
Abstract
Background
Diverticular disease is the most common morphological abnormality of the colon and the fifth most important gastrointestinal disease in terms of cost in the Western world. Tower Hamlets is the poorest borough in London containing a large Bangladeshi community. We observed that emergency admissions with complications of colonic diverticulosis were minimal in the Bangladeshi community. The objective was to compare the background prevalence of colonic diverticulosis in Bangladeshis with other ethnicities in patients undergoing colonoscopy at a single centre in Tower Hamlets.
Methods
Four thousand four hundred and fifty-four consecutive colonoscopy reports over a 2-year period were retrospectively analysed. Patients under 40 years of age and repeat colonoscopies were excluded, leaving 3151 patients (mean age: 63 years; 48% male). Demographics including ethnicity and medical background were retrieved from the electronic patient record system and findings correlated with the prevalence of other ‘Western’ diseases in the cohort.
Results
Six hundred and thirty out of 3151 (20%) colonoscopies were performed on Bangladeshis. The prevalence of colonic diverticulosis was significantly lower in Bangladeshis (17/630: 2.7%) than Caucasians (673/1869: 36%), Indians/Pakistanis (16/161: 9.9%), Oriental (15/44: 34%) and Black (90/369: 24.4%) patient groups (χ2 p < 0.0001 for all comparisons). The prevalence of classical sigmoid diverticulosis in the Bangladeshi cohort was only 1.0%, despite significantly more Bangladeshi patients undergoing colonoscopy for abdominal pain (p < 0.0001, χ2) and diarrhoea (p < 0.0034, χ2). There was also a significantly greater incidence of type 2 diabetes mellitus and ischaemic heart disease (p < 0.0001, χ2) in Bangladeshi patients.
Conclusions
There is a negligible prevalence of colonic diverticulosis in the Bangladeshi population of London who undergo colonoscopy. This is in spite of a high incidence of type 2 diabetes and ischaemic heart disease. The effect of diet and genetics on the prevalence of colonic diverticulosis in Bangladeshis is not known and merits further investigation.
Keywords
Introduction
Diverticular disease (DD) is characterised by multiple mucosal herniations through the colonic wall. It is the most common morphological abnormality of the colon 1 with a clinical spectrum that extends from an asymptomatic incidental finding (colonic diverticulosis) to life-threatening faecal peritonitis. It is currently the fifth most important gastrointestinal disease in terms of direct and indirect costs in the Western world 2 and one whose prevalence is increasing 3 not least because of the well-established relationship between disease and advancing life expectancy. 4 There is also evidence of an increased incidence of DD and related complications in obese patients, 5 which can be anticipated to add further to future disease burden.
In spite of the high societal cost of DD, remarkably little is known of its pathogenesis. Among various aetiological theories, pulsion predominates.6–8 This postulates that increased local (segmental) pressures resulting from a diet that is chronically low in fibre, but high in refined sugar, leads progressively to physical extrusion of the mucosa through points of weakness in the muscularis propria. This theory, first purported by Burkitt in 19719 is supported by manometric 10 and demographic studies, 7 and also by epidemiological studies of populations migrating from areas of low incidence to those with a high incidence, for example Japanese Hawaiians 11 and African Americans. 12 This being accepted, there is no doubt that the aetiology of DD must involve both genetic and environmental factors. This is highlighted by both the site of diverticulosis, which changes with ethnicity, and the resistance of some populations to development of colonic diverticulosis despite embracing cultural dietary changes. In Japanese patients, right colonic diverticulosis is more prevalent 13 and patients from the Indian subcontinent have been found to have a lower incidence of colonic diverticulosis compared with British Caucasian patients. 14 Also, in the Netherlands, the immigrant population (the majority of whom are of Turkish descent) have a significantly lower incidence than the indigenous population. 15
Bangladeshi emigration to the UK began in earnest in the 1970s. Most have settled in London, in particular the borough of Tower Hamlets. More than 90% of Bangladeshis in the Tower Hamlets borough are from the District of Syhlet in north-eastern Bangladesh. 16 In 2007, the ethnic Bangladeshi population in England was estimated at 353,90017 and this is now thought to be around 500,000. The population of the Tower Hamlets borough of London was 254,200 in 2011 and census data suggest that Bangladeshis comprise approximately 30% of this population. 18 The Royal London Hospital (part of Bart’s Health National Health Service Trust) is situated in Whitechapel and is the largest hospital serving the Tower Hamlets community.
