
Abstract
Background and study aims
Endoscopic submucosal dissection (ESD) is an optimal treatment for early gastric cancer (EGC) with negligible risk of lymph node metastasis; however, ESD is sometimes performed to treat lesions preoperatively contraindicated for the procedure due to various reasons. Here we aim to evaluate the treatment outcomes of ESD for lesions that were preoperatively contraindicated for ESD.
Patients and methods
Clinicopathological data of 104 EGC lesions in 104 patients were reviewed retrospectively. The demographic characteristics of patients, reasons for ESD, treatment results, complications, and outcomes were assessed.
Results
The major reasons for undergoing ESD included advanced age, desire to undergo ESD, and the existence of comorbidities. En-bloc and complete resection rates were 97 and 71%, respectively. Perforation and postoperative bleeding rates were 13 and 9%, respectively. Resection was beyond the expanded Japanese criteria for endoscopic treatment of EGC in 87 patients (84%), 41 (47%) of whom underwent additional therapy, including subsequent gastrectomy (29 patients) and photodynamic therapy (12 patients). The median follow-up period was 47 months, during which seven patients died from recurrent disease. The 5-year overall and disease-specific survival rates were 70 and 91.5%, respectively.
Conclusions
ESD is a technically demanding procedure for lesions preoperatively contraindicated for endoscopic resection. The curative resection rate was low, but the 5-year disease-specific survival rate of 91.5% was favourable. In experienced hands, ESD may be a treatment option for patients not suitable for radical surgery, and the relevant risk of complications must be considered before treatment.
Keywords
Introduction
Endoscopic resection (ER) for early gastric cancer (EGC) is limited to lesions that have a negligible risk of lymph node metastasis. The Japanese Gastric Cancer Treatment Guidelines 2010 (version 3) has proposed indication criteria for EGC suitable for ER.
1
Based on a negligible risk of lymph node metastasis, these criteria include lesions with a preoperative diagnosis that fulfil the conditions showed in Figure 1. With regard to technical issues, ER is recommended for EGC that can be resected en bloc depending on lesion size and location, since piecemeal resection results in a higher risk of local recurrence.2–5
Criteria of early gastric cancer indicated for endoscopic resection and criteria of a curative resection.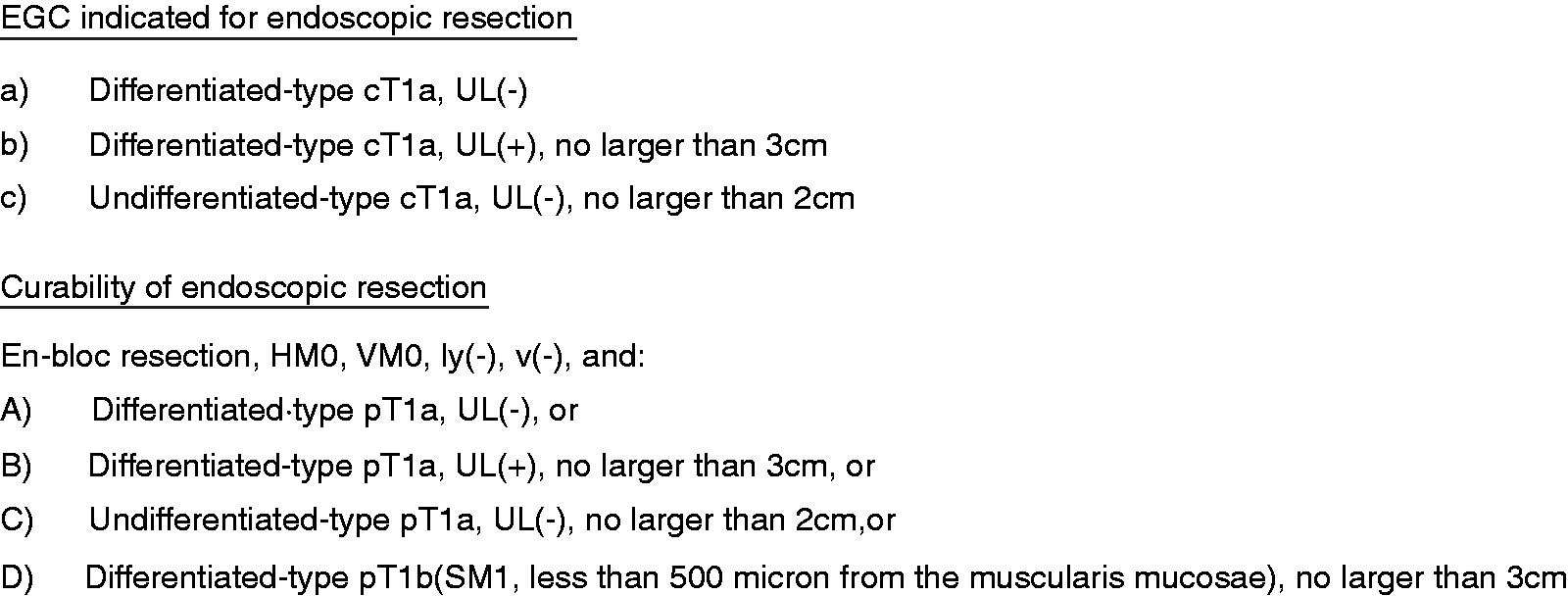
Endoscopic submucosal dissection (ESD) was developed to improve the en-bloc resection rate over that of endoscopic mucosal resection.2–7 Lesions that are considered impossible to remove en bloc by endoscopic mucosal resection are candidates for ESD. Therefore, it is important to decide whether a lesion should be treated by ESD taking into account of both cancer behaviour and technical issues. However, in some EGC patients, even though the lesion is preoperatively contraindicated for ER and should be treated by surgery, ER can be performed for various reasons. The aim of the present study was to investigate the present use and treatment outcomes of ECG in patients who were preoperatively contraindicated for ESD.
