
Abstract
Background and aims
Crohn’s disease (CD) frequently affects young women and may require surgery during pregnancy. Data regarding operation for CD in expectant mothers are scare.
Materials and methods
This was a retrospective nationwide survey from the GETAID Chirurgie. Any woman with CD undergoing surgery during pregnancy was eligible.
Results
A total of 15 cases were collected between 1992 and 2015. Most operations were performed due to penetrating or stricturing complications. Mean gestational age at delivery was 34 weeks, with a mean birth weight of 2507 g. Maternal post-operative complications occurred in two-thirds of cases. Maternal mortality rate was 6.7% and neonatal mortality rate 9.1%.
Conclusions
This is the largest case series of surgery for CD during pregnancy. This operation may have significant morbidity and mortality for mother, fetus, and newborn. Indication needs to be tailored to maternal status, disease severity, and gestational age. Surgery should be managed by experienced gynecologists, physicians, and surgeons. Active CD may be associated with a greater risk to the fetus than the surgical procedure itself.
Keywords
Key Summary
Data regarding surgery for Crohn’s disease during pregnancy are scarce This case report series seems to confirm significant morbidity and mortality for mother, fetus, and newborn Achieving and maintaining disease remission is a key factor for successful pregnancy outcomes
Introduction
Crohn’s disease (CD) affects mainly young people in their reproductive years.1Overall CD flare rates during pregnancy are similar to those reported in non-pregnant patients,2,3but women with active disease at conception have a higher risk of active disease during pregnancy than those who are in remission at the time of conception.4Women with active disease at conception also have increased risks of spontaneous abortion,5preterm delivery, and low birth weight.6,7Pregnancies in CD require cesarean section more often than in the general population.8Therefore, adequate control of disease before and during pregnancy is crucial.9Most inflammatory bowel disease (IBD) medications, with the exception of methotrexate, are considered safe during pregnancy.10While the majority of pregnant CD patients can be managed without surgery, severe exacerbations or complications may require multidisciplinary management involving gastroenterologists, obstetricians, neonatologists, surgeons, nutritionists, ideally at a tertiary care facility.11,12Indications for surgical therapy in CD during pregnancy are the same as in non-pregnant patients, and include obstruction, perforation, hemorrhage, abscess, or ongoing disease activity despite medical treatment.13Even in healthy women, surgery during the first trimester carries an increased risk of miscarriage, while, in the third trimester, laparotomy may be associated with technical difficulties and an increased rate of premature delivery.14,15Pregnant women admitted for CD more often have surgical disease than non-pregnant women.16However, the evidence level is weak, and data regarding surgical procedures in pregnant women for complicated CD are scarce. A systematic literature review identified a total of 20 patients, with the largest series having six cases.17We thus conducted a nationwide survey using the Groupe d’Étude Thérapeutique des Affections Inflammatoires du Tube Digestif (GETAID) Chirurgie network to investigate the outcome of surgery during CD and its consequences on both mother and child.
Materials and Methods
We conducted a retrospective multicenter study from the GETAID Chirurgie. Any woman with CD undergoing surgery during pregnancy was eligible, without time limitation. Data collected included age, disease duration, phenotype and localization of disease, smoking habit, prior intestinal surgery, number of pregnancies, concomitant treatments, indication for surgery, type of surgery, surgical approach, gestational age at surgery, surgical morbidity for mother and fetus, mode of delivery, gestational age at delivery, mode of delivery, birth weight, and neonatal complications. Only descriptive statistics were used.
Results
Characteristics of patients
A total of 15 cases were reported from 1992 to 2015, in 10 different tertiary French GETAID centers (Table 1). The mean age of patients was 28 years, with a mean disease duration of 6 years. Two patients did not have a diagnosis of CD before pregnancy; 10 patients had disease involving the ileum with penetrating complications. Three-quarters of patients were non-smokers. Concomitant treatments at time of surgery were mainly oral steroids and antibiotics in six and four cases, respectively. Only two patients were receiving anti-tumor-necrosis-factor (TNF) therapies (adalimumab or infliximab), and three were treated with azathioprine. Other treatments included 5-aminosalicylic acids (three cases), budenoside (two cases), and other (one case) (Table 1).
