
Abstract
Background:
Patients with irritable bowel syndrome (IBS) often complain of worsening of symptoms after meal intake. Meal challenge tests have previously been used to study symptoms and pathophysiology in functional dyspepsia.
Objective:
The objective of this article is to evaluate differences in gastrointestinal (GI) symptom response to a standardized meal test in IBS compared to healthy controls.
Methods:
We included 67 patients with IBS and 16 healthy controls. After an overnight fast the subjects were served breakfast (540 kcal; 36% fat, 15% proteins, 49% carbohydrates; 8.9 g fiber). They completed visual analog scales assessing severity of six GI symptoms (abdominal pain, bloating, discomfort, nausea, gas, fullness) before breakfast and every 30 minutes up to 240 minutes after breakfast. The patients also completed a questionnaire (IBS-SSS) to assess IBS symptom severity during the preceding week. The course of symptom scores over time was analyzed using mixed models.
Results:
The meal was well tolerated and all subjects completed the test period. In patients, significant effects of time (initial increase to a maximum, followed by a return to baseline) were found for fullness, bloating, nausea and discomfort (all p values < 0.01 for linear, quadratic and third-order effect of time). In IBS patients, an independent significant association between IBS-SSS scores and all postprandial symptoms, except for nausea, was found (all p < 0.01). In controls, a significant linear, quadratic and third-order effect of time (all p < 0.0001) was found for fullness only. The difference in time course for bloating and discomfort between IBS patients and controls was confirmed when comparing the groups directly (significant time-by-group interaction effects, all p < 0.05), but not for nausea. On average, IBS patients scored significantly higher than controls on all symptoms, except for nausea (significant main effects of group, all p < 0.05).
Conclusions:
A standardized meal test seems to be a promising tool to study the symptom pattern in IBS and potentially to follow the effect of interventions.
Introduction
Irritable bowel syndrome (IBS) is a prevalent functional bowel disorder, affecting approximately 10%–20% of the population worldwide. 1 The disorder is defined by abdominal pain and/or discomfort related to changes in bowel habit,2,3 but the pathophysiology is multifactorial and not fully understood. 4 A consistent relation between symptoms and impaired gastrointestinal (GI) function has been hard to identify. Consequently, there are no reliable diagnostic tools or means of measuring disease severity and treatment outcome. The most commonly described alteration in IBS patients is the presence of visceral hypersensitivity, 5 usually measured using a barostat. Still, there is considerable overlap between the patient group and healthy controls, 5 and the usefulness of barostat assessments has been questioned.6,7
The majority of IBS patients believe that dietary factors contribute to their symptoms,8,9 and reports of postprandial worsening of symptoms as well as adverse reactions to one or more specific foods are common.10–13 Especially foods rich in fat and carbohydrates seem to cause problems. 10 The etiology behind this postprandial symptom response is not obvious and probably involves different factors in subsets of patients. The most comprehensible explanation involves a combination of exaggerated GI sensory and motor responses after food intake. Altered visceral sensitivity is associated with IBS symptoms 14 and increased visceral sensitivity has been demonstrated in IBS patients after duodenal lipid infusion as well as after a liquid meal.15–17 The postprandial colonic motor response is altered in IBS patients18–21 and small bowel motility abnormalities become more evident after food intake. 22 Other factors that could be involved include intolerance to specific foods, 23 carbohydrate malabsorption 24 and altered colonic fermentation, 25 together with ineffective gas handling, which is further impaired by lipids.26,27 Moreover, dysfunctional communication along the brain-gut axis 28 is most probably also of relevance for self-reported food intolerance in IBS, but existing studies have not delineated the relative importance of central versus peripheral factors for food-related GI symptoms.
Alterations of the autonomic nervous system have also been implicated in the pathophysiology of IBS as it modulates both gastrointestinal motility and sensitivity. Interestingly, there are studies showing that IBS patients have altered autonomic responses to a meal.11,29 The same group has also presented that IBS patients exhibit an altered cellular immune response to food intake. 30 In addition, changes in gut hormone secretion, both in the fasting state as well as postprandially, have been reported in IBS patients.31,32
Given all these observations, it seems that the response to a meal is of importance in the pathophysiology of IBS. Meal challenge tests have previously been used to study symptoms and pathophysiology in functional dyspepsia,33–35 but so far, few studies have used a standardized meal test to assess meal-induced symptoms in a large IBS population. Our aim was therefore to determine and evaluate the GI symptom response to a standardized meal challenge in IBS. We hypothesized that IBS patients would experience a postprandial increase in symptom severity that would not be present in healthy subjects.
Materials and methods
Subjects
We included patients meeting the Rome II criteria 2 for IBS recruited from our outpatient clinic. They were categorized into subgroups based on the predominant bowel pattern according to the Rome II criteria. 2 In addition, healthy controls recruited by advertisement were interviewed and completed a GI questionnaire to exclude chronic diseases and the presence of GI symptoms. All subjects signed an informed consent and underwent a physical examination as well as routine laboratory blood testing including transglutaminase antibodies for celiac disease. IBS patients also completed a three-day food diary assessing the nutrient intake during three representative days. The subjects were studied between September 2005 and October 2006.
The study protocol was approved by The Regional Ethical Review Board at the University of Gothenburg.