Methods
Patients
A total of 1576 patients with 1893 non-treated EGC lesions underwent ESD from September 2002 to December 2009 at Shizuoka Cancer Center Hospital (Shizuoka, Japan). A total of 104 patients with 104 lesions were preoperatively contraindicated for ER. Their primary physicians carefully explained the need for surgery to these patients and they received consultations from gastric surgeons. However, ESD was performed as an initial treatment for these patients. The reasons for ESD, clinicopathological characteristics, treatment results, and outcomes were retrospectively assessed.
The medical records of the 104 patients were retrospectively analysed with regard to demographics, concomitant diseases, preoperative endoscopic findings, histological findings of the ESD specimen, and additional treatment after ESD. Treatment results included the en-bloc resection rate, en bloc with complete (R0) resection rate, curative resection rate (fulfil all the conditions of curability criteria in Figure 1), and complication rate of bleeding that required haemostasis and perforation. Treatment outcomes, including local recurrence, distant metastasis, and overall survival and disease-specific survival rates were analysed.
The risks and benefits of ESD were carefully explained to every patient and written informed consent was obtained from each in accordance with our institutional protocol prior to undergoing ESD. This retrospective study was approved by the ethical committee of Shizuoka Cancer Center Hospital (approval no. 25-J12-25-1-3).
Preoperative evaluation before ESD
