
Abstract
Although anatomical variations in pulmonary arterial branching are relatively common, the presence of an anterior truncal basal pulmonary artery is extremely rare. We herein report a unique case of right lower lobe lung cancer associated with an aberrant mediastinal A7 + 8 + 9 + 10(b + c) artery, successfully managed with thoracoscopic right lower lobectomy. A 76-year-old man presented with a gradually enlarging part-solid ground-glass opacity in segment 10 of the right lower lobe, clinically diagnosed as stage cT1aN0M0, stage IA1 adenocarcinoma. Contrast-enhanced imaging was not possible due to an allergy to iodinated contrast; however, high-resolution CT revealed an aberrant basal pulmonary artery that originated from the right main pulmonary artery and coursed medially into the lower lobe. Three-dimensional preoperative reconstruction was limited due to the lack of contrast enhancement. Video-assisted thoracoscopic right lower lobectomy was performed after wedge resection confirmed malignancy. Pathological staging was pT1aN0M0, stage IA1. The patient had an uneventful postoperative course and remains recurrence-free at 1 year. This case highlights the importance of detailed preoperative imaging review, particularly when contrast-enhanced computed tomography is contraindicated. A careful assessment of High-resolution computed tomography in multiple planes and an awareness of radiographic signs are essential for detecting rare vascular anomalies and ensuring safe surgical outcomes.
Keywords
Introduction
The branching patterns of the pulmonary arteries exhibit considerable anatomical variation among individuals, necessitating careful preoperative assessment to ensure surgical safety. High-resolution computed tomography (HRCT) and three-dimensional computed tomography (3D-CT) are valuable modalities for visualizing vascular anatomy prior to pulmonary resection. Although variations in pulmonary arterial branching are relatively common, the presence of a right anterior truncal basal pulmonary artery is exceptionally rare, with only a limited number of cases reported in the literature. We herein report a rare case of right lower lobe lung cancer associated with an anterior truncal basal pulmonary artery, successfully managed with right lower lobectomy following detailed preoperative imaging and anato-mical confirmation.
Case
A 76-year-old male was referred to our hospital for further evaluation after an abnormal shadow was detected on chest radiography. Although no overt tumor was visible, the right main pulmonary artery was not delineated below the level of the second right bronchial bifurcation (Figure 1). Chest CT revealed a part-solid ground-glass opacity in segment 10 (S10) of the right lower lobe, measuring 18 mm in total diameter with an 8 mm solid component (Figure 2). The lesion demonstrated slow growth over time. Additional diagnostic evaluation with 2-[¹⁸F]fluoro-2-deoxy-D-glucose positron emission tomography–CT (FDG PET-CT) and brain magnetic resonance imaging revealed no evidence of distant metastasis. Based on these findings, the lesion was clinically diagnosed as a primary lung cancer of the right lower lobe (cT1aN0M0, stage IA1). Contrast-enhanced CT was contraindicated due to the patient’s allergy to iodinated contrast media. Nevertheless, HRCT revealed an aberrant right anterior truncal basal pulmonary artery (A7 + 8 + 9 + 10[b + c]) arising from the right main pulmonary artery. This vessel coursed posterior to the upper pulmonary vein and medial to the middle lobe bronchus before entering the lower lobe (Figure 3). Reconstruction with 3D-CT based on non-contrast CT data failed to provide adequate visualization of this anomalous artery.

Chest radiography showed no tumors.

Chest CT showed a part-solid ground-glass opacity in segment 10 (S10) of the right lower lobe, measuring 18 mm in total diameter with an 8 mm solid component.

