
Abstract
Aim
To identify clinical and/or genetic predictors of response to several therapies in Crohn’s disease (CD) patients.
Methods
We included 242 patients with CD (133 females) aged (mean ± standard deviation) 39 ± 12 years and a disease duration of 12 ± 8 years. The single-nucleotide polymorphisms (SNPs) studied were ABCB1 C3435T and G2677T/A, IL23R G1142A, C2370A, and G9T, CASP9 C93T, Fas G670A and LgC844T, and ATG16L1 A898G. Genotyping was performed with real-time PCR with Taqman probes.
Results
Older patients responded better to 5-aminosalicylic acid (5-ASA) and to azathioprine (OR 1.07, p = 0.003 and OR 1.03, p = 0.01, respectively) while younger ones responded better to biologicals (OR 0.95, p = 0.06). Previous surgery negatively influenced response to 5-ASA compounds (OR 0.25, p = 0.05), but favoured response to azathioprine (OR 2.1, p = 0.04). In respect to genetic predictors, we observed that heterozygotes for ATGL16L1 SNP had a significantly higher chance of responding to corticosteroids (OR 2.51, p = 0.04), while homozygotes for Casp9 C93T SNP had a lower chance of responding both to corticosteroids and to azathioprine (OR 0.23, p = 0.03 and OR 0.08, p = 0.02,). TT carriers of ABCB1 C3435T SNP had a higher chance of responding to azathioprine (OR 2.38, p = 0.01), while carriers of ABCB1 G2677T/A SNP, as well as responding better to azathioprine (OR 1.89, p = 0.07), had a lower chance of responding to biologicals (OR 0.31, p = 0.07), which became significant after adjusting for gender (OR 0.75, p = 0.005).
Conclusions
In the present study, we were able to identify a number of clinical and genetic predictors of response to several therapies which may become of potential utility in clinical practice. These are preliminary results that need to be replicated in future pharmacogenomic studies.
Introduction
Crohn’s disease (CD) is a chronic and relapsing condition, with the majority of patients experiencing a progressive and disabling course over time. 1,2 Management of disease is complex and should take into account several factors such as disease location, activity, and behaviour. 3 Additional disease aspects that make management difficult are the lack of correlation between severity of clinical symptoms and severity of intestinal inflammation and the difficulty in predicting a patient’s clinical course and the individual response to a given treatment.
According to ECCO guidelines, 5-aminosalicylic acid (5-ASA) compounds could be used to treat patients with mild-to-moderate ileocecal disease, whereas the use of azathioprine/6-mercaptopurine and/or anti-tumour necrosis factor (TNF) therapy is recommended for patients with moderate to severe disease who relapse after responding to steroids. 3
In the past years, numerous efforts have been made with the aim of identifying early predictors of aggressive disease 4 –6 because, intuitively, patients presenting indicators of bad outcome at diagnosis would be the ideal candidates for early and more aggressive therapy in order to avoid long-term structural damage. However, patients who present with disease bad prognostic factors are not necessarily those who will respond better or worse to certain therapies. Although tailored therapy in CD is still far from reality, reliable prediction of response to treatment, combined with clinical indicators of aggressive disease, could allow a better selection of candidates for treatment, allowing the choise of not only the most effective therapies but also the less toxic ones. It is certainly important to remember that, according to previous studies, 7,8 30% of CD patients will have a mild disease course and will never need corticosteroids.
Previous studies have mainly focused on clinical predictors of response to biologicals. Short duration of disease is probably the single most important factor of response to anti-TNF agents and perhaps to azathioprine as well. 9 –11 Some found better responses to biologicals in nonsmoking patients with recent onset and colonic disease, while others could not confirm these observations. 12 –15 A high value of basal C-reactive protein also seems to be a predictive factor of response to biologicals. 16
As well as clinical and laboratory predictors, genetics could also influence patients’ individual response to a drug. 17,18 So far, pharmacogenomic research in inflammatory bowel disease has witnessed only modest success and sometimes conflicting results, mainly because response to treatment in this disease is very heterogeneous as it is influenced by many factors, such as disease duration, behaviour, and severity, which certainly interact with genetic variables and modulate response to treatment. 19 –21 While some authors reported that carriers of ABCB1 single-nucleotide polymorphisms (SNPs) present a worse response to azathioprine or corticosteroids, others could not confirm these observations. 22 –25 ABCB1 codes for the ATP-dependent membrane efflux transporter P-glycoprotein 1, which is expressed in various cells including in those in the gastrointestinal tract, which is responsible for resistance to a number of structurally and functionally unrelated drugs. IL23R has been recently implicated in the pathogenesis of CD. Although previous studies found that SNPs in this gene could increase susceptibility to develop CD, 26 few studies explored the association between these SNPs and phenotype or response to therapy in patients with inflammatory bowel disease. 18,27,28 Caspase9, Fas, and fas ligand encode for proteins involved in apoptosis, which has been shown to be defective in CD. Hlavaty et al. 29,30 observed that carriers of SNPs of genes involved in apoptosis, responded less frequently to biologicals. Finally, ATG16L1 is involved in autophagy, a key pathway for innate immunity and important for maintaining the epithelial barrier. Several drugs already used in the treatment of CD might exert at least part of their effect through the regulation of autophagy. 31 A recently published study found an association between SNPs in this gene and response to corticosteroids, azathioprine, and biologicals. 32
The primary aim of the present study was to identify clinical and/or genetic factors that, alone or in combination, could predict response of CD patients to several therapies. Our secondary end point was to distinguish between those patients who will be in remission with azathioprine only from those who will need escalation to anti-TNF agents.