Study design
All medications with known effects on the gastrointestinal tract were discontinued at least 48 hours before the study. After an overnight fast, the subjects presented to the laboratory at 7:30 a.m. Demographic data including height and weight was collected to calculate body mass index (BMI). Subjects were served a breakfast of oat bran (27 g) with 50 g applesauce and 2 dl milk, 2 crispbreads with 10 g margarine and two slices of cheese (20 g), and 1 dl apple juice (540 kcal; 36% fat, 15% proteins, 49% carbohydrates; 8.9 g fiber). Subjects were instructed to ingest the entire meal and finish within 10 minutes. GI symptoms were assessed before breakfast (baseline) and every 30 minutes up to 240 minutes after breakfast.
For IBS patients, individual mean daily energy intake was calculated based on the three-day nutrient diaries. These results were compared with results from a nationwide Swedish dietary survey of 2000 adults. 36
Symptom assessment
GI symptoms (abdominal pain, bloating, discomfort, nausea, gas and fullness) were assessed using 100 mm visual analog scales (VAS). Each subject completed six separate scales, one for each symptom, ranging from “no sensation” to “very severe sensation” at the time points mentioned above. In addition, at baseline all patients also completed the IBS severity scoring system (IBS-SSS). 37 This is a well-validated IBS symptom score that is based on five items (severity and duration of pain, abdominal distension, bowel habit dissatisfaction, and interference with life in general) and uses VAS. The maximum score is 500 and patients can be categorized as having mild (75–175), moderate (176–300), or severe (>300) IBS. The presence of comorbid symptoms compatible with functional dyspepsia (FD) was evaluated by using dedicated questions in the Rome II Modular Questionnaire (pain or discomfort centered in the upper abdomen).38,39
Data and statistical analysis
SAS 9.2 was used to analyze the data, which are expressed as mean ± standard deviation (SD). Significance was set at p < 0.05.
Demographic and baseline characteristics were compared between groups using unpaired Student’s t tests for continuous variables and Pearson χ2-tests for categorical variables.
To analyze the time course of the six different symptoms following meal intake, mixed-model analyses were used with intercept and time as random effects (to model the within-subject structure of the data correctly), time (in minutes) as a continuous fixed-effect and VAS score at each different time point as the dependent variable. The beta coefficients in linear mixed-model analysis can be interpreted in the same way as beta coefficients in ordinary general linear models (regression or analysis of variance (ANOVA)), indicating the magnitude of change in the dependent variable if the independent variable increases by one unit (for continuous independent variables: regression) or the difference in the dependent variable between two groups (for categorical independent variables: ANOVA).
First, linear, quadratic and third-order effects of time (time, time 2 and time3, respectively) were estimated for each symptom in IBS patients and controls separately. These three effects of time were included as plotting of the observed data versus the estimated data based on the regression equations showed that the estimated curve closely matches the observed curve when the effect of time is modeled up to the third order, with only marginal improvement when the fourth-order effect is added. This was further confirmed by comparing the fit statistics of the models with and without the fourth-order effect of time. Therefore, models were limited to the third-order effect of time for parsimony.
Second, both groups were pooled in one analysis to test a putative main effect of group (IBS versus controls). A significant main effect of group indicates a significant difference in average VAS score between groups independent of time (upward or downward shift of the whole curve without change in shape/time course), with the beta coefficient representing the magnitude of this difference.
Third, putative interaction effects between group on the one hand and the linear, quadratic and third-order effect of time on the other were tested if the analysis in both groups separately suggested different effects of time in both groups. Significant group-by-time interaction effects indicate differences in the shape of the linear, quadratic and/or third-order parts of the symptom curve between groups, with the beta coefficient for the respective interaction effects representing the magnitude of this difference.
Results
Subjects’ descriptive and demographic characteristics
Subject characteristics
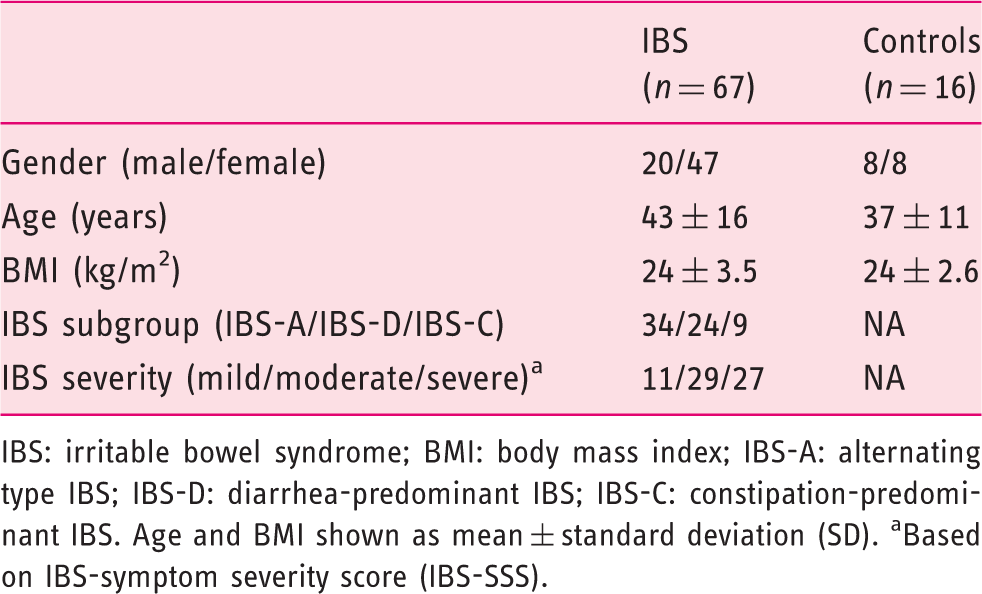
IBS: irritable bowel syndrome; BMI: body mass index; IBS-A: alternating type IBS; IBS-D: diarrhea-predominant IBS; IBS-C: constipation-predominant IBS. Age and BMI shown as mean ± standard deviation (SD). aBased on IBS-symptom severity score (IBS-SSS).