Before ESD, all patients were evaluated by oesophagogastroduodenoscopy with or without endosonography. A biopsy of the lesion was performed to diagnose the histological cancer type before ESD. When the lesion did not fulfil the indication criteria as shown in Figure 1, it was judged as contraindicated for ER. Before ESD, computed tomography was performed to evaluate the absence of nodal or distal metastasis.
Histological assessment of the ESD specimen
When the lesion was removed in one piece with negative margins of tumour, it was considered as en bloc with R0 resection. According to the Japanese Gastric Cancer Treatment Guidelines 2010 (version 3), 1 a resection was deemed curative when all of the conditions shown in Figure 1 were fulfilled. A resection that did not satisfy any of the curative resection criteria was considered non-curative.
Statistical analysis
Survival time was calculated as the interval between the date of ESD and the date of death or the last confirmed date of being alive. Survival curves were calculated using the Kaplan–Meier method. The Cox proportional hazards model and log-rank test were used for survival analysis. All analyses were performed with Excel Statistics 2012 software (Social Survey Research Information Co, Tokyo, Japan).
Results
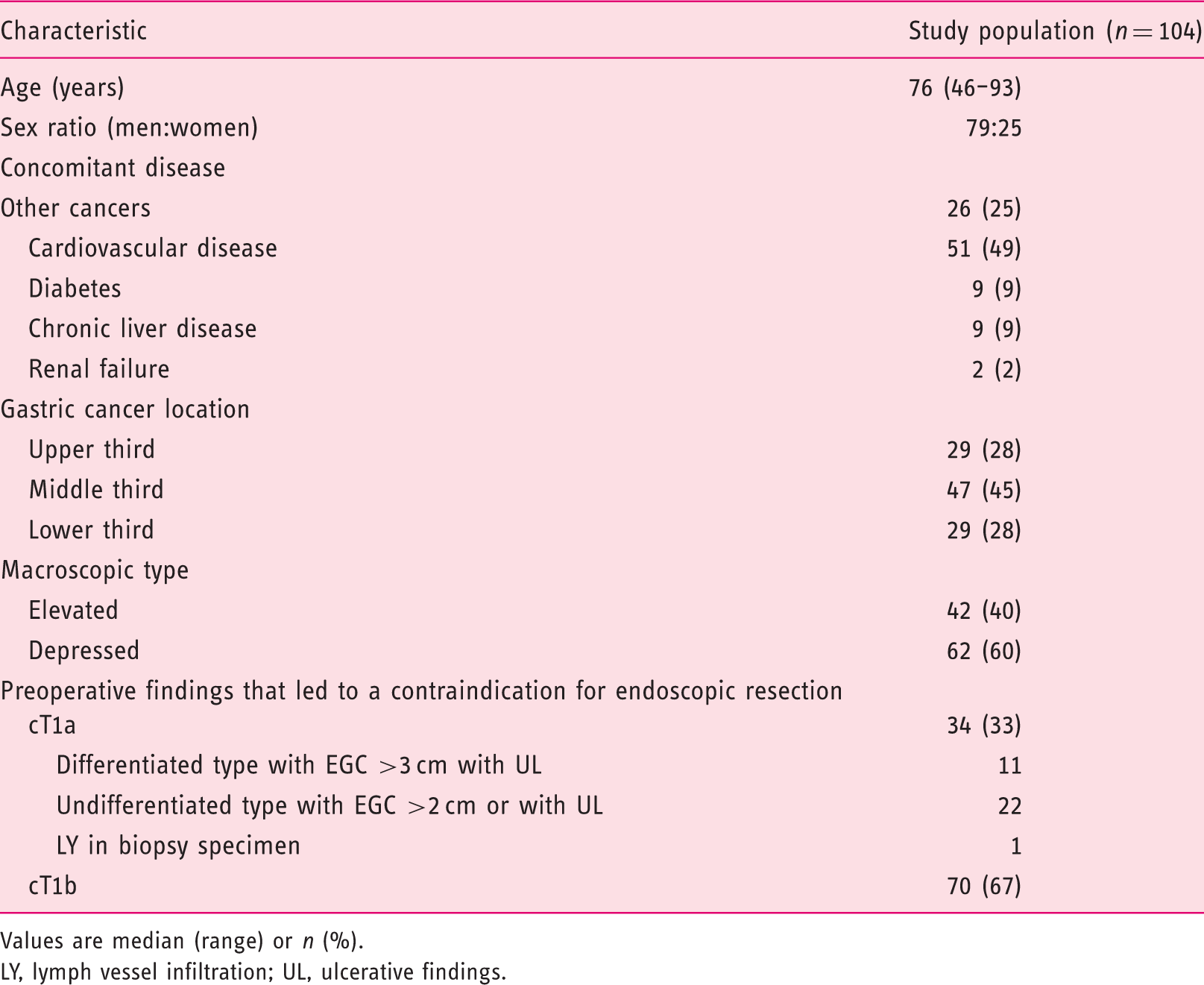
Demographic and tumour characteristics are summarized in Table 1. Preoperative findings that led to a contraindication for ER included lesions diagnosed as cT1a (34 lesions, 33%), among which 11 were diagnosed as differentiated type EGC >3 cm with ulcerative