Materials and methods
This was a multicentre study with participating hospitals from Central Portugal. Informed consent was obtained from all patients entering the study, which was approved by Scientific and Ethical committees of the several participating hospitals.
Patients with the diagnosis of CD 33 were classified according to the Montreal classification 34 based on age at diagnosis (A), location (L), and behaviour (B). Disease modifiers were also considered: L4 when the upper digestive tract was involved and P for perianal involvement. No families with CD were included in the present series. Phenotypic characteristics retrospectively collected from charts included demographic data, age of disease onset, disease extension, and behaviour, time of follow up, smoking habits, presence of extraintestinal manifestations, and previous therapies including surgery. All phenotypic data were collected in a blinded fashion to the results of the genotypic data.
Patients were selected to enter the study if a definitive classification in terms of response to a specific drug could be clearly obtained after reviewing the chart and interviewing the patient at the moment of entering the study. Patients were considered responders if they presented long-term sustained remission, defined as a Harvey Bradshaw Index (HBI) lower than 4, lasting at least 1 year after a certain therapy was started, not needing steroids, surgery, or escalation of therapy to biologicals for those taking azathioprine or switch to another biological (infliximab vs. adalimumab) for those on biologicals. Patients requiring the addition or switching to other therapies, corticosteroids or surgery before 1 year were considered nonresponders. If a clear distinction between these two scenarios was not possible for a specific drug, the patient was not considered either as a responder or as a nonresponder at least for this drug. Because our secondary end point was to distinguish between patients who responded to azathioprine from those who came to require biologicals, if a patient had a clinical remission for less than 1 year with azathioprine but came to require biologicals, he or she was considered a nonresponder to azathioprine.
Decision to switch therapy was made by the treating physician. HBI was calculated after a new therapy was started until the drug was discontinued or until end of follow up. Optimization of dose and/or interval of administration in patients on biologicals, was considered as therapy optimization and not as nonresponse. Biological parameters such as C-reactive protein levels or endoscopic response were not used to classify patients as responders or nonresponders because identification of these data on the precise moment on which a specific therapy was started was not clear in a large number of patients.
For steroids, only short-term response was considered. Steroid dependence was defined as recurrent flare up on withdrawal of glucocorticoids or as the need for glucocorticoids treatment twice within 6 months. Patients were considered refractory to steroids when no remission was obtained with a dose of 1 mg/kg during a period of at least 4 weeks.
DNA extraction and genotyping
Blood samples were taken from all study participants, and genomic DNA was isolated from peripheral blood using a DNA blood mini kit from Quiagen (Hiden, Germany) according to the manufacturer’s guidelines. A total of 10 SNPs were studied: ABCB1 C3435T (rs1045642) and G2677T/A (rs2032582), IL23R G1142A (rs11209026), C2370A (rs10889677), G43045A (rs 1004819) and G9T (rs1884444), CASP9 C93T (rs4645983), Fas G670A (rs1800682), Faslg C844T (rs763110), and ATG16L1 A898G (rs2241880). All genotypes were determined using real-time PCR with TaqMan Pre-Designed SNP Genotyping Assays (Applied Biosystems, USA), except for Fas G670A and FasLg C844TT, which were determined using Custom TaqMan SNP genotyping Assays probes (Applied Biosystems). To perform the genotype analysis, the target fragments were amplified in 20 -µl reaction mixture containing 10 µl TaqMan Universal PCR Master Mix, 1 µl primers, 5 µl Milli-Q water, and 4 µl DNA. Real-time PCR was conducted using a iCycler iQ® Multicolor Real-Time PCR Detection System (BIO-RAD) with the following thermal cycling program: 10 min at 95℃ and 50 cycles of 15 s at 92℃ and 1 min at 60℃.