Summary of the 15 cases.
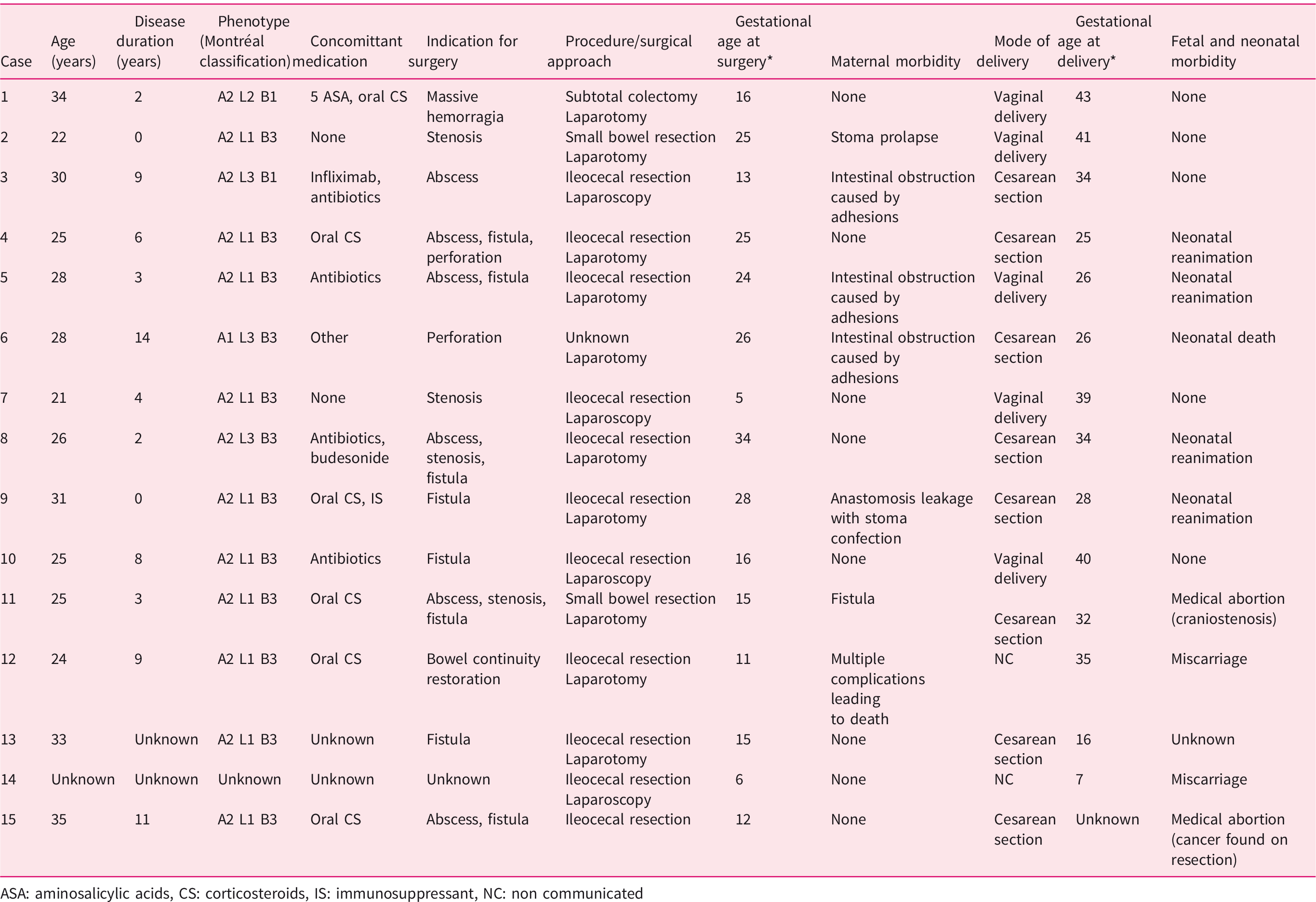
ASA: aminosalicylic acids, CS: corticosteroids, IS: immunosuppressant, NC: non communicated
Surgery and maternal outcomes
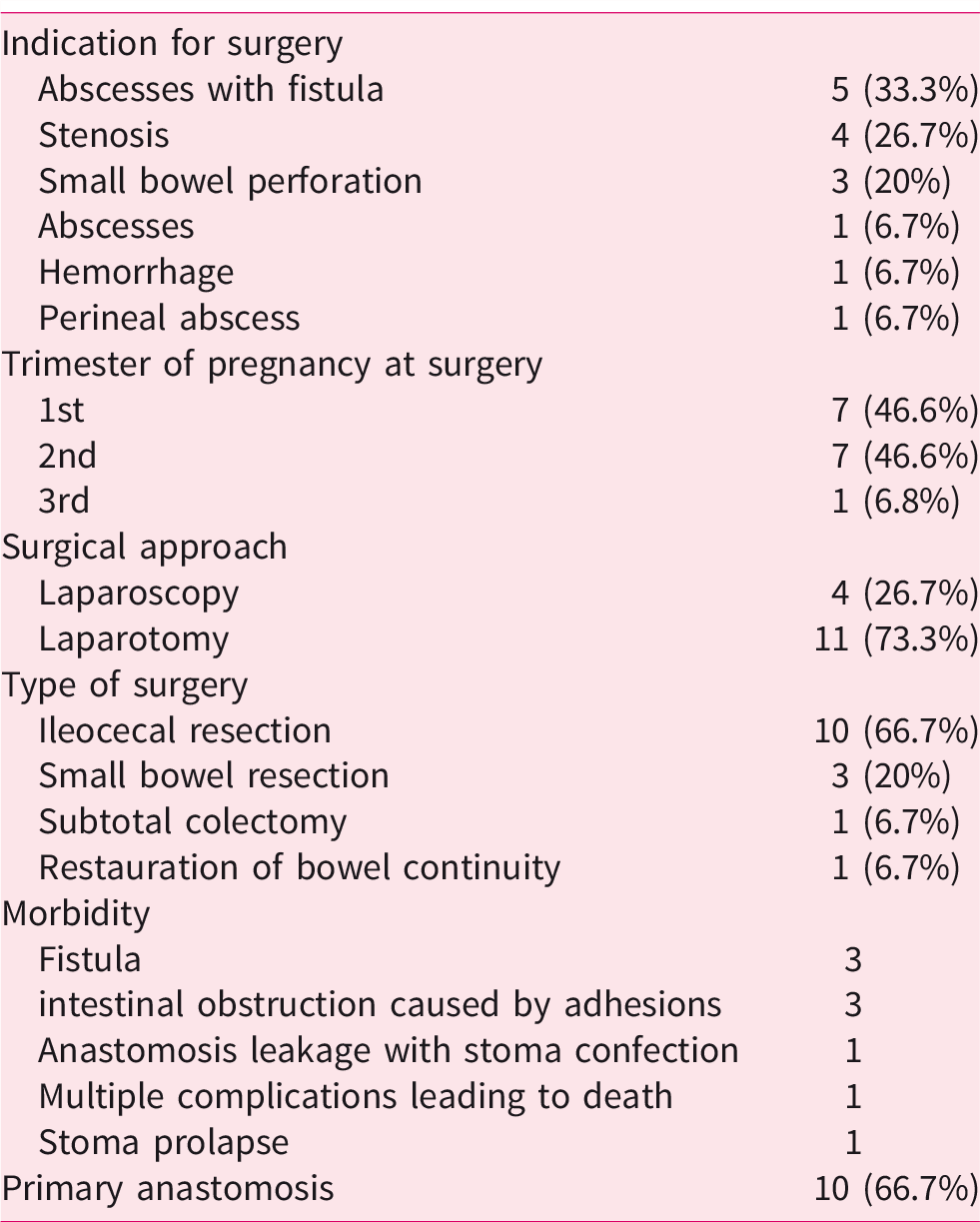
Indication for surgery was mainly abscess associated with fistula (five cases), stenosis (four cases), and small bowel perforation (three cases) (Table 1). Other indications were abscess without fistula, perianal abscess, and massive hemorrhage. Surgical approach was mainly laparotomy (11 cases). Only one patient underwent image-guided percutaneous drainage before surgery. Surgeries consisted of ileocaecal resection in 10 cases, small bowel resection in 3 cases, subtotal colectomy in 1 case, and programmed restoration of bowel continuity in 1 case. Primary anastomosis was made at the end of the procedure in 10 cases. Unfortunately, data about temporary ileostomies were often missing. Post-operative complications occurred in two-thirds of cases, with mainly fistulas (three, requiring stoma confection) and intestinal obstruction caused by adhesion (three, all treated medically). There was one stoma prolapse. Maternal mortality rate was 6.7% (one patient died from multiples complications including stercoral peritonitis and hemorrhagic shock) (Table 2).