A clinical observation that emergency admissions with complications of DD were almost non-existent in Bangladeshis led to the hypothesis that there is a reduced background prevalence of colonic diverticulosis within the Bangladeshi population. While colonoscopy has not been used historically to determine prevalence of colonic diverticulosis, this is now the main diagnostic modality for organic colonic disease and has been used in some recent studies.19–21 On this basis, we performed a retrospective analysis of systematically-recorded colonoscopic data in an enriched consecutive cohort (aged >40 years) to test the hypothesis that prevalence of colonic diverticulosis was significantly lower in Bangladeshis compared with other ethnic groups. Findings were correlated with the prevalence of other ‘Western’ diseases in the cohort.
Methods
Endoscopic data collection
Endoscopic procedures at The Royal London Hospital have been recorded electronically since 2008 using the Endoscribe (Unisoft Medical Systems, Enfield, UK) system. This system permits a fixed number of descriptors for indications of colonoscopy from a drop-down menu. All consecutive records of patients over the age of 40 years from a 2-year period (January 2009–December 2011) were retrieved and analysed by one of two investigators (RL and AA), regardless of clinical indication for colonoscopy. This included some patients who had previously undergone colonoscopy prior to the study period. All patients included in the study had adequate colonic preparation that allowed visualisation to the caecum with ileal intubation rates also recorded. Patient demographics, indication for colonoscopy, site and extent of DD were recorded. Patients under the age of 40 years, repeat colonoscopies (during the study period) and patients with inadequate colonic preparation were excluded.
Ethnicity and comorbidities
Ethnicity was recorded using the secure trust-based online electronic patient record (EPR) where it is systematically recorded using a drop-down list of descriptors. In addition, in view of the Burkitt hypothesis, major medical comorbidities (cardiovascular disease, diabetes and obesity) were retrieved from the Endoscribe records, having been systematically questioned by admission staff. Obesity was defined as a body mass index >30 kg/m2. The presence of hypercholesterolaemia was retrieved from the EPR and defined as elevated levels of cholesterol in the bloodstream compared with the reference range and requiring treatment. Usage of regularly prescribed medications, such as aspirin 22 and steroids, 23 was also recorded as these have been shown to be independent risk factors for diverticular haemorrhage.
Analysis
Interobserver variability and potential performance bias were tested by taking a random subgroup of 200 reports, which were analysed by both investigators, one of whom was blinded to the patient’s name and ethnicity. Categorical frequency (incidence) data for different ethnicities were analysed using the χ 2 test with Bonferroni correction. Simple hypothesis tests (unpaired t-test or Mann–Whitney U-test) were used to analyse continuous data based on normality of distribution. A probability value of <0.05 was considered to indicate statistical significance. All data were analysed using Stata v.10 (Stata, College Station, TX, USA).