Statistical analysis
Statistical analysis was performed using SPSS version 14.0 (SPSS, Chicago, IL, USA) and SNPassoc 1.6 package in R software. Data were expressed as mean ± standard deviation, number of subjects (%), or odds ratio (OR) with 95% confidence interval (CI). Primary analyses were performed using chi-squared test and univariate logistic regression. Multivariate logistic regression was performed to adjust for potential confounding variables. Receiver operating characteristic (ROC) curves were plotted for multivariate models, and sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and area under the curve (AUC) were calculated. Whenever the AUC value was under 0.65, the model performance was considered unacceptably low and data are not shown. Association between outcome and SNP was analysed with SNPassoc library in R and SPSS 19 (IBM SPSS statistics). Different inheritance models (dominant, recessive, log-add, and overdominant) were considered and were presented as eligible. Haplotype analysis was performed for ABCB1 C3435T and ABCB1 G2677T/A. To adjust for multiple testing, a Bonferroni correction was applied. Statistical significance was established for p < 0.05. Differences in genotypic and allelic frequencies and Hardy–Weinberg tests were performed using GENEPOP Web version 4.0.10 program. To obtain the exact p-value of the Hardy–Weinberg equilibrium, the Markov Chain method (Guo and Thompson, 1992) with a dememorization number of 1000, 100 batches, and 1000 iterations per batch was used. The p-value returned by this method is calculated as the sum of the probabilities of all tables and its standard error. Genotypic frequencies are under Hardy–Weinberg equilibrium when p > 0.001
Results
Demographic and clinical data from patients included in the study
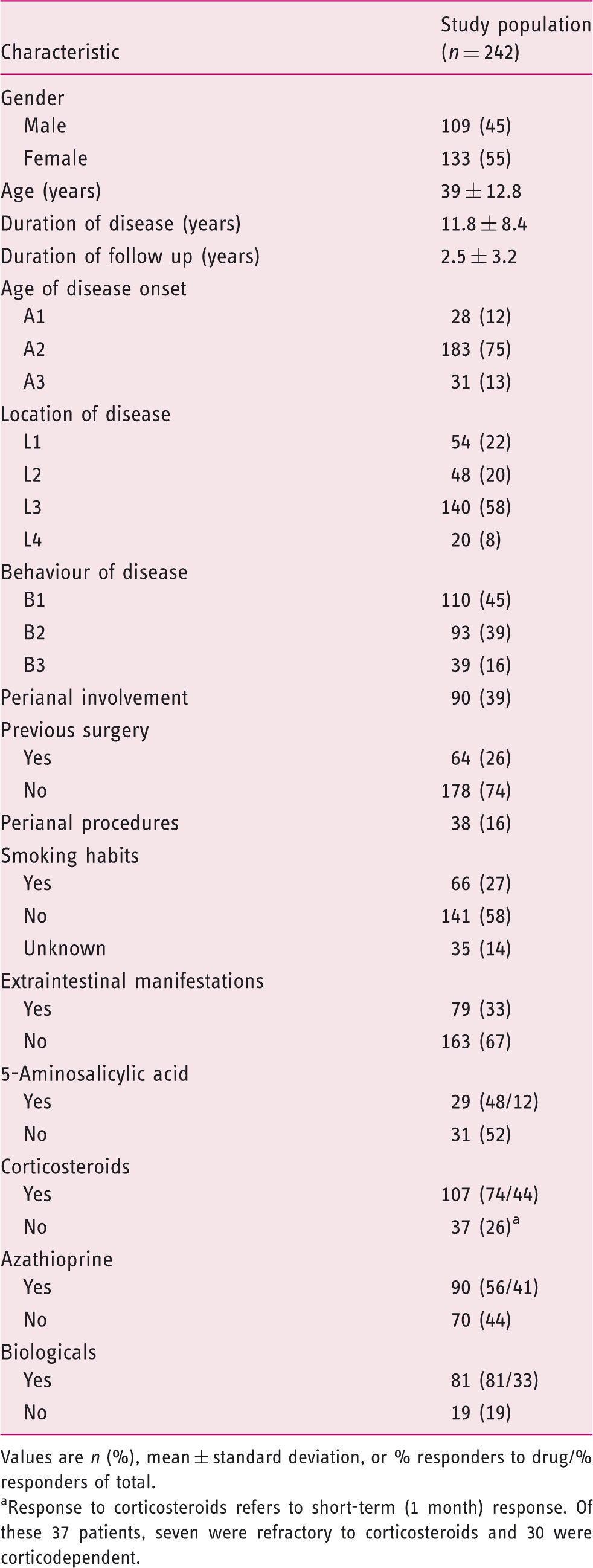
Values are n (%), mean ± standard deviation, or % responders to drug/% responders of total.
Response to corticosteroids refers to short-term (1 month) response. Of these 37 patients, seven were refractory to corticosteroids and 30 were corticodependent.
Allelic and genotypic frequencies
Genotypic frequencies, allelic frequencies, and Hardy–Weinberg equilibrium
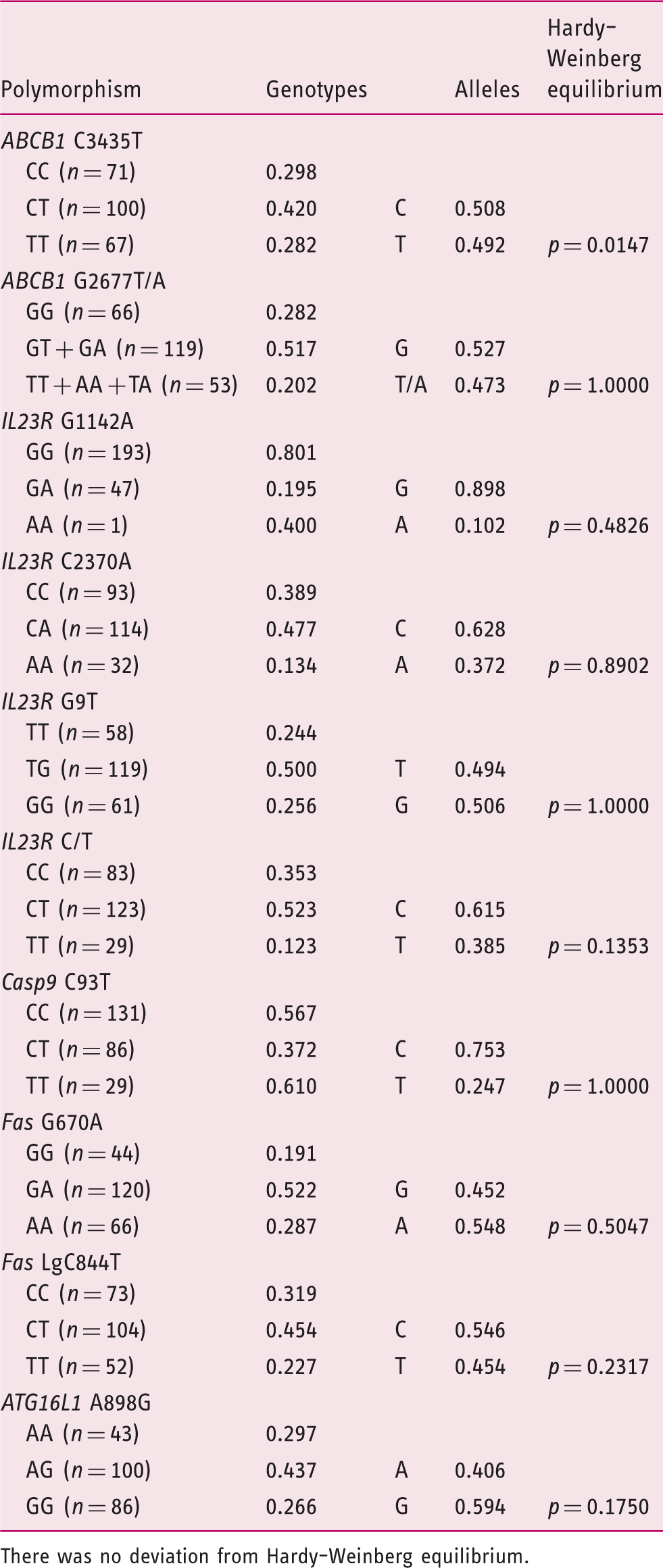
There was no deviation from Hardy–Weinberg equilibrium.