Meal challenge
The meal was well tolerated by all subjects and they all finished it within 10 minutes. All patients and healthy controls agreed that this was a meal that did not produce any intolerable symptoms, and therefore possible to eat again.
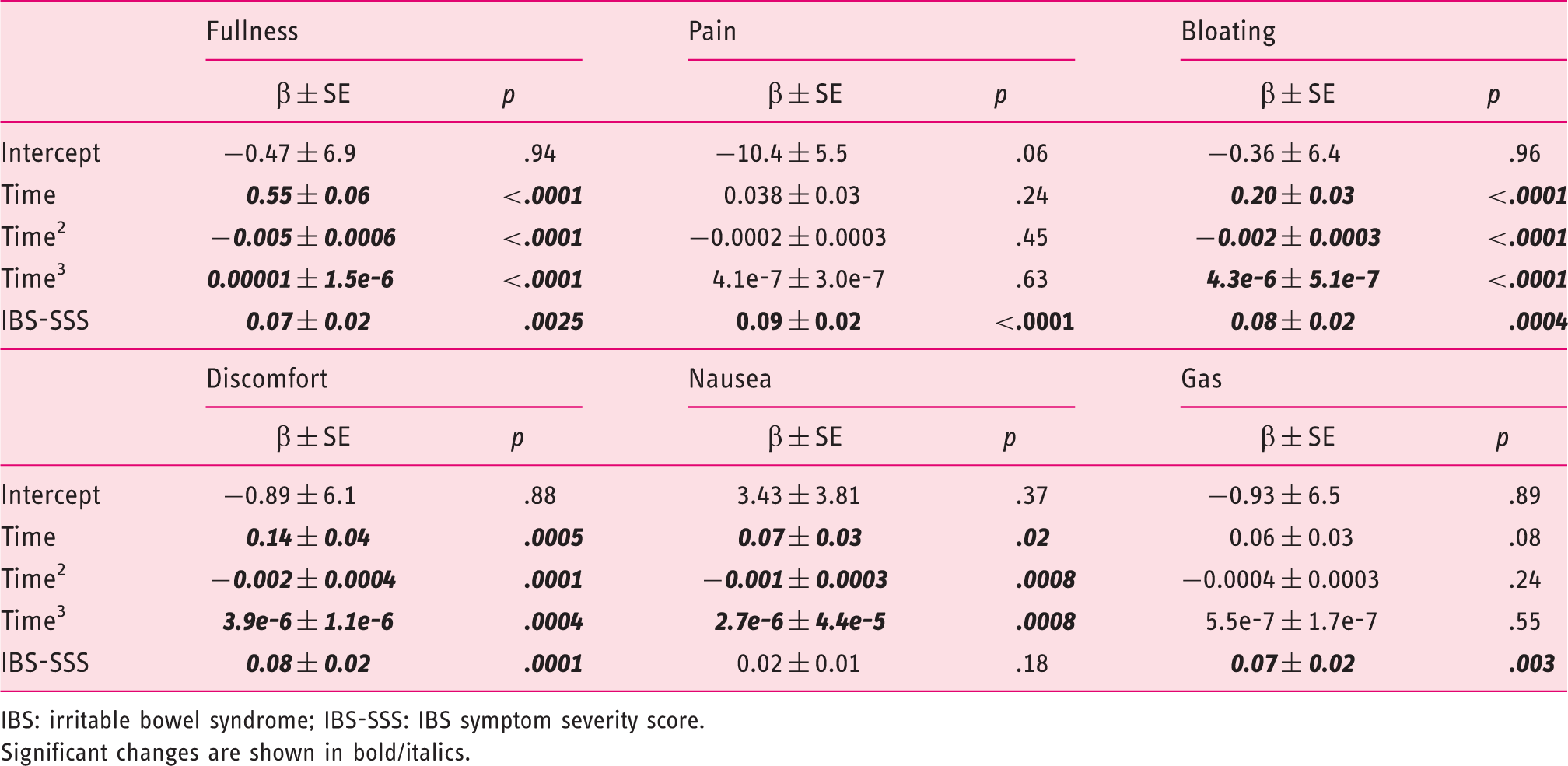
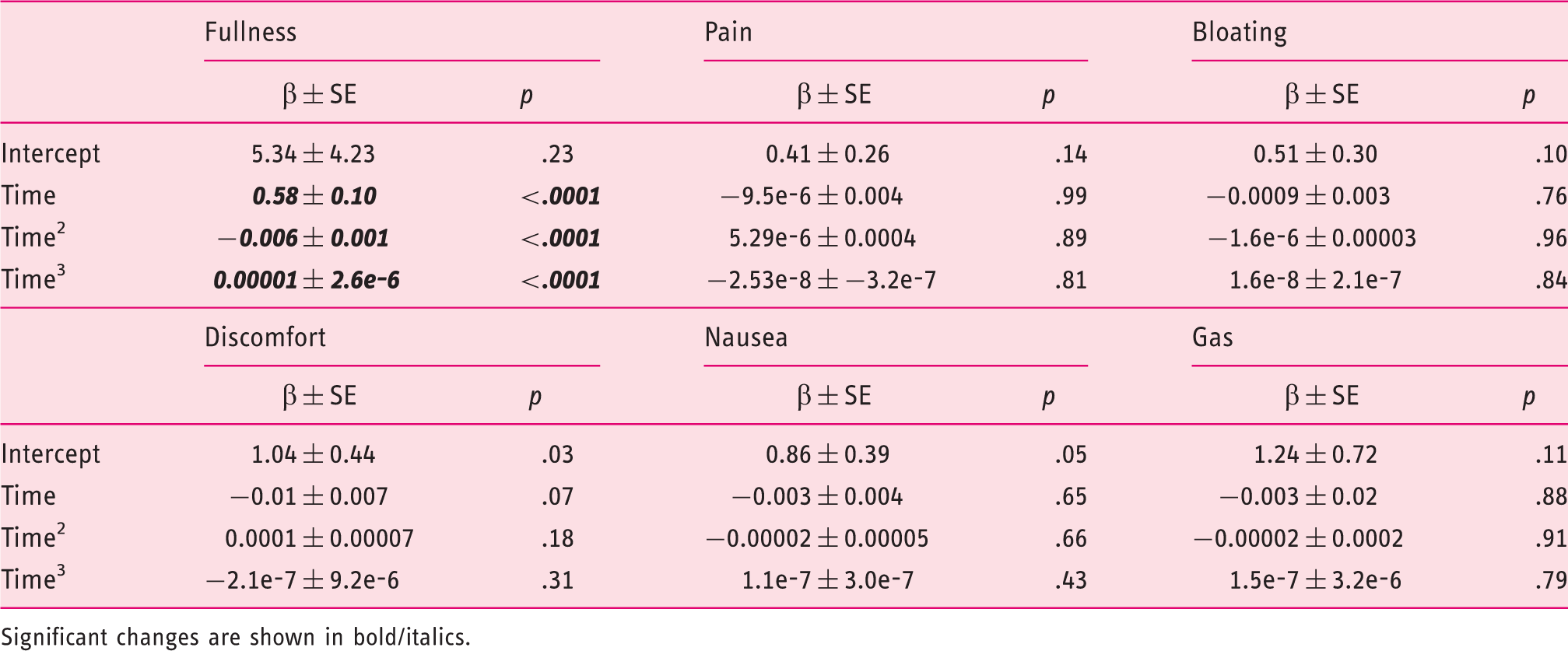
Time course of symptom scores for gas, bloating, discomfort, nausea, fullness and pain after a standardized meal in IBS patients. Data are shown as mean values. No measure of variability is included in order to enhance the appearance of the