Results
Prevalence of DD by ethnicity
Demographics of patients undergoing colonoscopy

Indications and comorbidities of patients undergoing colonoscopy
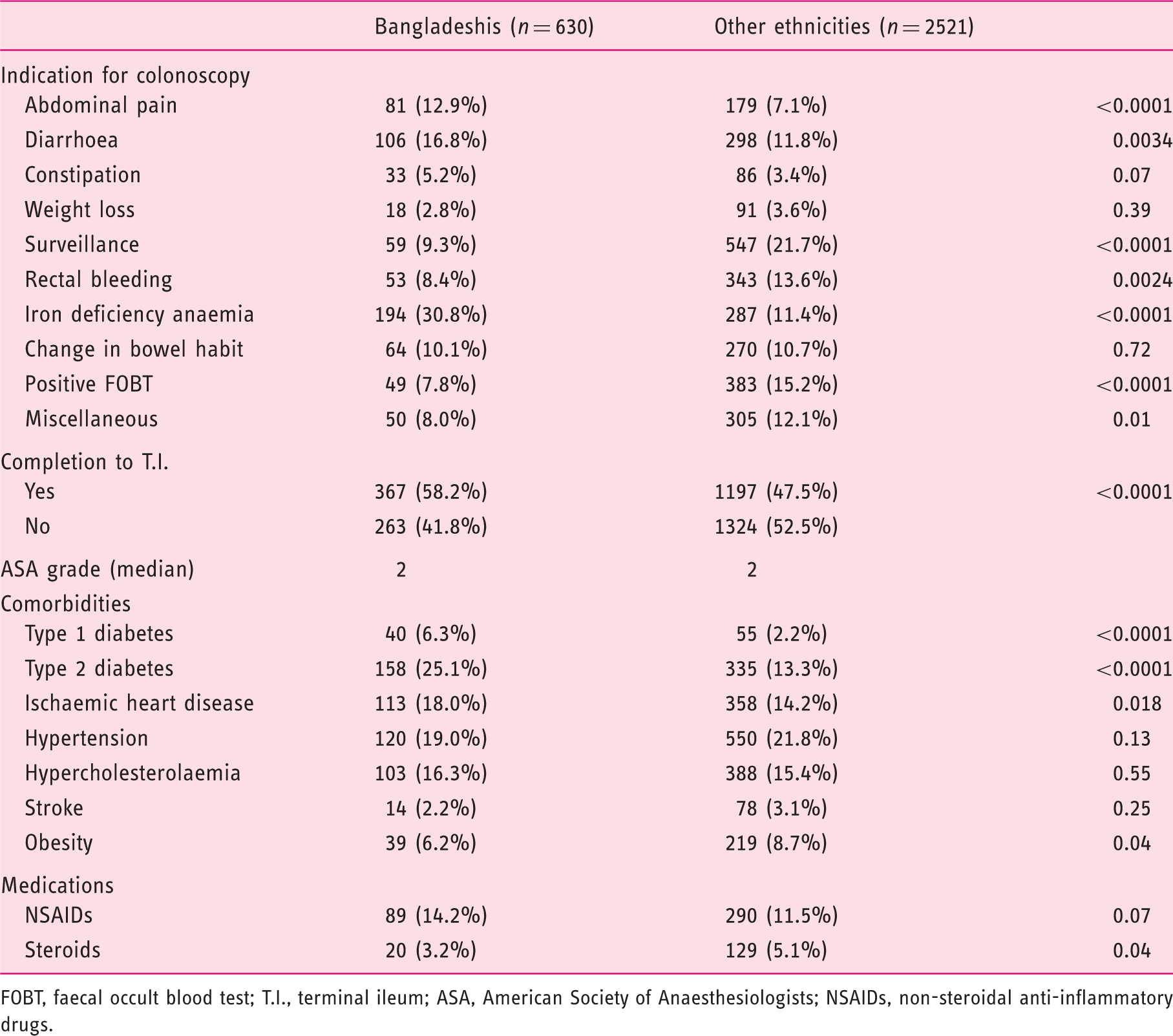
FOBT, faecal occult blood test; T.I., terminal ileum; ASA, American Society of Anaesthesiologists; NSAIDs, non-steroidal anti-inflammatory drugs.
