
Abstract
We present a 63-year-old male with a history of chronic cystoprostatitis and urethral stricture with recurrent purpuric skin lesions and fulminant uroseptic shock. Initial treatment for suspected septic vasculitis with antibiotics and corticosteroids improved his condition, but vasculitis recurred after corticosteroid tapering. Repeated biopsies confirmed leukocytoclastic vasculitis (LCV) triggered by persistent prostate infection. To our knowledge, this is the first reported case of recurrent LCV triggered by chronic cystoprostatitis—a rare and underrecognized infectious etiology. Definitive resolution required addressing the underlying prostatitis, underscoring the importance of identifying and treating chronic infectious triggers in recurrent cutaneous vasculitis.
Keywords
Introduction
Leukocytoclastic vasculitis (LCV) is a small-vessel vasculitis characterized histologically by neutrophilic infiltration of post-capillary venules with leukocytoclasia and fibrinoid necrosis, and clinically by palpable purpura.1–3 The etiologies of this type of vasculitis are diverse and include infections, drugs, autoimmune diseases, inflammatory bowel disease, and malignancy.4–6 Infections—such as those caused by Staphylococcus aureus, Streptococcus, hepatitis B and C viruses, and HIV—remain among the most frequent identifiable triggers. 7 Drug-induced cases are well described with antibiotics (β-lactams, fluoroquinolones), diuretics, antihypertensives, and biologics. 8 Paraneoplastic vasculitis represents another potential mechanism, particularly in hematologic and solid malignancies. 5 Despite these associations, approximately 40%–50 % of cases remain idiopathic. 3 Direct immunofluorescence (DIF) from an early lesion (<24 h) improves diagnostic yield and may help with classification.
In this case, we describe the diagnostic challenges and clinical course of a patient with fulminant uroseptic shock and recurrent LCV skin lesions. It further highlights the diagnostic importance of repeat biopsy with DIF, helping to differentiate between septic vasculitis and LCV triggered by a chronic infection with a presence of vasculopathic changes in association with a heterozygous Factor V Leiden mutation. By illustrating the interplay between infection and thrombophilic predisposition, this report adds to the literature emphasizing the need to identify and treat chronic infectious sources in recurrent vasculitis.
Case report
A 63-year-old male presented with an asymptomatic maculopapular rash and a non-palpable purpura on the extremities, that was present for 4 days (Figure 1). He had an indwelling urinary catheter because of prostatic obstruction, which was replaced 10 days prior. The patient had a history of recurrent cystoprostatitis and penile stricture. He reported experiencing several episodes of a similar rash on his hands and feet for the past 4 years, which was treated by his general practitioner with systemic prednisolone over several days, resulting in complete resolution of the skin lesions.

Maculopapular rash and purpural lesions on the right hand on the first hospital day.
Ultrasonography and computed tomography revealed a residual bladder hematoma as the sepsis focus, resolving with irrigation, but with a significant bladder wall infection. The patient had elevated C-reactive protein and leukocyte counts, as well as thrombocytopenia, without signs of disseminated intravascular coagulation (DIC). His condition deteriorated, and he was transferred to the intensive care unit with fulminant uroseptic shock.
Urine cultures were positive for Staphylococcus aureus. Histopathology of petechial skin lesions showed severe vascular damage with fibrin thrombi and erythrocyte extravasation but no immune complex deposition in the DIF test. No bacteria were found in the biopsy. There were no relevant drug reactions that could have induced the vasculitis. The extensive serologies for complement factors were normal. Cefepime and clindamycin were initially administered for 5 days because of suspected toxic shock syndrome. The initial empirical antibiotic treatment was adjusted to co-trimoxazole for 7 days and corticosteroids, assuming bacterial sepsis with septic vasculitis. Eventually, the therapy resulted in complete recovery. The patient reported relief following antibiotic and corticosteroid therapy and expressed appreciation for the thorough diagnostic process that identified the underlying infection as the trigger of his vasculitis.
Two months later, the patient returned with another episode of recurrent purpuric lesions and new-onset livedo reticularis after tapering the prednisolone dosage to 5 mg. A new skin biopsy of the left thigh showed neutrophilic infiltration and fibrin-thrombi in capillaries (Figure 2(a)). IgM and C3 deposits were detected in the walls of small dermal vessels by DIF (Figure 2(b)) and the diagnosis of LCV was established. The biopsy of the right knee showed thrombosed vessels as well as vasculitic changes extending from the entire dermis into the upper subcutaneous fat tissue. Thus, features of both vasculopathy and LCV were present. Given the evidence of vasculopathic changes, the patient underwent a hematologic work-up for thrombophilia that revealed a heterozygous Factor V Leiden mutation.