diagram. IBS: irritable bowel syndrome; VAS: visual analog score. Mixed-model analysis on the time course of six postprandial symptoms after a standardized breakfast in IBS patients IBS: irritable bowel syndrome; IBS-SSS: IBS symptom severity score. Significant changes are shown in bold/italics.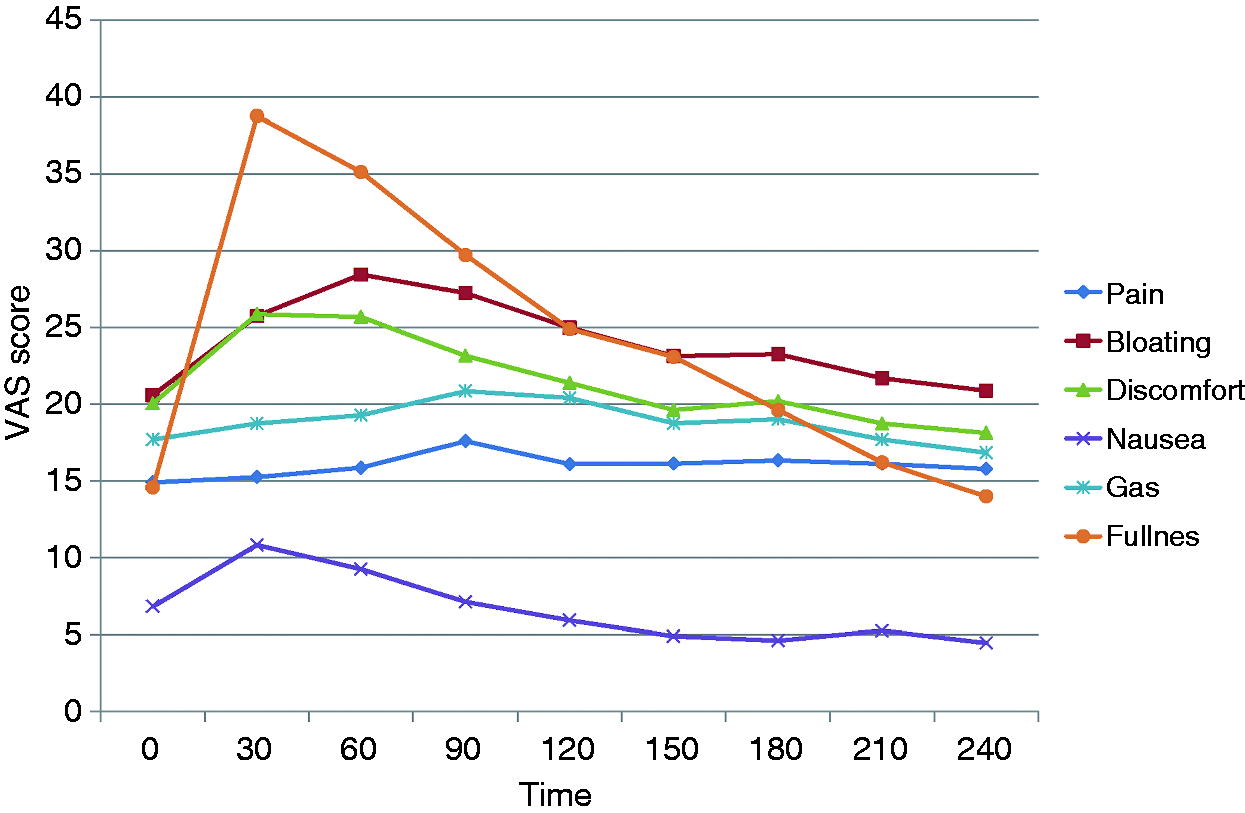
Effects of time on postprandial symptom ratings in IBS patients and healthy controls
IBS patients (Table 2, Figure 1)
Significant linear, quadratic and third-order effects of time were found for fullness, bloating, nausea and