Type of surgeries and surgical outcomes.
Delivery and obstetrical outcomes
Regarding pregnancy, half of patients were primiparous. Almost all surgeries were performed during the first or second trimester of pregnancy, with only one procedure during the third trimester. Mean gestational age at surgery was 18 weeks; 11 pregnancies led to delivery. There were two miscarriages and two medical abortions (one for craniostenosis and one because adenocarcinoma was found on operative specimen). The mean gestational age at delivery was 34 weeks (range 25–43 weeks), and delivery was vaginal in half of cases. Four cesarean sections were performed concomitantly to CD surgery. Birth weight was available only in seven cases and ranged from 850 g to 3500 g, with a mean of 2507 g. Four newborn required neonatal intensive care unit admission, with a neonatal mortality rate of 9.1% (one death).
Discussion
To our knowledge, this is the largest case series of surgery in CD pregnant patients, thanks to a nationwide collaboration effort of the GETAID Chirurgie. Our data are consistent with previous reports.17Characteristics of patients and indications for surgery are broadly similar. As in previous studies, most patients received steroids and only one-quarter was treated with azathioprine or a biologic. We reported the first case of maternal death after surgery for CD during pregnancy, although there may be a significant reporting bias. There was also more fetal mortality, even though this number is probably biased by two medical abortions, which did not result from surgical complications. Also, more patients underwent surgery in their first semester, which carries a higher risk of miscarriage.14We reported a higher rate of primary anastomosis, with a lower rate of surgical complications than previously seen. Unfortunately, information about temporary ileostomies was not available; stoma confection with secondary anastomosis should be considered during emergency surgery for CD.18While a minimally invasive approach was advocated by a number of authors because of fewer complications and shorter length of stay than the open approach,19only four surgeries were performed laparoscopically, with one conversion to laparotomy. Premature birth was observed in two-thirds of patients, which again is in line with previous cases.17The main strength of this study is that it is the largest case series of this rare event, with data collected from ten tertiary different centers thanks to a nationwide study. However, it has some limitations. First, this is a retrospective study and only descriptive statistics were used due to sample size. Second, all patients were managed by experienced multidisciplinary teams involving surgeons, gynecologists, and gastroenterologists working in GETAID centers, which are all centers of excellence for IBD management, and University Hospitals. Finally, no information regarding disease control at time of conception was available. This study underlines the complexity and potential risks of surgery for CD during pregnancy and might help clinicians who will be facing this issue in routine practice, even though more data are needed to draw definite conclusions. Emergency surgery should be performed at a tertiary center with neonatal and pediatric departments, and requires a multidisciplinary approach with input from an obstetrician, who should be readily available. The overall management and surgical procedure should be managed by physicians and surgeons with specific experience regarding CD. Decision to operate “medically refractory disease” should be discussed case by case, giving potential surgical complications. Surgical management of complicated CD during pregnancy needs to be tailored to maternal status, disease severity, and gestational age. However, in severely ill patients, continued illness poses higher risk to the fetus than the surgical procedure.20This case report series seems to confirm a significant morbidity and mortality for mother, fetus, and newborn. Achieving and maintaining disease remission is a key factor for successful pregnancy outcomes.
Footnotes
Specific author contributions
AD collected the data, revised and edited the manuscript for important intellectual content, TC wrote the first draft of the article and tables and contributed to the editing, LB-B, PZ, ZL, AA, AB, DL, JHL, SN, CS and LB collected the data and revised the manuscript for important intellectual content, LP-B contributed to editing of the manuscript and supervised the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The research was approved by the relevant institutional review boards or ethics committees in each center.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All human participants gave informed consent.