
Abstract
Colonic perforation is prevalent in instances of abdominal trauma and is typically associated with anterior abdominal wall injury. Early diagnosis and prompt surgical intervention are essential to enhance patient outcomes. Delayed recognition of colonic perforation can result in severe complications, including peritonitis and sepsis. Diagnostic imaging, such as computed tomography, plays a critical role in determining the extent of injury and informing treatment decisions. This case report presents an instance in which a 16-year-old boy was grasped from behind and rotated laterally on both sides, resulting in multiple colonic perforations without any external abdominal injury. The child’s life was saved by promptly performing surgery to repair the intestinal perforation and subsequently administering peritoneal wash. The boy remained under observation until his discharge from the hospital and attended all routine follow-up appointments. The young adolescent is now living a healthy and normal life. The presence of traumatic colon perforation without any visible external injury to the anterior abdominal wall makes this case unusual.
Introduction
Traumatic colonic perforation is a critical and potentially life-threatening condition that requires immediate diagnosis and intervention. It may result from either blunt or penetrating abdominal trauma, with blunt trauma being the most prevlent. 1 Diagnosing colonic perforation can be complex, as the clinical manifestations range from mild abdominal discomfort to peritonitis accompanied by sepsis. 2 In cases of vehicular accidents, seatbelts are highly effective in reducing mortality and morbidity, but they may also lead to specific injury patterns, including abdominal trauma. Seatbelt-induced colonic perforation is a recognized complication associated with motor vehicle accidents, particularly among restrained passengers.3,4 Here, we present a case of transverse colon perforation resulting from abdominal trauma, where the patient was grasped by both upper limbs from behind like a lap-strap of a seat belt and shaken laterally on both sides. The initial diagnosis was made using computed tomography (CT)-guided abdominal ultrasound, which was then followed by urgent surgical treatment. Because of this quick surgical intervention, intra-abdominal contamination caused by bleeding or perforation was successfully controlled. Therefore, these injuries should not be underestimated. Here, we discuss a case of anterior abdominal wall compression without visible external injuries, yet with noteworthy intestinal findings.
Case report
A 16-year-old boy was admitted to the emergency department of our tertiary care hospital with severe abdominal pain and experiencing two to three episodes of vomiting that were non-bilious, non-projectile, and free of blood. According to the account, while playing with a friend at the playground, one of his friends grabbed him from behind at the abdominal level and forcefully swung him sideways. He began to experience severe abdominal pain and two to three episodes of vomiting within 30 min of this incident. Upon examination of the patient, the abdomen was distended, with the umbilicus inverted and positioned at the midline. No external injuries were observed on the body. Palpation confirmed abdominal distension, and generalized tenderness was noted throughout the abdomen. Rigidity and guarding were present, although no rebound tenderness, palpable organomegaly, or masses were observed. Hernial orifices and external genitalia appeared normal. A resonant note was present over the abdomen on percussion. No bowel sounds were heard during auscultation. The per rectal examination revealed no abnormalities. Prior to the radiological examination, a Ryle’s tube was inserted through the nose and extended into the stomach. When aspirated, fluid stained with fecal matter was observed coming out of the Ryle’s tube (Figure 1). The patient underwent X-ray chest and abdomen (erect posture), ultrasonography, and CT abdomen for further investigations. Imaging studies revealed a significant pneumoperitoneum (suggestive of intestinal perforation) and several air pockets within the mesentery. In addition, it was observed that the loops of both the large and small intestines, along with the mesentery, omentum, liver, and spleen, were compressed toward the back and midline, indicating abdominal centralization due to the presence of massive pneumoperitoneum (Figures 2–4). The patient was resuscitated with IV fluids, broad-spectrum antibiotics, and analgesics. An emergency exploratory laparotomy was performed. As a midline incision was made in the peritoneum, a hissing sound was heard when suction was applied, and abdominal distension was relieved, signifying the release of air pressure from the peritoneal cavity (Supplemental Video 1). Upon closer inspection of the intestine from the rectum to the ileocecal junction, a serosal tear was observed on the posterior surface of the transverse colon, measuring 4 × 2 cm (Figure 5). Upon further examination, two perforations were identified in the transverse colon, with dimensions of 5 × 3 and 2 × 1 cm, located 50 and 70 cm from the ileocecal junction, respectively (Figures 6 and 7). The tears and perforations were repaired using an interrupted suture technique with a Ethicon Mersilk 2-0. Peritoneal lavage was performed using warm saline, a drain was placed, and the abdomen was closed in layers. The patient was transferred to the intensive care unit for observation, and intravenous fluids were administered. After 24 h, the patient was permitted to consume small amounts of water. Bowel sounds gradually reappeared on the third day, and the oral liquid diet was subsequently increased. On the sixth day, the drain was removed, and the patient was instructed to gradually increase mobility. On the 11th postoperative day, the patient was discharged from the hospital. It was recommended that the patient consume meals that are high in protein, fiber, and potassium, in smaller portions and at more frequent intervals.