findings and 22 were diagnosed as undifferentiated type EGC >2 cm or with ulcerative findings. In one lesion, lymph vessel infiltration was diagnosed following biopsy. A diagnosis of cT1b was made for 70 lesions (67%). The diagnosis of cT1b in these patients was made by endoscopic findings such as clear depression with hardness or two-step elevation of the lesion during oesophagogastroduodenoscopy (Figure 2), and an additional endosonography was performed in 33 lesions. After ESD, 73% of these lesions (51/70) were diagnosed as pT1b.
Chromoendoscopy pictures of 0-IIc lesions. (a) Lesion showing a well-demarcated depression, which showed hardness by deflating the air during oesophagogastroduodenoscopy, leading to a diagnosis of cT1b; the lesion was diagnosed pT1b after ESD. (b) Lesion showing a two-step elevation, with the surface being reddish and rough, leading to a diagnosis of cT1b. The lesion was diagnosed pT1b after ESD. Demographic and tumour characteristics of patients who underwent endoscopic submucosal dissection for early gastric cancer preoperatively contraindicated for endoscopic treatment Values are median (range) or n (%). LY, lymph vessel infiltration; UL, ulcerative findings.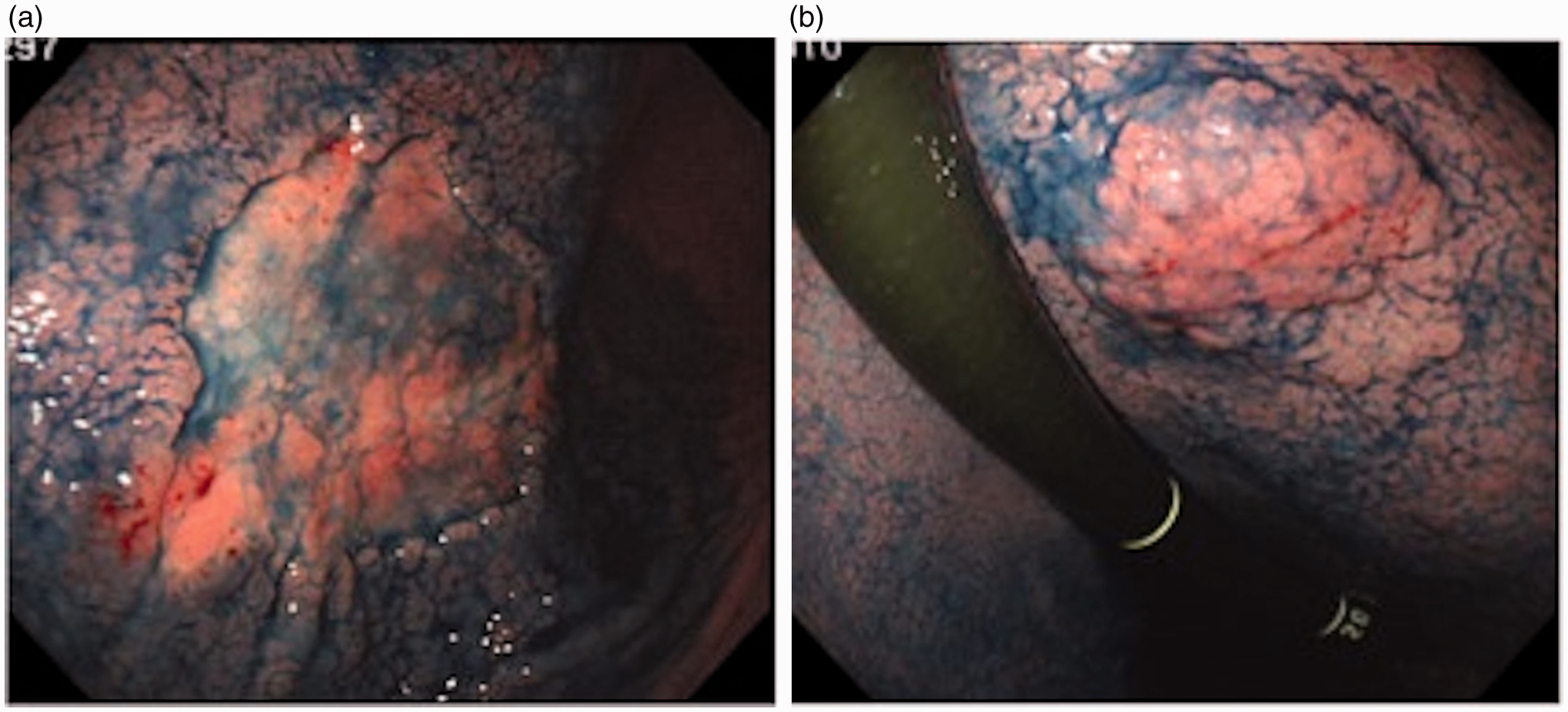
Reasons for endoscopic submucosal dissection
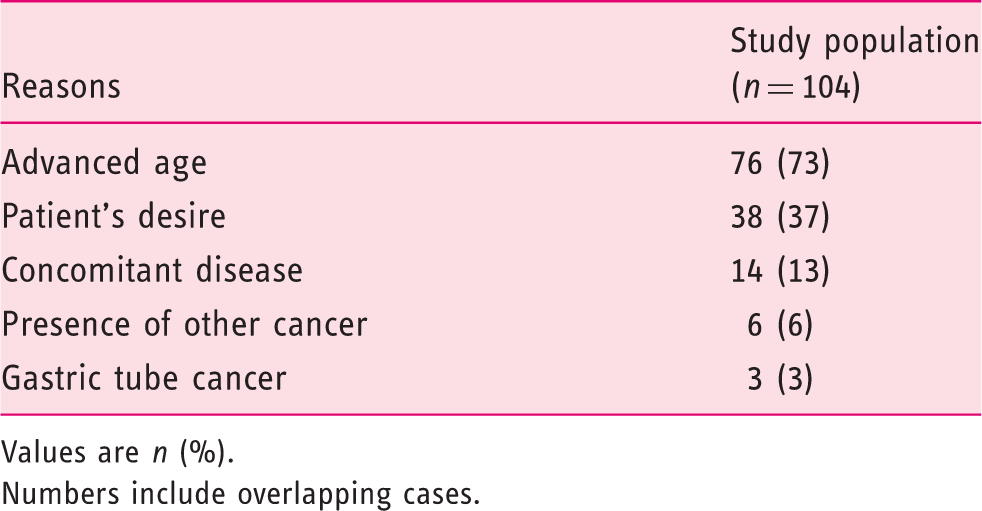
Values are n (%).
Numbers include overlapping cases.
Treatment results
Short-term ESD outcomes in 104 EGC patients who were preoperatively contraindicated for the procedure
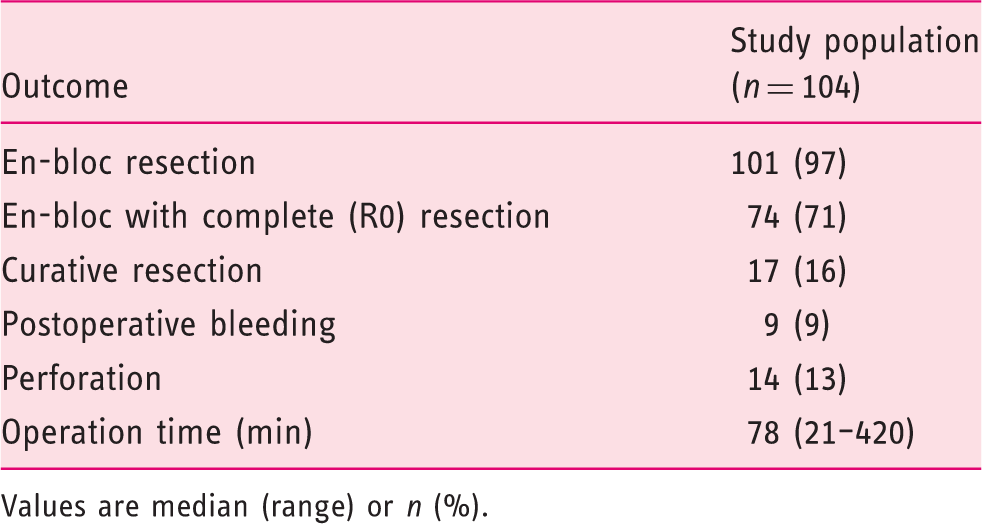
Values are median (range) or n (%).
