
Abstract
A 67-year-old Japanese man had been complaining of discomfort in the chest and back and feeling febrile for 2 weeks. Chest computed tomography indicated a thoracic aortic aneurysm. He occasionally showed a high fever (up to 38.0°C), even after hospital admission, irrespective of antibiotic therapy. The patient was found to have elevated serum IgG4 levels (366 mg/dL). The aneurysm demonstrated rapid growth; therefore, rifampicin-soaked woven Dacron synthetic graft replacement was performed 22 days after admission. Immunohistostatining of the resected aorta segment showed an IgG4-positive plasma cell infiltrate within the intimal layer neighboring the cholesterol-rich atheromatous plaque. After surgery, the patient’s serum IgG4 level dropped acutely; however, it did not reach the normal range. The possible role of IgG4 in the development or suppression of aortic remodeling, as well as in atherogenesis, among patients with rapidly growing aortic aneurysm requires further investigation.
Introduction
Immunoglobulin G4 (IgG4)-related disease, 1 which is characterized as inflammatory cell infiltration with IgG4-positive plasma cells, dense fibrosclerosis, and elevated serum IgG4 levels, 2 has been gathering increasing attention owing to its possible involvement of a wide variety of organs, including lung, kidney, liver, and exocrine and endocrine organs. Inflammatory aortic aneurysm, although not all of them, are now considered to represent one of the features of IgG4-related disease. 3
Several reports showed that infiltration of IgG4-positive cell in the perivascular tissue may occur in chronic infected aortic aneurysm 4 or infected aortitis, 5 suggesting that IgG4-positive cell might have physiological importance during the development of aortic aneurysm. IgG4, unlike other immunoglobulin G subclasses, cannot activate complement and is involved in a continuous process of half-molecules referred to as Fab-arm exchange, 6 and therefore, whether IgG4 aggravates or counteracts the aortic inflammation or whether it is a bystander, awaits further investigation. Here, we report the case of a patient with thoracic aortic aneurysm in whom elevation of serum IgG4 levels and infiltration of IgG4-positive plasma cell in intimal layer were demonstrated.
Case report
A 67-year-old Japanese man had been complaining of discomfort in the chest and back, and feeling febrile for the previous 2 weeks. He did not have a past history of autoimmune pancreatitis or diabetes mellitus. He underwent chest computed tomography (CT) that showed aortic aneurysm that was located in the distal aortic arch and was referred to our hospital. His medical history was unremarkable from the cardiovascular point of view. On admission, vital signs showed a body temperature of 36.2°C, blood pressure of 126/68 mmHg, and heart rate of 58 beats/min. Chest X-ray revealed a cardiothoracic ratio of 54%. Laboratory studies showed a white blood cell count of 8730/µL, hemoglobin level of 15.2 g/dL, platelet count of 46.2 × 104/µL, C-reactive protein (CRP) concentration of 6.87 mg/dL, soluble interleukin 2 receptor level of 169 U/mL, and serum procalcitonin level of 0.06 ng/mL. The patient tested negative for antinuclear antigen. His serum levels of IgG, IgA, and IgM were 1567, 67, and 50 mg/dL, respectively, and his serum IgG4 level was increased to 366 mg/dL. Antibiotic (meropenem hydrate) administration was started under the suspicion of the active infection at the aortic wall or periaortic tissue, although the blood culture was negative. Because his CRP levels did not fall and his body temperature was again elevated to 38.0°C, vancomycin hydrochloride treatment was also started. CT on day 22 after admission showed enlargement of ulcer-like projection in the aortic wall (Figure 1), and the patient underwent urgent thoracic aortic replacement. It was found that the aneurysm partially lacked its wall structure, and the vascular lumen was in direct contact with lung parenchyma.

Contrast-enhanced computed tomography. Aortic aneurysm that was located in the distal aortic arch. (a and b) Images acquired on the day of admission to hospital. (a) Transverse and (b) coronal sections are shown. Thickening of the periaortic region is observed. (c and d) Images acquired 19 days after admission. (c) Transverse and (d) coronal sections are shown. The diameter of the aortic arch and the size of ulcer-like projection showed slight enlargement.
The etiology of aneurysm was suspected as pseudo-aneurysm due to severe infection. Then, via left thoracotomy, aneurysmal wall was resected and the rifampicin-soaked woven Dacron synthetic graft (26 mm Gleveave; Vescutek, Terumo, Japan) that was covering between the aortic arch 1-cm distal to the origin of the left subclavian artery and descending aorta at the level of Th6 was placed. Antibiotics were continued after the operation, and the patient was discharged 41 days after surgery with peroral antibiotics.
Infective microorganisms were not apparent in the histologic specimen obtained at the time of surgery, and IgG4 staining showed IgG4-positive plasma cell infiltrates neighboring the atheromatous plaque within the intimal layer (Figure 2). The serum IgG4 level remained high, but showed an acute drop after the operation (Figure 3), although it did not reach the normal range, which is less than 105 mg/dL. The patient is now followed as outpatient, without recurrence of graft infection and is treated with oral minocycline.

Histological and immunohistochemical findings of the resected aorta specimen. (a) Elastica van Gieson staining, (b) hematoxylin and eosin staining, (c and f) CD38 staining, (d and g) IgG staining, (e and h) IgG4 staining. (f, g, and h) A high-powered image of the bracketed area in (c, d, and e), respectively. Infiltration and accumulation of the lymphocytic cells are observed (arrows) at the shoulder of the plaque containing cholesterin crystals (arrowheads). Original magnifications, ×40 (a–e) and ×100 (f, g, and h). Scale bar indicates 200 µm.