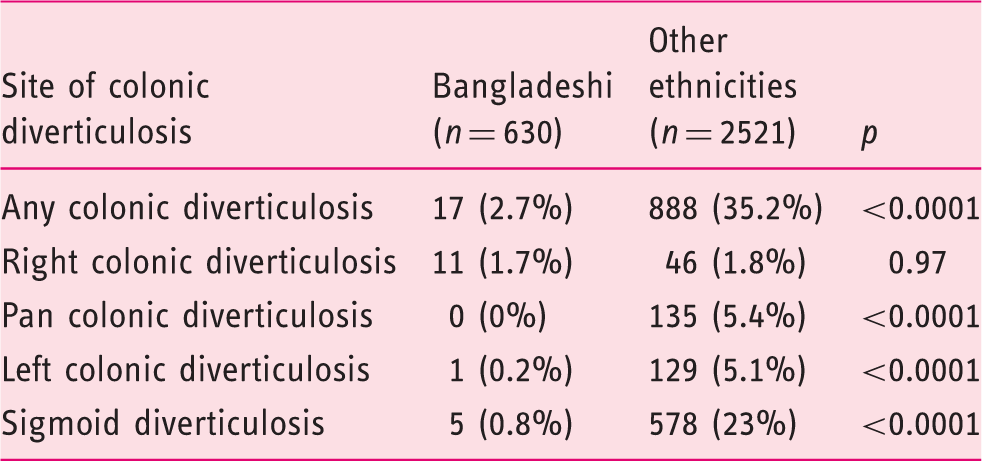
Prevalence figures for colonic diverticulosis in Bangladeshi patients versus those from other ethnicities (grouped). (Right colonic diverticulosis were diverticula recorded between the caecum and hepatic flexure; left colonic diverticulosis were diverticula between the splenic flexure and sigmoid, pan colonic diverticulosis were diverticula present throughout the colon.)
The age-related prevalence of colonic diverticulosis by ethnicity. Patients with unknown ethnicity were not included in this table
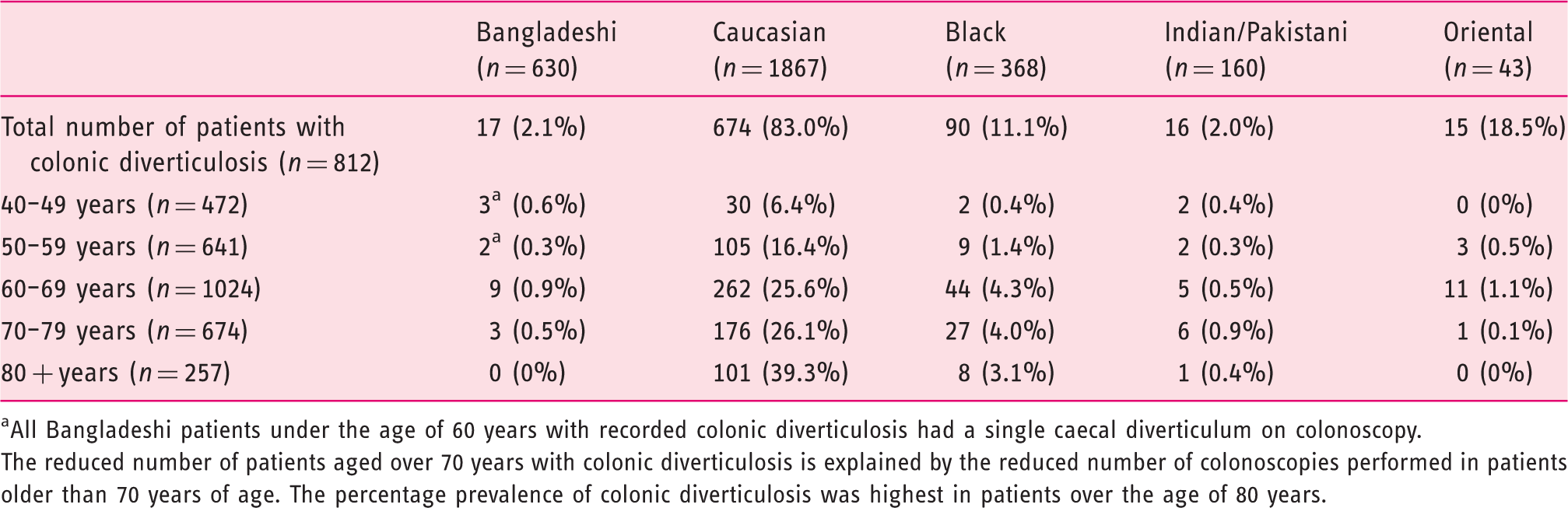
All Bangladeshi patients under the age of 60 years with recorded colonic diverticulosis had a single caecal diverticulum on colonoscopy.