discomfort, whereas no significant effects of time were found for gas and pain. Further, an independent significant association between IBS-SSS scores and all postprandial symptoms, except for nausea, was found. Controlling for comorbid FD did not change the effects of time or IBS-SSS, nor was the effect of FD significant for any of the symptoms.
Time course of symptom scores for gas, bloating, discomfort, nausea, fullness and pain after a standardized meal in healthy controls. Data are shown as mean values. No measure of variability is included to enhance the appearance of the diagram. VAS: visual analog score. Mixed-model analysis on the time course of six postprandial symptoms after a standardized breakfast in healthy controls Significant changes are shown in bold/italics.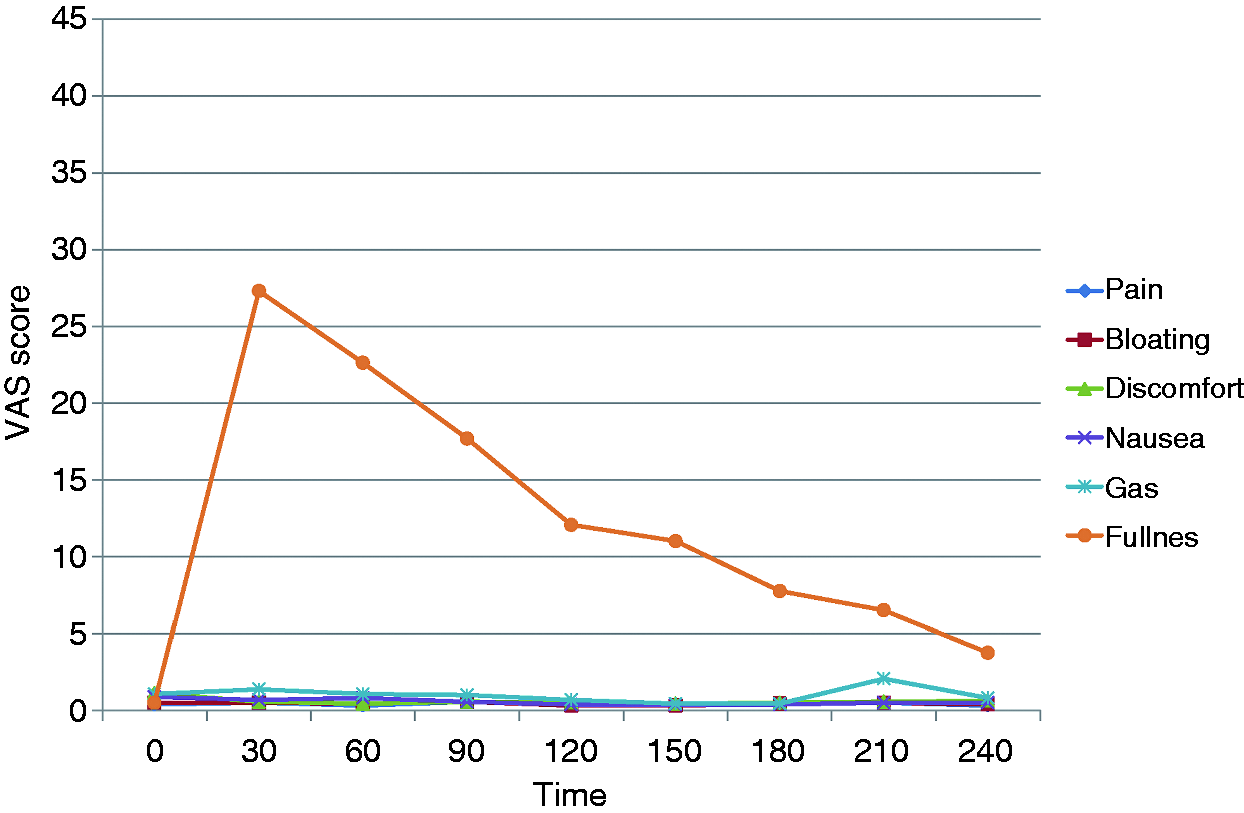
Healthy controls (Table 3, Figure 2)
Mixed-model analysis on the time course of six postprandial symptoms after a standardized breakfast: Main effect of group (IBS versus controls)
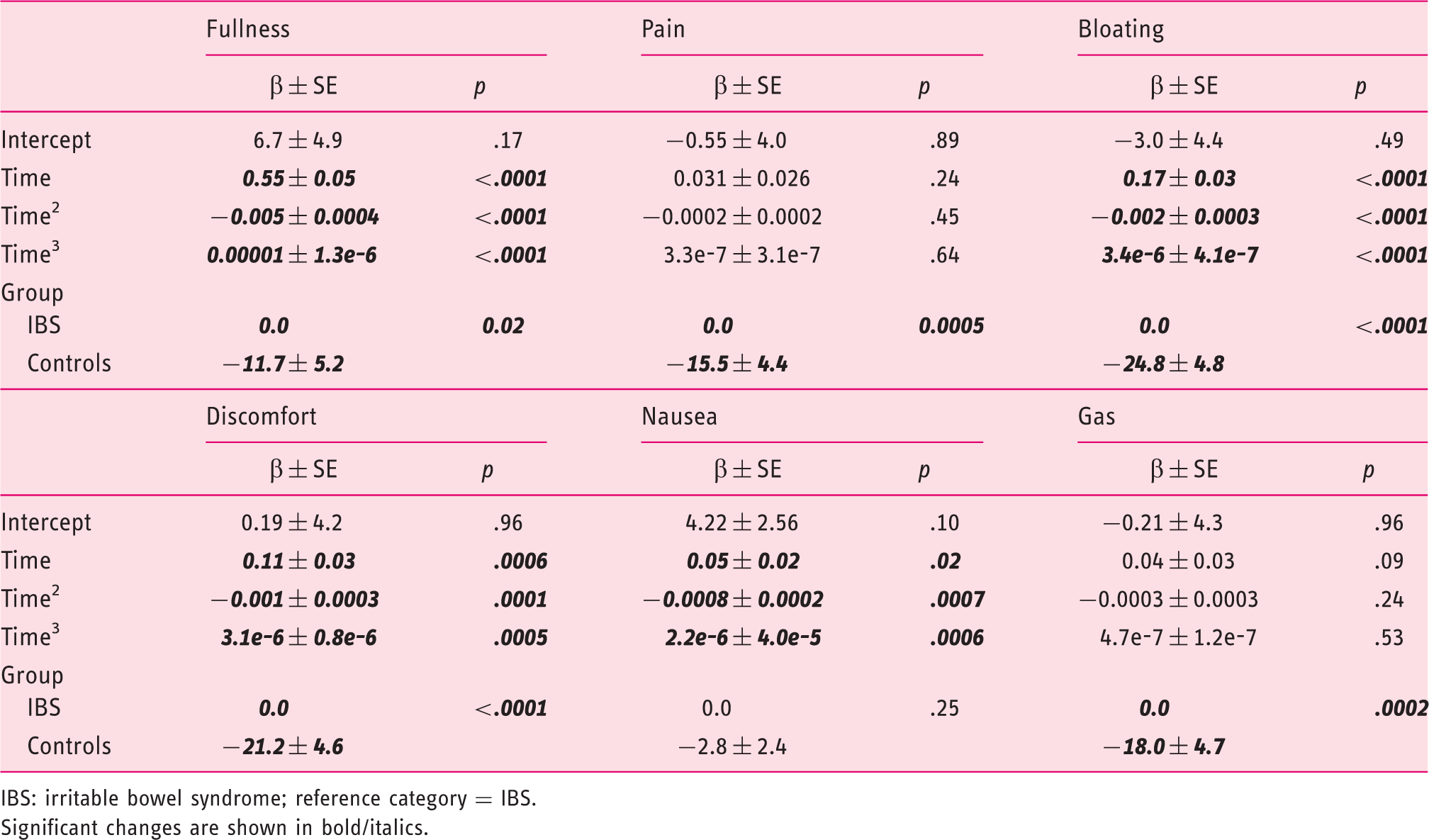
IBS: irritable bowel syndrome; reference category = IBS. Significant changes are shown in bold/italics.