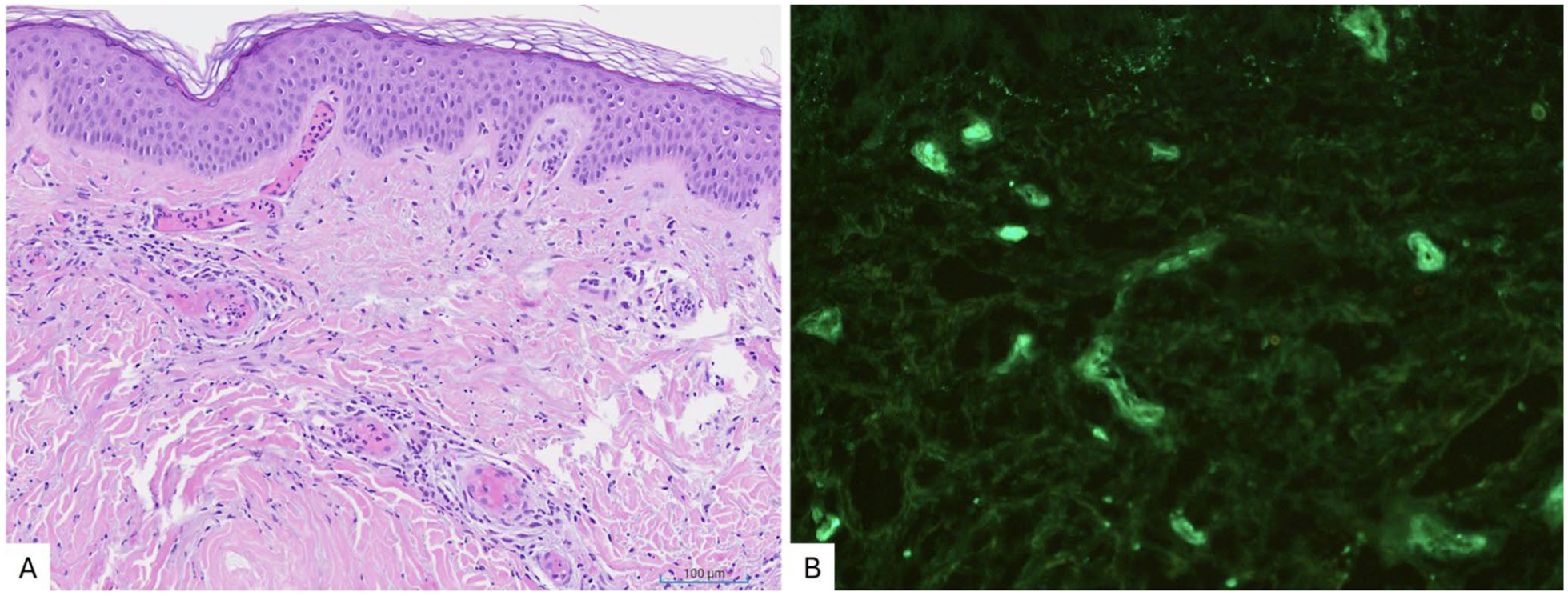
Histology of a purpuric lesion on the right lower leg: H&E stain (a). Small vessel vasculitis with infiltration of vessel walls with neutrophils, fibrinoid necrosis of vessel walls and intravascular thrombi. Perivascular infiltrate mainly of neutrophils with leukocytoclasia and nuclear dust (=degeneration of leukocytes), and discrete extravasation of red blood cells.
In summary, systemic vasculitis was unlikely and we therefore concluded that the chronic cystoprostatitis was triggering the vasculitis symptoms. A minimally invasive prostatectomy, including urethral reconstruction, was planned. However, the patient chose to delay the surgery, and the vasculitis recurred. The patient adhered to the prescribed corticosteroid taper and antibiotic therapy during the initial episode, with good tolerability and no reported adverse effects. However, the planned surgical intervention (prostatectomy and urethral reconstruction) was delayed at the patient’s request, contributing to recurrence. No medication side effects or intolerances were noted.
Discussion
As the patient initially presented with septic shock, treatment for toxic shock syndrome was started, a diagnosis with poor prognosis, also considering the possibility of an allergic reaction or urticarial vasculitis. Histopathology later revealed features consistent with septic vasculitis. Accordingly, we treated the septic condition with antibiotic therapy and corticosteroid support.