The reduced number of patients aged over 70 years with colonic diverticulosis is explained by the reduced number of colonoscopies performed in patients older than 70 years of age. The percentage prevalence of colonic diverticulosis was highest in patients over the age of 80 years.
Figure 1A and B shows the prevalence of colonic diverticulosis in different ethnic groups. The overall prevalence in the Bangladeshi cohort (2.7%; 17/630) was significantly lower than in the Caucasian (674/1867; 36%), Indian/Pakistani (10%; 16/160), Oriental (34.9%; 15/43), Black (90/368; 24.4%) and the unknown ethnicity group (25.6%; 27/83) (p < 0.0001, χ
2
). Furthermore, of the 17 Bangladeshi patients with evidence of diverticula, 11 had only a solitary caecal diverticulum, leaving a prevalence of only 1.0% of classic (left-sided including sigmoid) disease compared with 28.1% in other ethnic groups combined (Table 3). The mean age of patients with multiple colonic diverticula seen on colonoscopy was 67.3 years in the Bangladeshi cohort and 67.2 years in the combined other ethnicities cohort. This was slightly older than the mean age of both whole cohorts (61.4 years Bangladeshi vs 63.6 years other ethnicities).
(A) Numbers of patients with colonic diverticulosis by ethnicity. (B) Percentage of patients with colonic diverticulosis by ethnicity.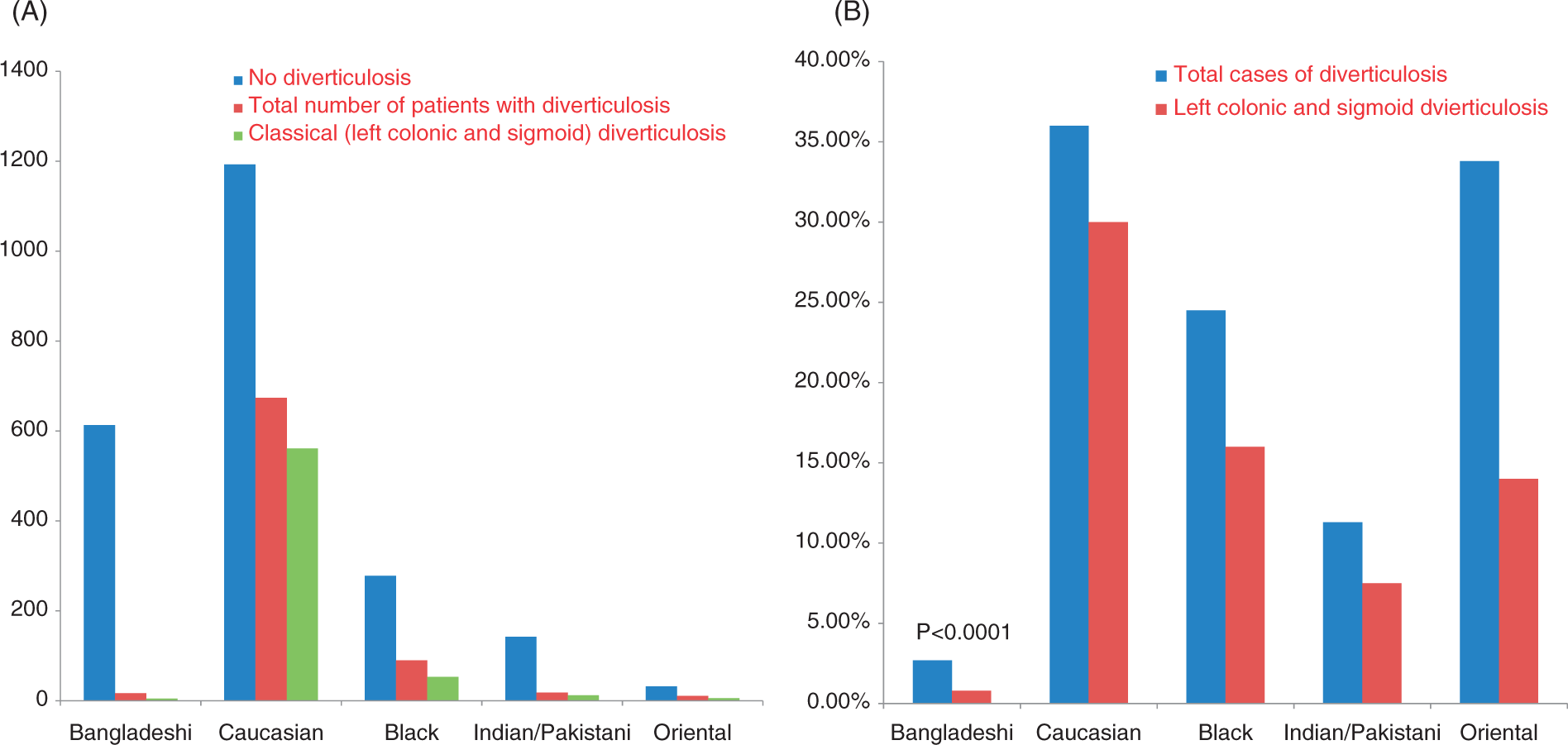
Comorbidities
Bangladeshi’s had significantly increased incidences of type 1 diabetes, type 2 diabetes and ischaemic heart disease compared with other ethnicities (Table 2). There were, however, slightly fewer obese patients in the Bangladeshi group (6.2. vs 8.7%). Significantly fewer Bangladeshis were on steroid treatment. There was no significant difference in non-steroidal anti-inflammatory drug usage.
Discussion
The prevalence of colonic diverticulosis in Bangladeshi patients in our study was very low, with only 1% having multiple classically-sited (sigmoid/left) diverticula. This prevalence was much lower than all other ethnic groups, despite being observed in a cohort of patients who were, in comparison with other ethnic groups, more comorbid for cardiovascular disease and diabetes. Furthermore, some indications for colonoscopy that might predict eventual findings of diverticulosis were actually more frequent in the Bangladeshi group, for example abdominal pain, diarrhoea and constipation (vs surveillance, rectal bleeding, positive faecal occult blood test). The small, but significant, differences in steroid usage (greater in other ethnicities) could, conceivably, have influenced the incidence of rectal bleeding in this group, but is unlikely to have influenced prevalence of diverticulosis based on previous literature. 23