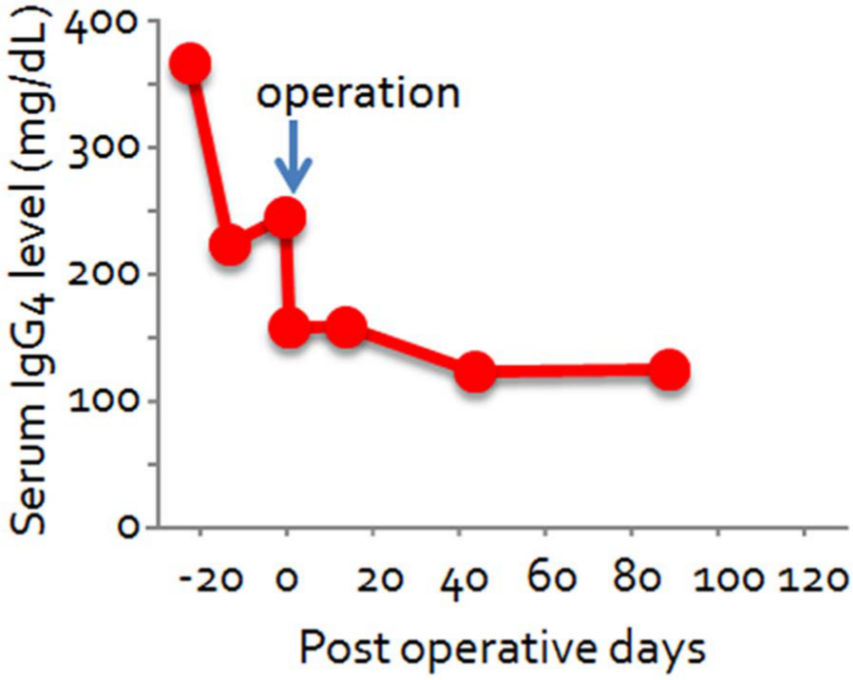
Trend in serum IgG4 levels.
Discussion
We herein report a patient with the diagnosis of aortic aneurysm who showed elevated serum levels of IgG4 and an IgG4-positive cell infiltrate in a specimen from the resected aorta. Due to enlargement of the aneurysm, synthetic graft replacement was performed before complete resolution of the elevation of the inflammatory markers. After the surgery, serum IgG4 level dropped acutely; however, it did not reach normal values. Infected aortic aneurysm, which is infrequently life-threatening without timely surgical therapy, is a distinct entity of inflammatory aortic aneurysm, a disorder that is histologically characterized by extensive fibrosis with marked thickening of the aortic wall and severe lymphoplasmacytic infiltration.3,7 Because an immunological background is presumed to underlie inflammatory aneurysm, corticosteroid therapy may be effective in reducing the extent of inflammation, in distinguishing mantle sign, and, albeit not always, in reducing the size of the aneurysm. 8 Infected and inflammatory aneurysms may be differentially diagnosed according to clinical symptoms, their location, morphology, and susceptibility to rupture: infected aneurysms may appear saccular in shape with characteristic rapid growth and a strong tendency to rupture, 9 whereas inflammatory aneurysms are usually fusiform and located in the abdominal part of the aorta. 10 With regard to our patient, high fever and sustained elevation of CRP, in addition to the location, morphology and clinical course of the aneurysm, led us to suspect infected aortic aneurysm, but the diagnosis could not be made because of the negative bacterial culture of the aneurysmal sac, as well as blood samples, which might, however, have been due to the prolonged antibiotoic theraphy.
Because serum IgG4 concentrations were elevated, it is presumed that serum IgG4 may be a useful biomarker for discrimination between infected and inflammatory aortic aneurysm,2,11 it should be noted, however, that only about a half of the cases of inflammatory aortic aneurysm may possess features of IgG4-related disease. 3 Conversely, an IgG4-positive cell infiltrate may be observed in the infected aortic aneurysm, especially if it is a chronic form. 4 We could not make diagnosis of infected aortic aneurysm because of the negative results of the bacterial cultures. It was reported that only about a half of the patients with infected aortic aneurysm may have positive blood cultures. 12 Because of the fever and increased inflammatory markers, the patient was presumed to have active infection or inflammation at the site of thoracic aorta, although the blood culture was negative. We used rifampicin-soaked woven Dacron synthetic graft because it had been shown to be safe, durable, and resistant against infection in the case of in situ repair of infected aortic aneurysms in several previous reports.13–15
In our patient, serum IgG4 levels fell rapidly after surgical intervention. A similar phenomenon was observed in a patient with IgG4-related coronary periarteritis, 16 and it may be attributed to a decline in lymphocytic activity after extracorporeal circulation. 17
The role of IgG4 in the development (or the limitation) of the aortic wall injury observed in inflammatory and infected aneurysm remains unclear; however, IgG4-positive cell infiltrates have been reported to be present in the adventitial layer. In our case, IgG4-positive plasma cells were accumulated within the intimal layer. Infiltration of the lymphocytic cells and macrophages in the shoulder region of the atheromatous plaque has been demonstrated; 18 to our knowledge, this is the first report to show the IgG4-positive plasma cell infiltration in such regions.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.