Associations between genetic polymorphisms and phenotypic characteristics
We observed that carriers for IL23R G9T and IL23R C2370A SNPs had less frequently upper GI involvement as compared to wild-type carriers (OR 0.4, 95% CI 0.2–0.82, p = 0.008, and OR 0.25, 95% CI 0.06–0.86, p = 0.03, respectively). Also, TT carriers for FasLg C844T SNP exhibited more often an inflammatory behaviour (B1) (OR 0.38, 95% CI 0.18–0.82, p = 0.014). No other significant associations were observed between the remaining SNPs and disease characteristics.
Associations between clinical characteristics, SNPs, and response to therapy
Association between clinical phenotypic characteristics and response to therapy according to univariate analysis
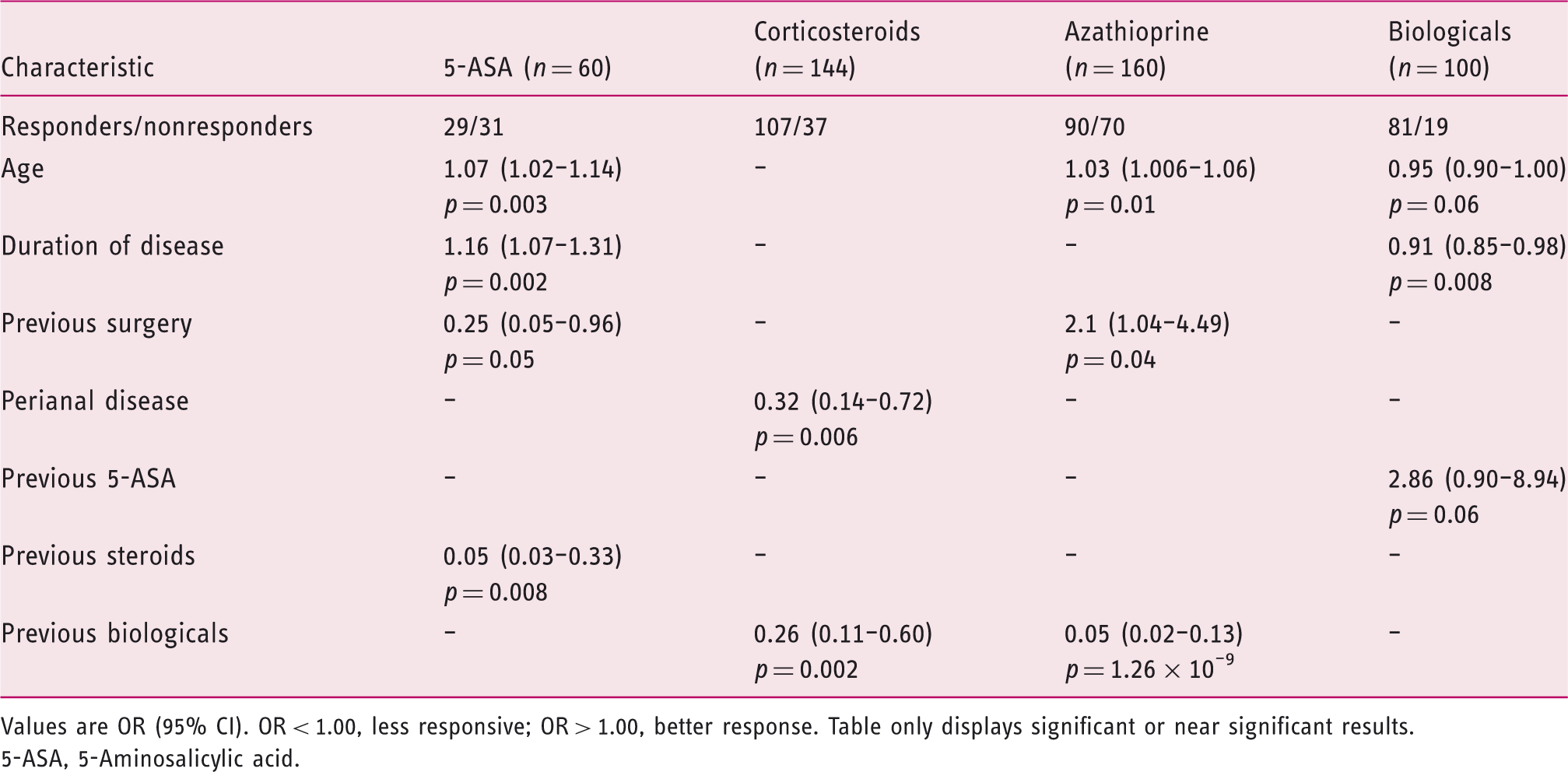
Values are OR (95% CI). OR < 1.00, less responsive; OR > 1.00, better response. Table only displays significant or near significant results.