Differences between IBS patients and controls
Main effect of group (Table 4)
Mixed-model analysis on the time course of three postprandial symptoms after a standardized breakfast in IBS patients and healthy controls: Group-by-time interaction effects
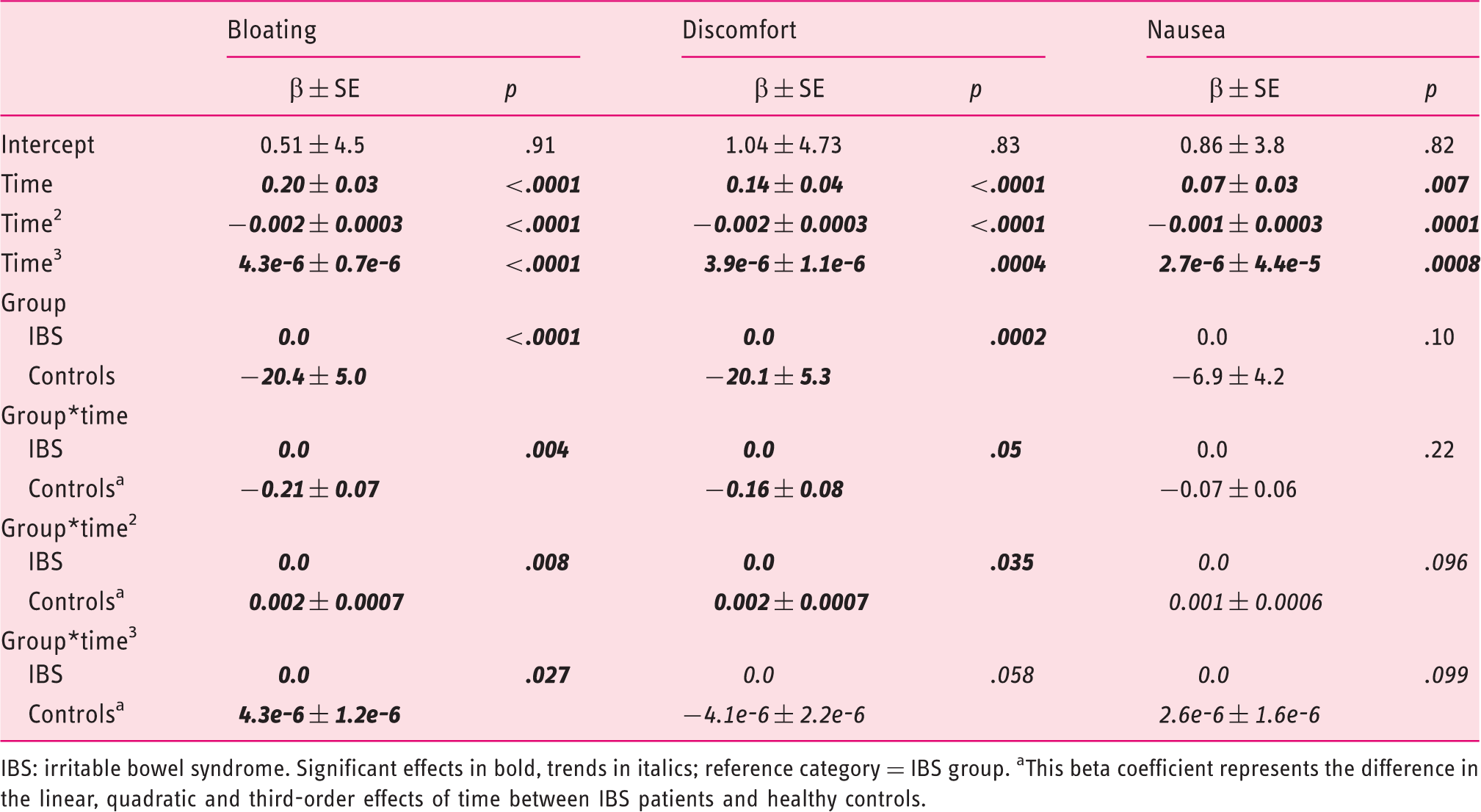
IBS: irritable bowel syndrome. Significant effects in bold, trends in italics; reference category = IBS group. aThis beta coefficient represents the difference in the linear, quadratic and third-order effects of time between IBS patients and healthy controls.
Group-by-time interaction effects (Table 5)
The analyses in IBS patients and healthy controls separately point toward differential effects of time on postprandial symptom ratings in both groups for bloating, discomfort and nausea (see above, Tables 2 and 3). To test the significance of these putative between-group differences directly, interaction effects between group on the one hand and the linear, quadratic and third-order time effects on the other were added to the respective models. Significant interaction effects between group and all three effects of time were found for bloating and discomfort, whereas the group-by-time2 and group-by-time3 interactions showed a trend for nausea. Controlling for comorbid FD did not change the effects of time, group or their interaction, nor was the effect of FD significant for any of the symptoms.
Discussion
Patients with IBS often report worsening of symptoms after meal intake.10–13 In the present study we studied a large cohort of IBS patients and systematically measured their response to a standardized meal challenge. We observed a significant GI symptom response in the patients for all symptoms except for nausea, whereas in healthy controls with similar demographic characteristics, such a response was found for fullness only. Interestingly, postprandial symptom severity was associated with overall IBS symptom severity at baseline. Several studies have previously reported that IBS patients show various alterations in their autonomic, immunologic and visceral response to food intake.11,15–22,29,30 However, to the best of our knowledge this is one of the first studies to propose a meal as a way to induce GI symptoms in IBS patients and compare their symptom responses to healthy controls, with the intention to create a tool for disease evaluation.