While the observed influence of Bangladeshi ethnicity on prevalence of diverticulosis appears dramatic, the study has limitations that must be discussed. All retrospective studies are limited by bias. First, it is possible that selection bias might have led to a predilection for colonoscopy, i.e. screening uptake in a group of Bangladeshis who had better general health and diet. Bangladeshis within the Tower Hamlets borough of London are known to be among the poorest populations in the city (and, indeed, the UK). However, while cultural differences, along with low socioeconomic status (SES), might have led to poor uptake of health services in the most at-risk group, we have no evidence to support this contention. In fact, the prevalence of diverticulosis would be supposed high in all Bangladeshis if the previously acknowledged influence of low SES 24 was applied. Second, it is possible that ascertainment bias led to reduced reporting of colonic diverticulosis in the Bangladeshi group. Colonoscopy has not been historically used to determine background prevalence of diverticulosis, with previous estimates being based mainly on barium enema and autopsy studies. More recent population studies have largely drawn inference from incidence of complications.3–5 However, the results we obtained in Caucasians correspond to publications of prevalence from unselected colonoscopic examinations in large cohorts,19–21 as well as several historic barium enema25,26 and autopsy studies.27,28 Furthermore, regardless of the argued reduced sensitivity for colonoscopy in detecting colonic diverticulosis compared to other methods, the data in the current study are comparative, i.e. reduced endoscopic sensitivity should influence yield in all groups equally and not, therefore, affect the central hypothesis. The only proviso to this is that despite a high level of quality control engendered by national and local training using Endoscribe, it could still have been possible that experienced local endoscopists, cognisant of the low prevalence of diverticulosis in Bangladeshis had either stopped looking for it or reporting it in this patient group. However, on questioning senior endoscopists, we have no reason to suspect that this is practised. Furthermore, we confirmed in a random sample of 200 patients that the reporting of colonic diverticulosis was sufficiently clear so as not to have been biased by the investigators in the knowledge of ethnicity (no interobserver variability). While other confounders might include the Bangladeshi cohort being significantly younger than other grouped ethnicities given that incidence of colonic diverticulosis increases with age, the difference in age noted (2 years), while significant given the cohort size, was unlikely to have conferred anything more than a small difference in disease progression. The same is true of the very small difference in obesity levels (6% vs 8%) noting also that UK 4 and international3,29,30 cohort studies of DD and obesity have principally observed changes in the risk and outcome of complications of DD (inflammation, perforation and bleeding), rather than overall prevalence.