Anterior truncal basal pulmonary artery A7 + 8 + 9 + 10(b + c) (yellow arrow) branched from the central side of the superior trunk artery (red arrow), and flowed into the basal segment from the dorsal side of the superior pulmonary vein (blue arrow), passing through the middle and lower lobe bronchi.
The patient underwent five-port video-assisted thoracoscopic surgery. Initially, wedge resection was performed, and intraoperative frozen section confirmed lung adenocarcinoma. As the tumor received blood supply from both mediastinal and interlobar pulmonary arteries, limited resection, such as basal segmentectomy, was deemed inappropriate. Therefore, a right lower lobectomy was performed.
The interlobar fissure between the middle and lower lobes was well developed. The segmental arteries A6 and A10a were identified as branches of the interlobar pulmonary artery (Figure 4(a)). The right lower lobe bronchus and inferior pulmonary vein were divided (Figure 4(b)), followed by division of the aberrant A7 + 8 + 9 + 10(b + c) using an endoscopic stapler (Figure 4(c)). Systematic mediastinal lymph node dissection was performed. The operation lasted 157 min, with a total blood loss of 60 mL. The postoperative course was uneventful. The chest drain was removed on postoperative day 5, and the patient was discharged on day 7. The final pathological diagnosis was adenocarcinoma, measuring 13 mm in total diameter with 10 mm solid component; no lymph node metastases were observed, pT1aN0M0, stage IA1. At the one-year follow-up, the patient remains disease-free.
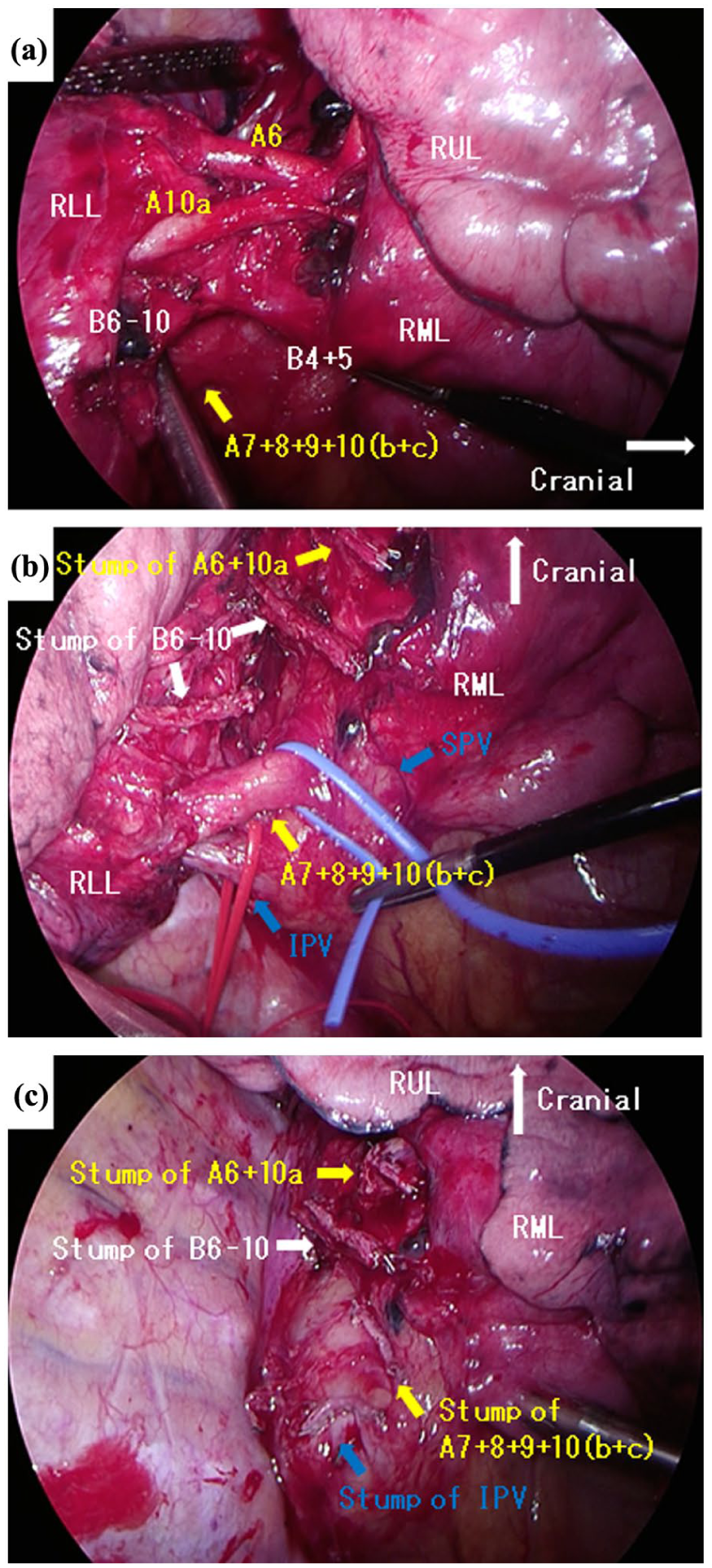
Intraoperative findings. (a) A6 + 10a was identified as branching from the interlobar pulmonary artery. (b) After dissection of A6 + A10a, B6 − 10. (c) After dissection of A7 + 8 + 9 + 10(b + c).
Discussion
Pulmonary arterial branching patterns vary widely among individuals, and preoperative recognition of such anatomical variations is essential to avoid intraoperative complications, particularly vascular injury and bleeding. Among these, mediastinal lingular arteries (e.g., A4+5, A4, or A5 subtypes) are relatively common. 1 In contrast, aberrant basal segmental arteries originating from the mediastinum are exceedingly rare, with a reported incidence of just 0.03%. 2 To date, only 14 cases of right anterior truncal basal pulmonary arteries have been documented.3–5 This is the first reported case of a mediastinal A7 + 8 + 9 + 10(b + c) branching pattern.
Three-dimensional CT is a valuable modality for identifying such vascular anomalies preoperatively. However, contrast-enhanced imaging may not be feasible in patients with contraindications such as renal dysfunction, asthma, or contrast media allergy. In our case, only non-contrast CT was available due to contrast allergy. Although recent advancements allow 3D reconstruction from non-contrast images, the close proximity of mediastinal basal arteries to pulmonary veins can hinder accurate identification. Therefore, surgeons must carefully review axial, coronal and sagittal CT images and not rely solely on 3D reconstructions.
While chest radiography is not definitive for vascular evaluation, it can serve as a useful, cost-effective screening tool for raising suspicion of vascular anomalies. In our case, the absence of the right main pulmonary artery on radiography below the second bronchial bifurcation raised suspicion of a possible anomaly. Recognition of this aberrant vessel on both radiography and HRCT contributed to safe and complication-free surgery. An anterior truncal basal pulmonary artery typically originates from the right main pulmonary artery, passes posterior to the superior pulmonary vein, and courses between the middle and lower lobe bronchi to enter the lower lobe. In cases where the major fissure is incomplete or poorly developed, fissure dissection can increase the risk of arterial injury and bleeding.
Conclusion
Anterior truncal basal pulmonary arteries are extremely rare anatomical variants. Preoperative identification of such anomalies is crucial for preventing intraoperative complications. Although 3D-CT is a valuable tool for anatomical assessment, it may be insufficient or unavailable in certain situations, especially when contrast cannot be used. Careful interpretation of HRCT, complemented by chest radiography when appropriate, remains essential for accurate identification of vascular anomalies and for safe surgical planning.
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
This research has received approval from the Saitama Medical Center Ethics Review Committee for Clinical Research on 28/11/2024, with approval number S24-087.
Consent to participate
Informed consent was obtained verbal.
Author contributions
Kentaro Minegishi gave final approval of the version to be published. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The case report and publication process were explained to the patient, and she granted permission to publish this report.