Visceral hypersensitivity, traditionally assessed by determining sensory thresholds during barostat distention of hollow viscera, is so far the most common, though not entirely consistent, pathophysiological alteration observed in IBS patients. 5 However, barostat procedures are invasive and cumbersome for investigators as well as patients, even to the extent that some patients will refuse to participate in these studies, potentially creating a selection bias. Also, it is hard to create protocols that diminish the problem with response bias for intensity rating during distention series. 6 Other means of assessing IBS patients are clearly needed, especially to evaluate interventions, aiming at reducing visceral sensitivity. The meal challenge presented in this study is a physiological challenge test that was well tolerated by patients and control subjects, and therefore has the potential to reduce selection bias and, similar to what was observed in FD and gastroparesis, to serve as a tool to evaluate new treatment options.40–42 A more challenging test meal should contain more fat and poorly absorbed carbohydrates, 10 but this would risk reducing the willingness to perform the test and therefore increase selection bias. Other advantages with this method are that no special preparations are needed and several tests can be performed in a short period of time at a low cost without any obvious risk of adverse effects. However, the meal test still depends on self-report measures and may therefore not be an entirely objective tool, but this also applies to barostat protocols for rectal sensitivity testing. Hypervigilance toward the GI tract and a tendency in IBS patients to label GI symptoms negatively6,7 may therefore contribute to some of the observed differences compared to controls. To fully elucidate the usefulness of this test, formal comparisons with the barostat should be performed, in addition to studies assessing the reproducibility of the meal test as well as the responsiveness to changes in symptom severity.
The average symptom levels during the challenge were clearly different between IBS and controls for all symptoms except for nausea, which is not a typical IBS symptom. This observation argues against a general tendency toward enhanced symptom rating in IBS contributing to the scores. With time, all symptoms except for pain and gas increased in patients, whereas only fullness increased in control subjects. The fact that pain did not increase during this test in patients may be viewed as a disadvantage on the one hand, but also as an advantage on the other hand, as pain-provoking tests are not attractive for patients and therefore a meal-test may potentially reduce selection bias. Moreover, IBS symptom severity based on IBS-SSS was significantly associated with the severity of all symptoms during the test, except for nausea, further strengthening its validity.
Of great importance, the symptoms generated were not affected by the presence of functional dyspepsia, further strengthening that this is a relevant test for generation of symptoms in IBS patients in general, and not only in those with coexisting upper GI symptoms. Controls also reported a postprandial increase in fullness, which could have been due to an interpretation of the term “fullness” as the opposite of “hungry.” It is likely that healthy subjects may have used “fullness” also in a positive sense to label their sensations of being full and satisfied after the meals, whereas more negatively charged symptoms were, as expected, not reported by control subjects.
Previous studies have reported that nutrients can enhance visceral sensitivity.15–17 This study did not aim to assess the possible mechanisms responsible for the observed meal-induced exacerbation of symptoms. Therefore no conclusions regarding this can be drawn, but the fact that symptom severity according to the IBS-SSS correlated with postprandial exacerbation could indicate that visceral hypersensitivity is somehow involved, as this has been associated with IBS symptom severity. 14 However, altered motor responses to meal intake could also be involved, as well as several other putative pathophysiologic alterations seen in IBS. 4 This should be explored in future studies.
One possible limitation of this study was that neither the caloric contents of the meal nor the serving size were individualized based on factors such as gender, BMI, or reported average meal size. It could be expected that some subjects found the meal to be too large, while others found it to be too small. However, there were no significant differences in reported symptoms depending on gender or BMI (data not shown), indicating that this did not have a substantial effect on the results. Moreover, to have a more challenging meal for IBS patients, a meal with a larger fat content and poorly absorbed carbohydrates could be considered. Another limitation is that patients who actually have a food allergy or intolerance to any of the ingredients, as well as vegetarians or vegans, would need a specially prepared meal. For this study we chose to exclude patients who reported lactose intolerance. However, the dairy products included in the meal could easily be substituted to equivalent lactose-free or nondairy products.
To conclude, we report results from a standardized meal challenge test that caused a significant increase in GI symptoms in IBS patients but not in controls. In contrast to some other procedures used in IBS research, this model is physiological, noninvasive and well tolerated. Further evaluation is warranted to establish reproducibility and association with other pathophysiologically relevant factors, such as psychological features,43–45 motility alterations, 46 visceral hypersensitivity 14 and gut microbiota composition, 47 but we believe that the meal challenge test is a promising tool that may be used to evaluate the effect of different interventions in IBS patients, as well as to provide relevant information about the pathophysiology of postprandial symptoms in IBS.
Footnotes
Funding
This work was supported by Arla Foods Innovation, The Swedish Medical Research Council (grants 13409, 21691 and 21692), The Marianne and Marcus Wallenberg Foundation, University of Gothenburg, Centre for Person-Centred Care (GPCC), Sahlgrenska Academy, University of Gothenburg and by the Faculty of Medicine, University of Gothenburg. Lukas Van Oudenhove is a postdoctoral research fellow of the Research Foundation-Flanders (FWO-Vlaanderen) and a research professor of the KU Leuven Special Research Fund. Jan Tack is supported by a Methusalem grant from Leuven University.
Conflict of interest
Iris Posserud, Hans Strid, Stine Störsrud, Hans Törnblom and Lukas van Oudenhove have nothing to declare.
Ulla Svensson was employed by Arla Foods Innovation and is now working at UKS Life Science Consulting AB.
Jan Tack has given scientific advice to: Almirall, AstraZeneca, Danone, Menarini, Novartis, Nycomed, Ocera, Ono pharma, Shire, SK Life Sciences, Theravance, Tranzyme, Xenoport and Zeria Pharmaceuticals, and has been member of the Speaker bureau for: Abbott, Almirall, AlfaWasserman, AstraZeneca, Janssen, Menarini, Novartis, Nycomed, Shire and Zeria.
Magnus Simrén has received unrestricted research grants from Danone, Arla Foods and AstraZeneca, and served as a Consultant/Advisory Board member for Danone, Novartis, Boehringer-Ingelheim and Shire/Movetis.