We initially suspected septic vasculitis in the context of the patient’s urosepsis, and the clinical improvement following antibiotic therapy initially supported this hypothesis. However, several factors made septic vasculitis unlikely as the final diagnosis: the patient quickly improved after starting antibiotics, which is quite untypical for septic vasculitis, which usually presents with more extensive systemic and cutaneous involvement.9,10 Blood cultures remained negative throughout and there were no bacteria found in the skin biopsy. Consequently, antibiotics were discontinued after approximately 10 days, shorter than typical durations for septic vasculitis treatment. The patient was discharged on a tapering dose of prednisolone. After 2 months, the vasculitic skin lesions recurred, and the second biopsy was crucial for establishing the correct diagnosis. An important step in establishing the diagnosis was the use of DIF, which significantly enhances the diagnostic accuracy of LCV by identifying immune complex deposits—particularly IgA, IgM, C3, or fibrin—in small vessel walls. DIF is most effective when performed on early lesions (<24–48 h) and serves as a crucial complement to routine histopathology in the evaluation and classification of vasculitic skin disorders. 11
Infections remain a major precipitating factor, particularly chronic bacterial infections such as Staphylococcus aureus. 12 In our case, recurrent cystoprostatitis provided a persistent antigenic stimulus, driving immune complex deposition and small-vessel inflammation. In other cases, LCV can mimic other dermatologic or infectious conditions, leading to diagnostic delays. Buck et al. (BMC Gastroenterology, 2020) reported a patient with Crohn’s disease whose leukocystoclastic vasculitis lesions were initially misdiagnosed as cellulitis, highlighting that both conditions can present with erythematous, tender plaques. 4 Such overlap underscores the importance of histopathologic confirmation, especially when infection or inflammatory bowel disease is suspected.
Drug-induced LCV continues to be reported with modern therapeutics, including methotrexate, biologics, and immune checkpoint inhibitors.8,13 Paraneoplastic vasculitis has also been described, particularly with hematologic malignancies and solid tumors. 5 Moreover, LCV associated with COVID-19 infection or vaccination has emerged as a recent clinical entity. 14
In our patient, the chronic infectious focus (cystoprostatitis) likely acted as a trigger for recurrent immune complex–mediated vasculitis. The presence of Factor V Leiden may have contributed to the observed vasculopathic features; its contribution in this clinical context remains speculative. 14 Although the second biopsy demonstrated fibrin thrombi in small dermal vessels alongside findings consistent with LCV, these changes result from immune complex-mediated inflammation rather than a primary thrombotic vasculopathy. The patient’s septic condition may have served as an additional transient thrombotic risk factor, but no direct causal link to Factor V Leiden could be established in this case.
This case report has several strengths. First, it presents a rare and likely first-described instance of recurrent LCV secondary to chronic cystoprostatitis, contributing novel clinical insight to the literature. The diagnostic process is thoroughly documented, including the use of repeat histopathology and DIF, which strengthens the diagnostic reliability. Additionally, the report highlights the diagnostic value of identifying infectious triggers in recurrent vasculitis.
However, limitations must also be acknowledged. As a single case report, generalizability is inherently limited. The lack of histopathologic sampling from the prostate prevents direct confirmation of the infection as the definitive antigenic trigger. Moreover, while the patient had a Factor V Leiden mutation, the association between thrombophilia and LCV in this context remains speculative and cannot be conclusively established. Finally, the delay in surgical intervention limited the ability to assess whether removal of the infectious focus would result in long-term remission of vasculitis.
Conclusion
LCV is a small-vessel vasculitis characterized by the inflammation of small blood vessels, particularly post-capillary venules, due to immune complex deposition. Differentiating LCV from other types of vasculitis can be challenging due to its heterogeneous clinical presentation. Key messages in diagnosis include the time lapse between clinical presentation and biopsy, as well as the use of DIF from a fresh skin lesion (desirably <24 h duration). This case underscores the importance of early identification of the underlying etiology in vasculitis. Timely recognition and targeted treatment of the infectious trigger are essential to prevent recurrence and potential systemic complications. It underscores the need for comprehensive immunological, infectious, and hematologic evaluations in patients with atypical vasculitic presentations. Sometimes a second biopsy is needed, and the DIF test can be an important additional diagnostic tool for identifying immune complex deposition in small-vessel vasculitis.
Supplemental Material
sj-docx-1-sco-10.1177_2050313X261420032 – Supplemental material for Case report: Challenging diagnosis of leukocytoclastic vasculitis, caused by recurrent urinary tract infection
Supplemental material, sj-docx-1-sco-10.1177_2050313X261420032 for Case report: Challenging diagnosis of leukocytoclastic vasculitis, caused by recurrent urinary tract infection by Slavena Dineva, Christoph Henzen, Thomas Hodel, Gernot Schmid, Emel Türkay, Sacha Zeerleder, Claudia Vonlanthen and Isabel Kolm in SAGE Open Medical Case Reports
Footnotes
Author note
All patient identifiers have been removed from the case report. No names, initials, dates of birth, or other identifying details are included. The patient is referred to only by age and gender, and clinical details are presented in a way that ensures anonymity.
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.