The characteristics of lesions judged as curatively resected are summarized in Table 4. Although these lesions were preoperatively contraindicated for ESD, 17 (16%) of 104 lesions were judged as curatively resected after histological assessment of the specimen. Twelve of the 17 (70%) curatively resected patients were falsely classified as EGC invading the submucosa. A preoperative diagnosis was undifferentiated type cT1a >2 cm in another three lesions, however the final diagnosis was differentiated dominant type pT1a. The other two lesions were preoperatively diagnosed as differentiated type cT1a with ulceration finding (UL) >3 cm; however, the final diagnosis was differentiated type pT1a without UL (Figure 3).
Endoscopic images of lesions showing central redness and fold convergence. (a) Depressed lesion, leading to a diagnosis of 0-IIc with ulcer scar; the lesion was diagnosed as pT1a without ulceration finding after ESD. (b) An elevated lesion, leading to a diagnosis of 0-IIa with ulcer scar; the lesion was diagnosed as pT1a without ulceration finding after ESD. Characteristics of lesions that were judged as achieving curative resection after preoperative contraindication for ESD SM1, submucosal invasion <500 µm below the muscularis mucosa; UL, ulcerative findings.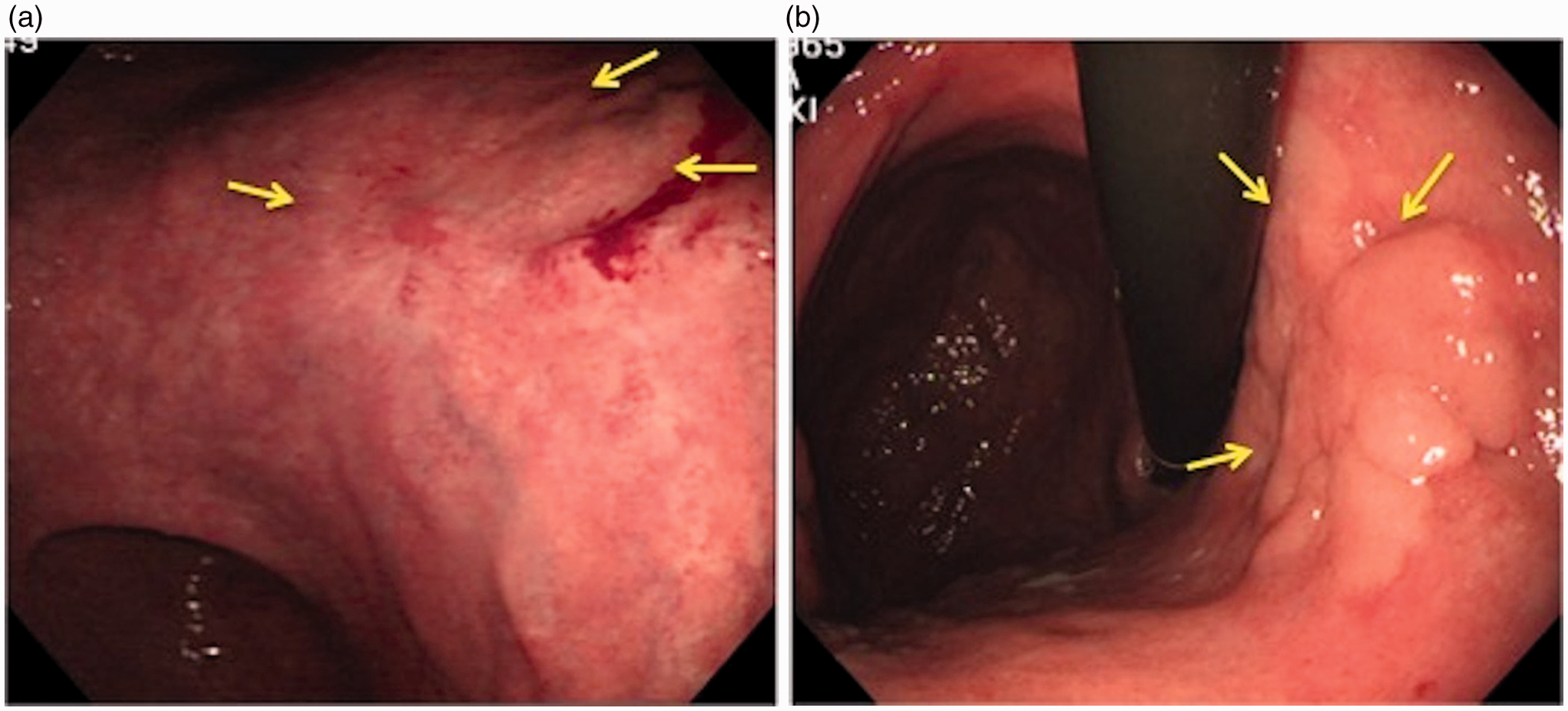

Among the 87 (84%) of 104 patients with non-curative resections, 41 (47%) underwent additional treatment. Once again the need for radical surgery was carefully explained to each patient and 29 patients agreed to undergo subsequent surgery. Of these patients, 19 patients were positive of lymphovascular infiltration, seven patients had massive submucosal invasion, and the other three patients had other factors of non-curative resection. The remaining 12 patients refused surgery and received photodynamic therapy (PDT). Of the 29 patients who underwent additional surgery, 18 had neither residual cancer nor lymph node metastasis, six had residual cancer without lymph node metastasis, and five had lymph node metastasis only. Among the 18 patients with no residual cancer or lymph node metastasis, the histology was differentiated type in 15 patients: 10 had lymphovascular infiltration, six had massive submucosal invasion, and three patients had positive deep margins of the ESD specimen.