Accepting these limitations, the very low prevalence of colonic diverticulosis in Bangladeshis is a magnitude lower even than other ethnic communities, such as those from other Asian areas. The finding that the Indian/Pakistani group had a significantly lower prevalence of diverticula than Caucasians is in agreement to a previous study, which found a significant difference between subcontinental Asians and British Caucasians. 14 However, the 10-fold difference in prevalence of multiple diverticula between Bangladeshi’s and other subcontinental Asians is still highly significant. Sixty-five percent (11/17) of diverticula found in Bangladeshi patients were in the right colon, of which 10 of 11 only had a single caecal diverticulum. The predilection of diverticula in the right colon in Asians and sub-Saharan Africans has been documented previously. 9 The presence of a solitary diverticulum in the caecum may be congenital and not a pathological finding. In a previous study, 42% of Singaporean patients with right colonic DD had a single caecal diverticulum. 31
Since Painter and Burkitt’s seminal epidemiological hypothesis in 1971, 9 the concept of DD as a ‘disease of Western civilisation’ concomitant on the consumption of increased refined sugar 9 and decreased dietary fibre has held primacy with supporting evidence from changing incidences in mobile populations, for example Japanese Hawaiians 11 and African Americans, 12 decreased incidence in vegetarians, 32 increased incidences in low SES populations with poor diet,21,33 and small case control and cohort studies.34,35 In contrast, the current study has presented data from a migrant population that seems almost resistant to the development of colonic diverticulosis despite low SES and high incidences of other Western conditions, such as atherosclerosis and type 2 diabetes. Although the latter findings in no way prove that the Bangladeshi community eats a diet that should promote development of diverticulosis, detailed prospective dietary data not presented in the current study, but obtained by a separate study of Tower Hamlets Bangladeshis at our institution as part of the diabetes prevention program (BanglaDiP), confirm the supposition that migrated Bangladeshis have a diet that is high in sugar (owing to traditional Bangladeshi sweet intake) and low in fibre (large volume of white rice consumed). Regrettably, the current study did not explore risk (diet) or exposure times, as detailed dietary and migratory data were not recorded. Nevertheless, the scale of disparity between Bangladeshis and all other ethnic groups in terms of colonic diverticulosis prevalence must suggest that ‘Western civilisation’ alone is unlikely to be the only determinant of colonic diverticulosis development. This thesis is entirely in agreement with data from a recent cross-sectional study from the USA (also using colonoscopy) in which longitudinal dietary data were collected, and in which quality of diet had no apparent effect on risk. 20 Future studies could confirm the findings of the current study with more detailed prospective recording of migratory and dietary factors. Such studies could also pave the way for genomic approaches to identify differences between high and low incidence populations that may yield preventative targets for this important, yet under-researched, disease.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
All authors have completed the Unified Competing Interest form at ![]() (available on request from the corresponding author) and declare no support from institution for the submitted work; no relationships with any institution that might have an interest in the submitted work in the previous three years; and no non-financial interests that may be relevant to the submitted work.
(available on request from the corresponding author) and declare no support from institution for the submitted work; no relationships with any institution that might have an interest in the submitted work in the previous three years; and no non-financial interests that may be relevant to the submitted work.