5-ASA, 5-Aminosalicylic acid.
We observed that older patients and those with a longer duration of disease responded better to 5-ASA compounds (OR 1.07, p = 0.003 and OR 1.16, p = 0.002, respectively). On multivariate analysis, after adjusting for age and previous surgery, disease duration remained statistically significant (OR 1.21, p = 0.005); however, age was no longer statistically significant. The same trend was observed in respect to response to azathioprine and age (OR 1.03, p = 0.01), which means that there is a 3% increase in the chance of responding to azathioprine for each additional year of life. In respect to biologicals, an opposite trend was observed with a higher chance of response in younger patients (p = 0.06) and with more recent disease onset (p = 0.008). However, on multivariate analysis, both age and duration of disease lost significance.
Previous surgery negatively influenced response to 5-ASA compounds (OR 0.25, p = 0.05), while the opposite effect was observed in regard to azathioprine (OR 2.1, p = 0.04) (Table 3). In respect to perianal involvement, we observed that these patients did significantly worse on corticosteroids (OR 0.32, p = 0.006) (Table 3). No significant associations were found between disease behaviour, disease location including L4 involvement, smoking habits, presence of extraintestinal manifestations, and response to various therapies. Stricturing and penetrating phenotypes (B2 and B3, respectively) were more often associated with surgical therapy in contrast with inflammatory phenotype (B1) (OR 18.3, 95% CI 7.5–54.8, p < 0.0001).
Interestingly, previous therapies seemed to influence response to therapy in various ways (Table 3). Thus, previous 5-ASA users responded better to biologicals, although not reaching statistical significance (OR 2.86, 95% CI 0.90–8.94, p = 0.06). Previous corticosteroid therapy negatively influenced response to 5-ASA (OR 0.05, 95% CI 0.003–0.333, p = 0.008). Finally, previous use of biologicals decreased the chance of responding both to corticosteroids (OR 0.26, p = 0.002) and to azathioprine (OR 0.05, p = 1.26 × 10–9).
Association between genetic polymorphism and response to therapy according to univariate analysis
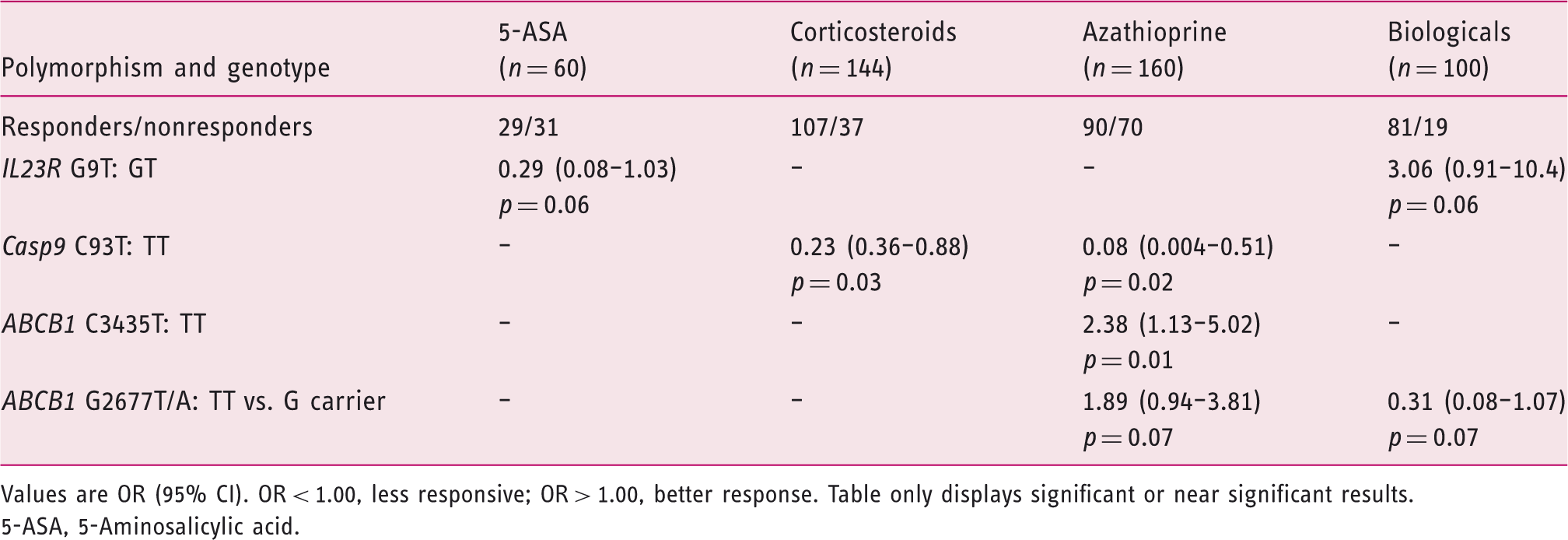
Values are OR (95% CI). OR < 1.00, less responsive; OR > 1.00, better response. Table only displays significant or near significant results.