Reasons for not undergoing additional therapy in the remaining 46 patients included concomitant diseases (unfit for surgery), presence of another cancer, advanced age, and patient refusal. In five (11%) of 46 lesions, observation was chosen by the physician because the only reason for non-curative resection was an indefinite tumour margin.
Outcomes
The median follow-up period was 47 months (range 1–126 months). Local recurrence was detected in three patients and distant metastasis in six patients. A total of seven patients died from gastric cancer. The 5-year overall and disease-specific survival rates were 70% (95% CI 0.59–0.80) and 91.5% (95% CI 0.85–0.97), respectively.
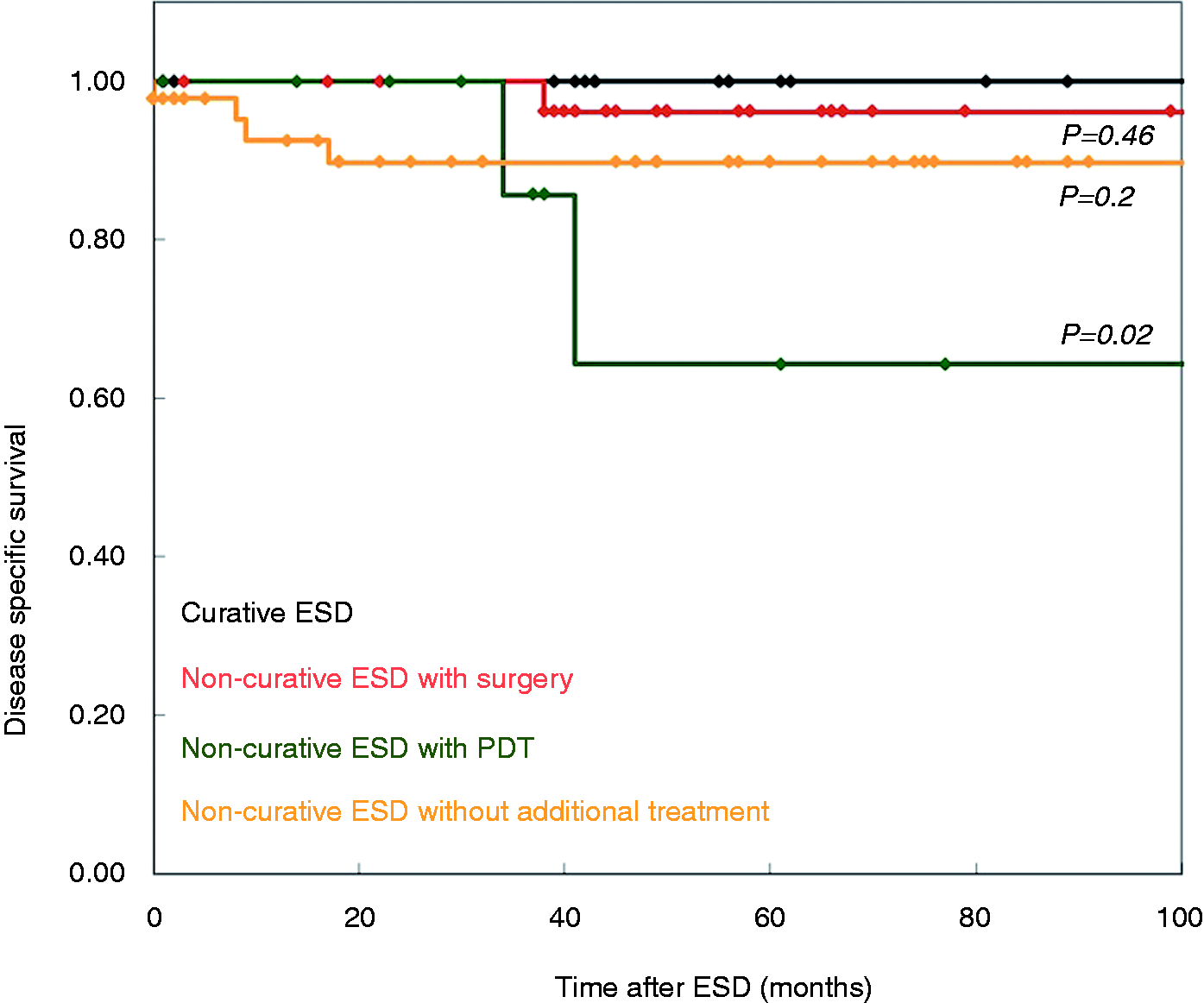
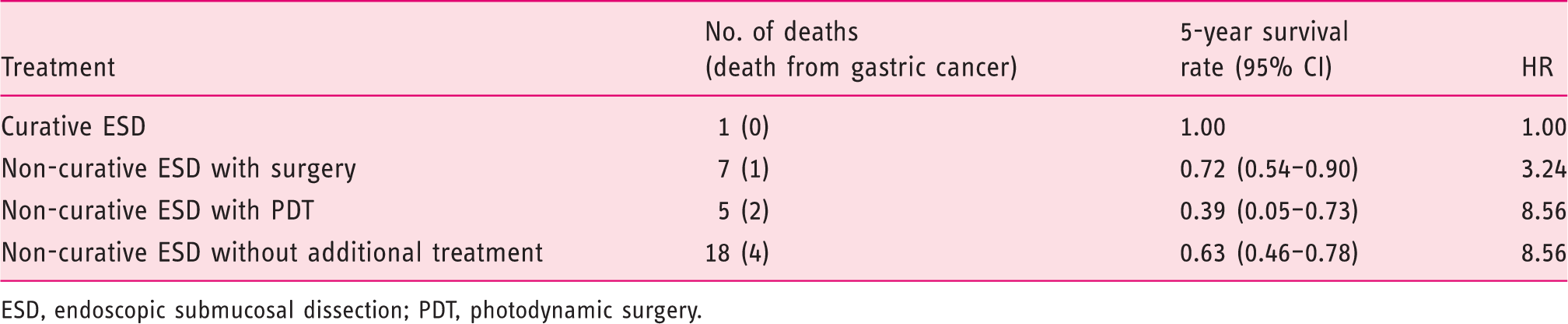
The 5-year overall survival rates for patients following curative ESD, non-curative ESD with surgery, non-curative ESD with PDT, and non-curative ESD without additional treatment were 100, 72, 39, and 63%, respectively (Figure 4 and Table 5). The hazard ratios for overall survival in patients following non-curative ESD with surgery, with PDT, and without additional treatment compared with those who underwent curative ESD were 3.24, 8.56, and 8.56, respectively (Table 5). There was no significant difference between the 5-year disease-specific survival rates among patients who underwent curative ESD, non-curative ESD with surgery, and non-curative ESD without additional treatment, (100, 96, and 89%, respectively) (Figure 5). However, the 5-year disease-specific survival rate of patients who underwent non-curative ESD with PDT was significantly low as 64% (p = 0.02; Figure 5).
Kaplan–Meier analysis of overall survival among patients following curative ESD and non-curative ESD with or without additional treatment. Kaplan–Meier analysis of disease-specific survival among patients following curative ESD and non-curative ESD with or without additional treatment. Hazard ratios of overall survival according to curability of ESD and additional treatment ESD, endoscopic submucosal dissection; PDT, photodynamic surgery.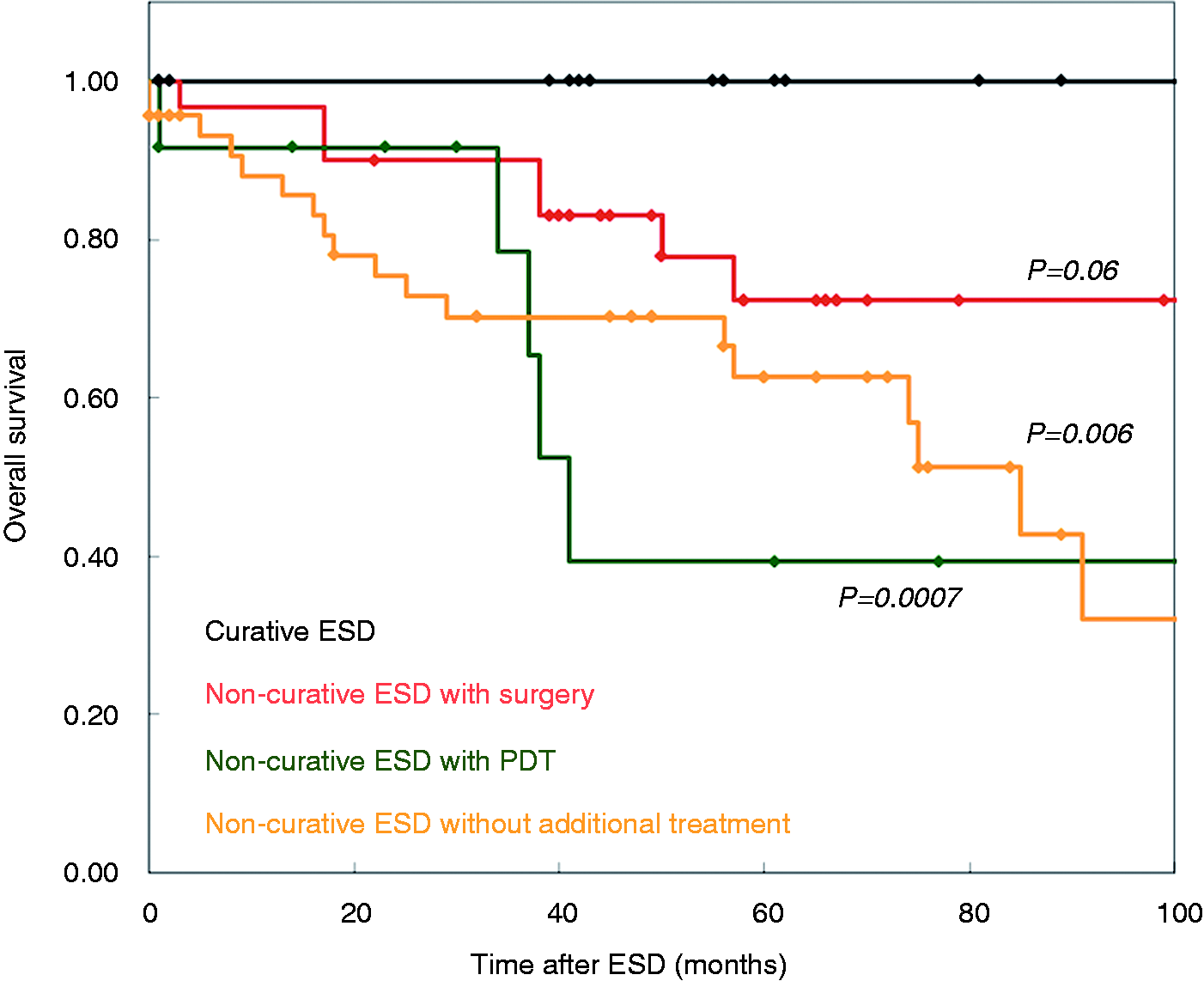
Discussion