Fecal staining fluid is coming out from the Ryle’s tube.

The X-ray image shows pneumoperitoneum.

Centralization of abdominal organs due to the presence of gas.
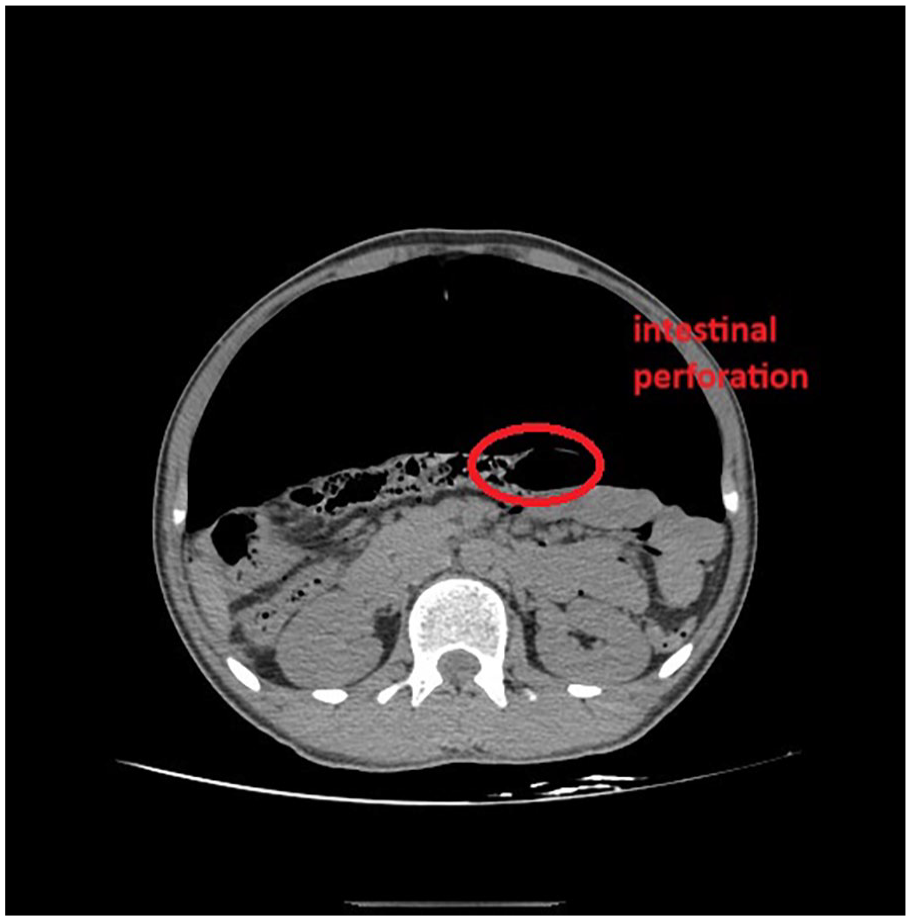
CT image of intestinal perforation.