5-ASA, 5-Aminosalicylic acid.
Homozygotes for Casp9 C93T SNP had a significantly lower chance of responding both to corticosteroids and to azathioprine (OR 0.23, p = 0.03 and OR 0.08, p = 0.02, respectively; Table 4). After adjusting for previous response to biologicals, gender, and ATGL16L1, the probability of responding to corticosteroids was even further decreased (OR 0.14, 95% CI 0.03–0.71 p = 0.014). A ROC curve was plotted for the previous model: 71.1% sensibility, 71.9% specificity, 54.9% PPV, 11.5% NPV, and an AUC of 0.778 was obtained (Figure 1).
Receiver operating characteristic curve for model assessment of the Casp9 C93T SNP Multivariate logistic regression model: dependent variable, therapy response to corticosteroids; independent variables, Casp9 C93T SNP, gender, previous therapy with infliximab, and ATGL16L1.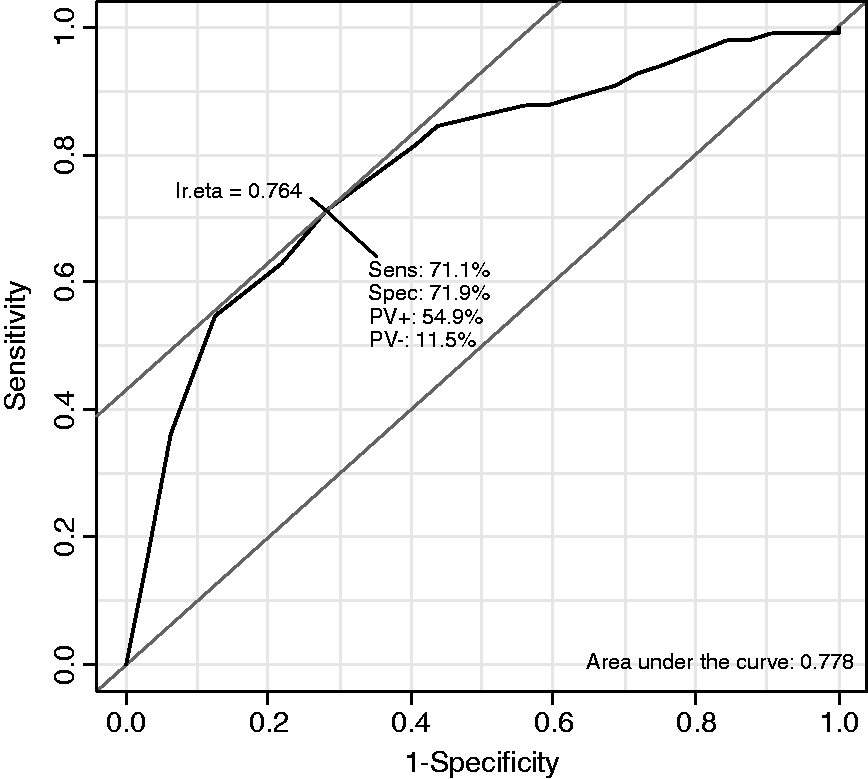
In respect to the ABCB1 C3435T SNP, we observed that TT carriers had a significantly higher chance of responding to azathioprine (OR 2.38, p = 0.01; Table 4). After adjusting for gender distribution, we observed that this association remained significant (OR 2.4, 95% CI 1.13–5.03 p = 0.019) and became even more significant after further adjustment for age and smoking habits (OR 3.22, 95% CI 1.13–5.03 p = 0.005). Model assessment with a ROC curve generated a 60,5% sensibility, 73% specificity, 39.5% PPV, 27% NPV, and an AUC of 0.687 (Figure 2).