Radical surgery is an accepted standard treatment for EGC. Patients who are preoperatively assessed with a negligible risk of lymph node metastasis are candidates of ER; additional surgery is recommended if the resection is judged as non-curative.8,9 However, surgery may not be an optimal treatment option for all EGC patients with a risk of lymph node metastasis because it carries a significant risk of morbidity and mortality.10–12
Our study showed a low complete resection rate of ESD performed for lesions preoperatively assessed as contraindicated for ESD, which was clearly lower than those for lesions indicated for ER reported in previous studies.13–15 Among previous reports regarding the feasibility of ESD for contraindicated lesions, a low complete resection rate of 55.6% (10/18) was reported for undifferentiated cancer and 36.6% (15/41) for submucosal invasive cancer. 16 Regarding the depth of EGC, the technical feasibility of ESD between pT1a (M) and pT1b (SM1) lesions was reported as the same regarding the complete resection and complication rates. 17 However, for pT1b (SM2) lesions (invasion of 500 µm or deeper below the muscularis mucosa), the complete resection rate was significantly low (57.8%, 48/83) compared with pT1b (SM1). 18
Bleeding and perforation are major ESD complications. The complication rate for bleeding is reportedly 0–15.6, and for perforation 1.2–5.2%.19–22 In our series, the rate of postoperative bleeding and perforation reached 9 and 13%, respectively. Suzuki et al. 23 also reported a disappointing postoperative bleeding rate of 18.4% (7/38) and a perforation rate of 13.2% (5/38) among operable patients with cT1b EGC who refused surgery and underwent ESD. Regrettably, these data are insufficient to assess the technical validity of ESD for lesions preoperatively contraindicated for ER in terms of both complete resection rate and complication risk. In particular, the present ER indication criteria that were determined by a negligible risk of lymph node metastasis could also be interpreted as indices of lesions technically amenable to safe and reliable ESD.
