IMS Health Lebanon).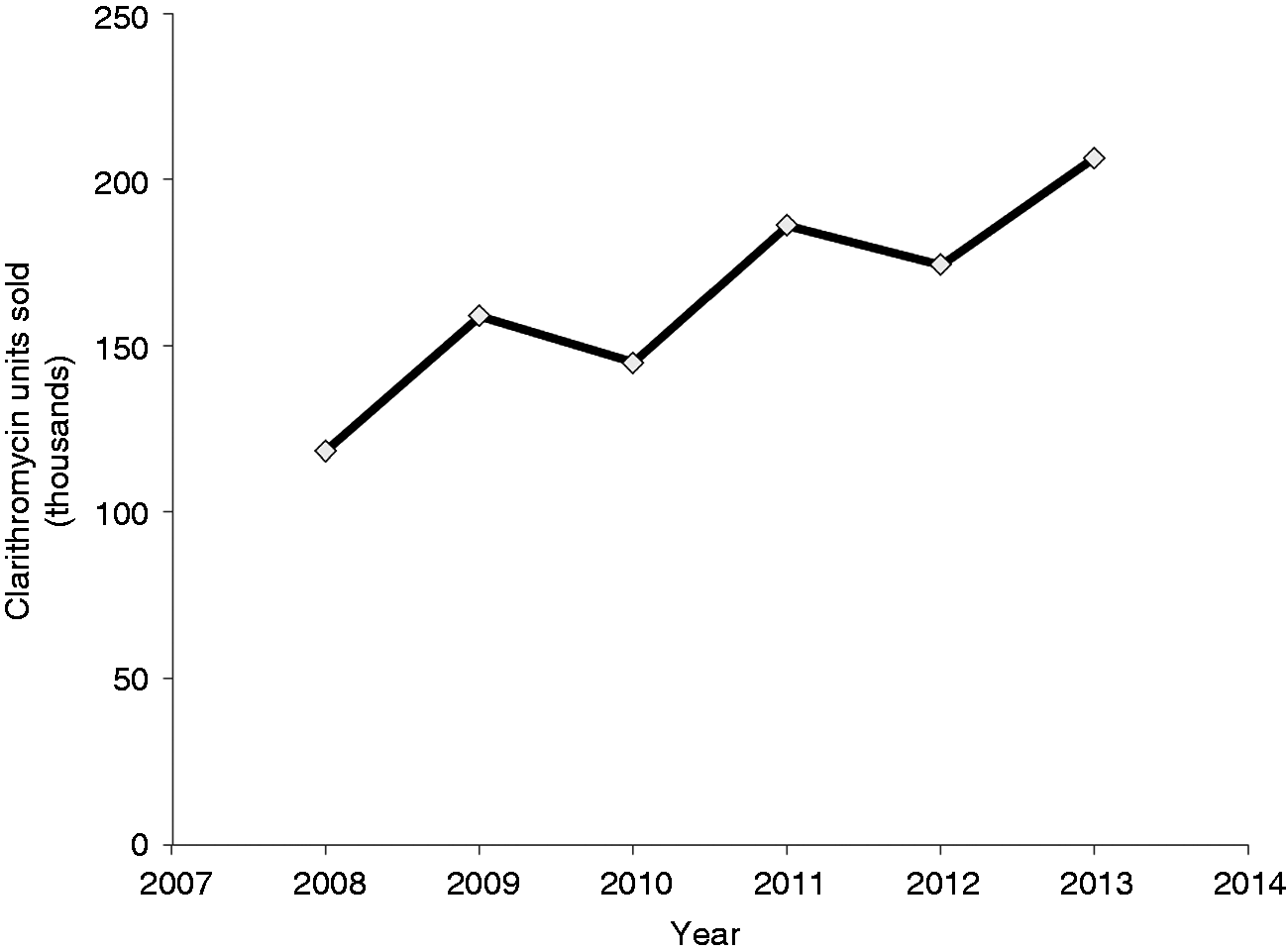
In the recent multicentre Spanish–Italian study, 14-day of concomitant NBQT was successful at eradicating all clarithromycin-resistant strains of H. pylori. However, this was applicable to only eight patients (of 68 undergoing in vitro culture and susceptibility). Based on the above and in the absence of stronger evidence to the contrary, we believe that all clarithromycin-based regimens should be avoided in patients with known or documented history of prior macrolide use. Such an important variable should be sought in every patient considered for H. pylori treatment.
There are a few limitations to our study. Culture and in vitro susceptibility testing were not performed and hence the exact role of antibiotic resistance (namely to clarithromycin and metronidazole) in eradication failure cannot be evaluated. Moreover, information on prior macrolide use was collected from patients using a questionnaire and may therefore be subject to recall bias. Although this is one of the largest controlled trials on concomitant NBQT (Table 3), it was powered at 80% with a delta of 10% for noninferiority assuming an eradication rate of 90% in both study arms. Eradication rates in this study were, however, suboptimal in both arms. This notwithstanding, given absolute parity on ITT analysis, it is somewhat unlikely that we missed a true or clinically significant difference between both regimens. Lastly, the potential effect of CYP2C19 genetic polymorphism on PPI metabolism and, consequently, the stability of the acid-labile antibiotics amoxicillin and clarithromycin was not investigated. This may conceivably be of added importance when one uses reduced-dose PPIs in CYP2C19 ultra-metabolizers, a common phenotype in Western populations. It is important to note, however, that rabeprazole undergoes primarily a nonenzymic hepatic metabolism and that multiple studies have confirmed equivalent eradication rates between standard-dose and reduced-dose rabeprazole in clarithromycin-based triple therapy and independent of CYP2C19 genetic polymorphism. 43 The equivalent eradication rates in our study in a population with matching CYP2C19 profile to people of European origin 44 appears to fall in line with this observation.
In conclusion, a 7-day half-dose concomitant NBQT is equally effective but better tolerated and cheaper than its standard-dose equivalent in the treatment of H. pylori. The concept of reduced-dose antimicrobials in multidrug H. pylori regimens seems partially validated and deserves further evaluation in large randomized controlled trials. Such a strategy can lead to significant cost savings, reduced adverse events, and enhanced compliance, adherence and treatment uptake and may consitute a paradigm shift in the treatment of H. pylori. Although likely, it remains unproven whether the half-dose strategy remains effective with extended concomitant NBQT for 10 or 14 days and leads to acceptable eradication rates.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.
Presentation
This work was presented in part at the American College of Gastroenterology Annual Meeting, Las Vegas, NV, USA, 19–24 October 2012 and in full as an oral presentation at the 28th International Congress of Chemotherapy and Infection, Yokohama, Japan, 5–8 June 2013.