Receiver operating characteristic curve for model assessment of the ABCB1 C3435T SNP Multivariate logistic regression model: dependent variable, therapy response to azathioprine; independent variables, ABCB1 C3435T SNP, gender, smoking habits, and age.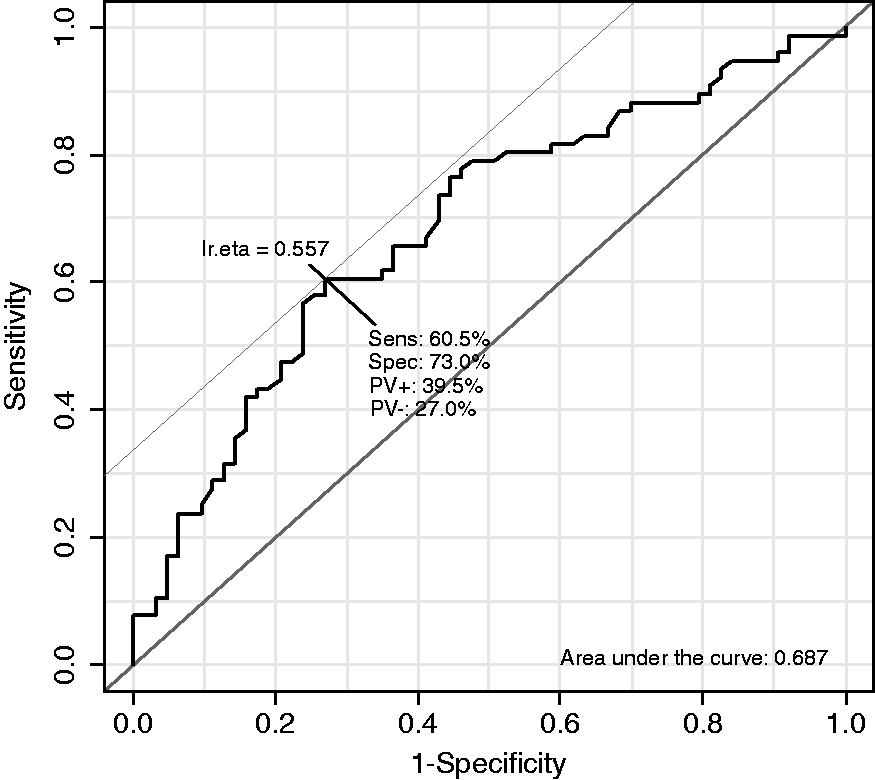
The same was observed for the polymorphic allele carriers of the other SNP of this gene (ABCB1 G2677T/A), although not reaching statistical significance (OR 1.89, p = 0.07). Carriers of both haplotypes had a higher chance of responding to azathioprine (OR 1.53, 95% CI 0.94–2.49, p = 0.08). The ABCB1 G2677T/A SNP, as well as responding better to azathioprine, had a significantly lower chance of responding to biologicals (OR 0.31, p = 0.07), which became significant after adjusting for gender (OR 0.75, 95% CI 0.24–0.63, p = 0.005). Adjusting for duration of disease also increased the strength of this association (OR 0.23, 95% CI 0.07–0.70, p = 0.01). When considering the ROC curve for the former model, 70.1% sensibility, 63.2% specificity, 65.7% PPV, 11.5% NPV, and an AUC of 0.714 was obtained (Figure 3).
Receiver operating characteristic curve for model assessment of the ABCB1 G2677T/A SNP Multivariate logistic regression model: dependent variable, therapy response to biologics; independent variables, ABCB1 G2677T/A SNP, gender, and disease duration.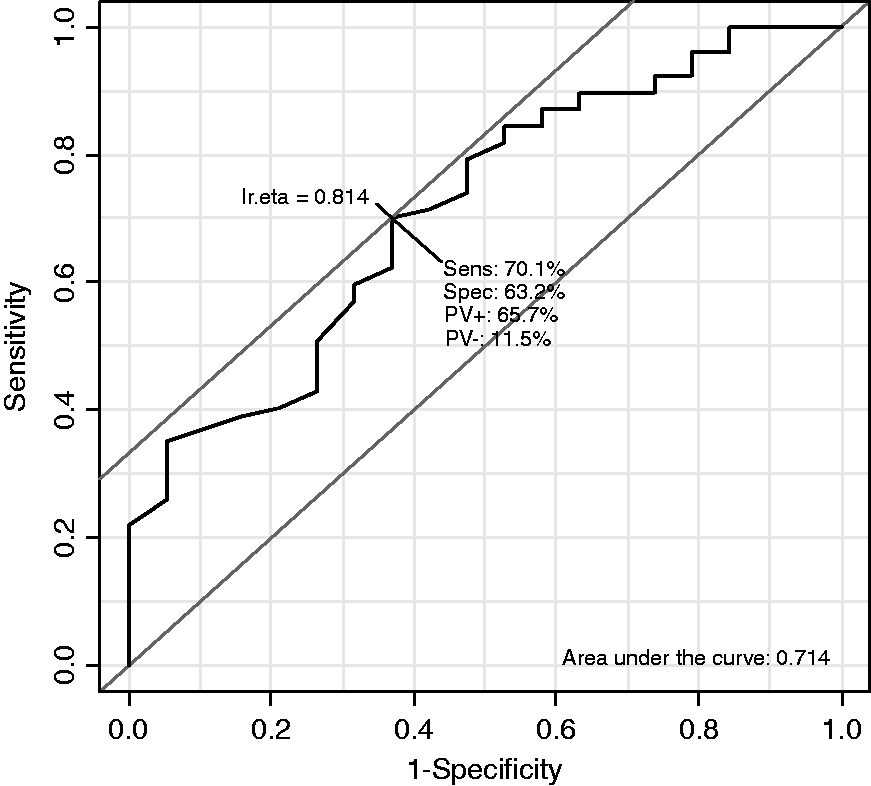
Interaction between ABCB1 haplotypes (C3435T and G2677T/A) and disease location
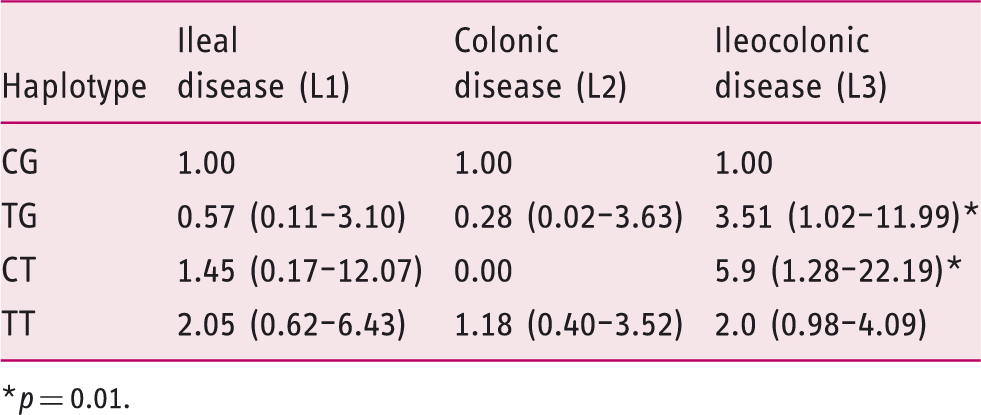
p = 0.01.