Our data showed a 5-year disease-specific survival rate of 91.5% for patients who underwent ESD for lesions preoperatively contraindicated for ER. Similar results were shown in operable patients with cT1b EGC who underwent ESD as an initial treatment with a 5-year disease-specific survival rate of 91.8%. 23 Other studies reported similar 5-year disease-specific rates among patients who underwent non-curative ESD with or without surgery.9,18 In patients older than 75 years, additional surgery is recommended following non-curative ER. 24 Our study population mostly included patients with some reason to hesitate undergoing radical surgery as an initial treatment. Therefore, it is difficult to compare survival rates between patients who underwent non-curative ESD with additional surgery and those who did not undergo additional surgery due to poor physical condition. In fact, in our study, 23 of 29 patients who did not receive surgery after non-curative ESD died of other causes during the follow-up period.
Our study included 12 patients who underwent PDT after non-curative ESD but did not undergo surgery due to physical condition or refusal. The resected lesions were either pT1b with or without positive resection margins. PDT was employed to eliminate any local residual cancer cells after ESD. At present, PDT is considered as a palliative treatment for EGC patients who are contraindicated for curative endoscopic treatment or surgery. 25 The overall survival rate of patients who received PDT after non-curative ESD was low in our study; thus, it was difficult to determine the additional effect of PDT. Moreover, individual factors, such as comorbidities and reasons for non-curative ESD, ultimately influenced whether to administer additional treatment after ESD, thereby resulting in a possible selection bias.
In conclusion, ESD is a technically demanding procedure for lesions preoperatively assessed as contraindicated for ER. The curative resection rate was low and did not seem to play an important prognostic role. However, the 5-year disease-specific survival rate was favourable. In experienced hands, ESD may be a treatment option for patients not suitable for radical surgery and the relevant risk of complications must be considered before treatment.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.
Presentation
This study was presented at the 20th United European Gastroenterology Week held in Amsterdam, The Netherlands, 2012.