Serosal tear of the intestine.

Transverse colon perforation.

Transverse colon perforation.
Discussion
When assessing patients with blunt abdominal trauma, particularly those injured from behind at the abdominal level, healthcare professionals should be vigilant of possible organ damage. CT is the preferred method for detecting injuries within the abdomen. In cases of blunt trauma, injuries to the abdominal organs are frequent, with the spleen and liver being the most affected. In these cases, the kidney is the third most frequently injured abdominal organ. In pediatric patients, ~25% of significant trauma cases involve abdominal injuries, with the spleen being the most frequently affected organ.5–7 Traumatic colonic perforation without external injury is a rare but serious condition that can lead to significant morbidity and mortality. According to existing literature, most colonic perforations are attributed to diverticulitis (58%) and carcinoma (21%). The overall mortality rate for colonic perforation is 19.6%, underscoring the severity of this condition. 8 Although fecal contamination increases the likelihood of early complications, it does not significantly affect the long-term outcomes if appropriately handled. Notably, fecal contamination during surgery greatly increased the risk of early postoperative complications (82.9% compared to 49.5% in cases without contamination). 9 However, it does not substantially influence the late complications or mortality rates. This indicates that effective management of early complications is essential for enhancing overall outcomes. 9 DiMaio and Molina outline three possible causes of bowel rupture: squeezing between the front abdominal wall and the spine or pelvis, sudden deceleration at a fixed point (usually the ligament of Treitz or the ileocecal junction), or a specific area experiencing heightened intraluminal pressure. He further noted that the central part of the large intestine is particularly vulnerable to injury owing to its proximity to the spine and its exposed location in the mid-abdominal region. A strong impact or compression on the front abdominal wall can crush the middle section of the transverse colon between the front abdominal wall and the lumbar vertebrae. 10 Treatment options for colonic perforation depend on factors such as the cause, location, and extent of the perforation. While surgery is frequently required, in some situations, a conservative approach may be suitable. Available surgical treatments consist of Hartmann’s procedure, segmental colectomy with anastomosis and diverting colostomy, simple oversewing of the perforation, and resection followed by primary anastomosis.11,12 Prompt action, thorough washing of the peritoneal cavity, excision of affected tissue, and assertive treatment of peritonitis are essential strategies for managing colonic perforations. 11 Compression of the anterior abdominal wall can potentially cause colonic perforation, a tear in the colon wall that leads to leakage of colon contents into the abdominal cavity, resulting in a severe infection called peritonitis. Several factors can contribute to this, including blunt trauma, surgical procedures, and even specific medical devices. 13 Similarly, in the current case, the minor was grasped from behind at the epigastric level and subjected to lateral rotation, resulting in abrupt acceleration and deceleration. This was accompanied by abdominal compression that ultimately led to colonic perforation.
Conclusion
Traumatic colonic perforation without external injury is a complex condition characterized by high morbidity and mortality rates. Early diagnosis and prompt surgical intervention are crucial for improving patient outcomes. The choice of surgical approach depends on various factors, including the location and extent of the perforation and the patient’s overall condition. Postoperative care and close monitoring are essential to prevent complications and to ensure successful recovery.
Footnotes
Ethical considerations
Ethical approval to report this case was obtained from the Institute Ethical Committee Registration—DHR Reg No.—EC/NEW/INST/2021/592 (IEC/BU/2025/Cr. 26/147/2025 dated May 9, 2025).
Consent for publication
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.
Author contributions
Soham Upadhyay—accountable for all aspects of the work and ensures that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. I drafted the work or revised it critically for important intellectual content. Riddhi Upadhyay—manuscript writing and collection of references. Arohi Gandhi—made substantial contributions to the conception or design of the work. Arijit Datta—made substantial contributions to the conception or design of the work. Akshat Vadaliya—manuscript writing and collection of references. Rushi Barot—drafted and revised the work critically for important intellectual content.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.