Discussion
CD is a heterogeneous disease both in terms of clinical manifestations as well as in terms of response to therapy. Great effort has been dedicated to develop treatment algorithms with the aim of choosing the most effective treatment with less adverse effects and risks. 35 –39 In this sense, a number of previous studies tried to identify clinical, 12 –16,40 serological, 41,42 or genetic 17 –25 predictors of response to several therapies available; however, so far, the results have not been very consistent across studies. One of the reasons for these discrepancies might result from what is considered response. In the present study, we decided to use long-term response (more than 1 year) because we believe that this concept is clinically more relevant. Thus, a patient who responds to azathioprine or biologicals at 2–3 months but later relapses with the need of corticosteroids or escalation of therapy was considered a nonresponder to this specific therapy.
In regard to predictors of response, we used both clinical and genetic markers. The latter may be more attractive because they do not change over time. However, in clinical practice they are of little value until their utility can be clearly demonstrated and validated in other studies. In contrast, clinical or phenotypic variables are more readily used in clinical practice.
In the present study, 25% of patients (60/242) were treated with 5-ASA: 29 of these responded to this therapy whereas the remaining 31 did not and required further escalation of therapy. Although overall this means a low number of patients (29/242, 12%), we think that it is certainly important to identify those patients who do very well on less aggressive and less toxic therapies. According to the last ECCO consensus, 3 no treatment may be an option in patients with mild disease, because a systematic review of clinical trials 43 showed that 18% of patients (95% CI 14–24%) of patients entered remission with placebo alone. In line with these findings, it is plausible that these patients could be treated with 5-ASA compounds only.
Previous surgery was a negative predictor of response in regard to 5-ASA (OR 0.25), but previously operated patients had a twice-higher chance of responding to azathioprine (OR 2.1). Clinically, we are often faced with the patient who does not respond to medical therapy, needs surgery, and post operatively has a mild course, further raising the question of whether, once the diseased segment is resected, he can be maintained on 5-ASA therapy or whether immunosuppression should be started. Our data strongly supports the latter.
In regard to corticosteroids we observed that previous therapy with biologicals was a negative predictor of response to both corticosteroids (OR 0.26) and to azathioprine (OR 0.05). These are important observations from a clinical point of view because patients who are on biologicals and relapse are often treated with corticosteroids. 3 According to our results, this is not contraindicated but they are less likely to respond. Also, patients who are doing well on combination therapy and in whom we want to de-escalate therapy, the immunosuppressor (azathioprine) should preferentially be stopped.
Genetic polymorphisms included in the present study were chosen according to previous studies, which had shown some type of association with response to therapy. Although some previously reported associations could not be confirmed in the present study, 23,29,30 we found some interesting associations in the sense that genotypes identified patients who were simultaneously less likely to respond to certain therapies but more prone to respond to others. Thus, individuals who are heterozygotic for IL23R G9T SNP were less likely to respond to 5-ASA (OR 0.29) but 3-times more likely to respond to biologicals (OR 3.06). TT carriers of Casp9 C93T SNP had a significant reduction in the probability of responding both to corticosteroids and azathioprine (OR 0.23 and 0.08, respectively), while TT carriers for both ABCB1 C3435T and ABCB1 G2677T/A showed a higher chance of responding to azathioprine. Concomitantly, TT carriers for ABCB1 G2677T/A had a 25% reduction in the probability of responding to biologicals, which might be relevant in clinical decisions. ROC curves were plotted to test the performance of each of these models. This analysis allowed us to assess the performance of each of these models including SNPs for the several genetic associations found in multivariate analysis and response to corticosteroids, azathioprine, and biologicals. AUC values close or higher than 0.70 are considered reasonable classifiers, further reinforcing the reliability of the associations found between SNPs tested and response to several therapies.
This study had some limitations that need to be addressed. A major drawback relies on the fact that response to drugs was evaluated retrospectively from data recorded in the charts. However, in our opinion, after having the perspective of long-term evolution and whether the patient came to require therapy escalation after a transitory response which lasted less than 1 year, evaluating the response to a specific drug is clinically more relevant than evaluating short-term responses. Another limitation refers to the number of patients included in the study, which may be considered low for a pharmacogenomic study. Therefore, the data obtained in the present study can only be considered preliminary until prospectively validated in an independent cohort of CD patients.
In conclusion, in the present study we were able to identify a number of clinical predictors of response to several therapies available to treat CD patients, that might be of help in clinical practice, not only to select patients for more potent therapies such as immunosuppressors or biologicals, but also to less toxic ones such as 5-ASA compounds. In regard to genetic predictors, associations found are certainly promising but can only, at best, be considered hypothesis generating until these results are confirmed in larger populations.
Footnotes
Funding
This research was supported by Grupo de Estudo da Doença Inflamatória Intestinal (2009–2012).
Conflict of interest
The authors declare that there is no conflict of interest.