
Abstract
Ammonia is one of the most commonly produced chemicals in the world, with uses in agriculture, household cleaning, and as an alternative fuel source. While typically encountered in low concentrations, pure anhydrous ammonia in its gaseous form is extremely toxic and a potent caustic. We report the case of a previously healthy 19-year-old with prolonged anhydrous ammonia exposure after a motor vehicle accident caused an inadvertent release of 4000 gallons of anhydrous ammonia. Despite optimal initial medical management, he required venovenous extracorporeal membrane oxygenation (VV-ECMO) in addition to aggressive multispecialty care to address his extensive injuries. After a prolonged hospitalization, he recovered without the need for lung transplantation and returned to activities of daily living. This case highlights the fastidious care necessary to effectively treat those exposed to anhydrous ammonia, including VV-ECMO as a salvage technique.
Keywords
Introduction
In late 2023, there was a nationally reported accident on a U.S. highway involving a tanker truck carrying 7500 gallons of anhydrous ammonia that resulted in a large ammonia vapor cloud in the surrounding area. Numerous individuals died at the scene from anhydrous ammonia exposure, while others were urgently transferred to higher levels of care. 1 One of the surviving airlifted patients is the subject of this case report. They suffered severe inhalational injury secondary to anhydrous ammonia exposure and were successfully managed with venovenous extracorporeal membrane oxygenation (VV-ECMO) without the need for lung transplantation.
Case report
We report a case of a previously healthy 19-year-old male who was driving on the highway when a motor vehicle accident involving a pressurized tanker truck resulted in the release of approximately 4000 gallons of anhydrous ammonia. The patient’s estimated anhydrous ammonia exposure time was 40 min based on the timing of the initial accident. At the local hospital, he was evaluated and decontaminated to the best of their ability. A bronchoscopy was performed, demonstrating a swollen, bright red trachea without active bleeding, but tissue sloughing was already noted throughout his bilateral airways. Computed tomography (CT) of his chest without contrast and chest X-ray on arrival (Figures 1 and 2) were consistent with pneumonitis. At this time, he was transferred to our health system, a large quaternary burn referral center, and initially admitted to the Burn Intensive Care Unit.

Chest X-ray on arrival showing heterogenous opacities throughout bilateral lung fields.
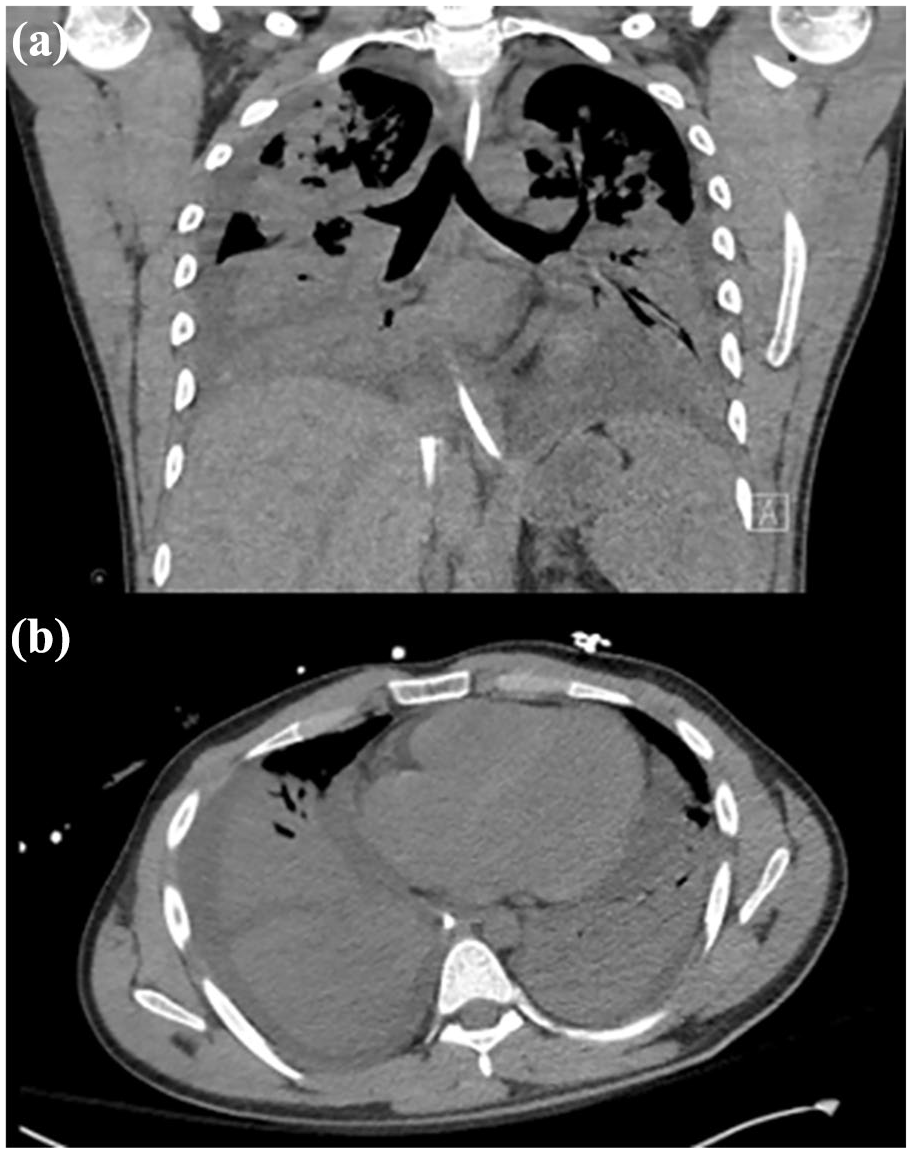
(a) Top, coronal slice of CT chest near admission, (b) bottom, axial slice of CT chest near admission, both showing extensive consolidation in lower lobes in conjunction with patchy alveolar and groundglass opacities throughout the upper lungs.
On arrival, he remained intubated on ventilator settings of volume control with tidal volume 400 mL (6.25 mL/kg of ideal body weight), FiO2 100%, respiratory rate 26, and positive end-expiratory pressure of 5 cm H2O. The patient did experience intermittent desaturations but would recover quickly. He also exhibited a normal neurological exam during sedation weans. Superficial burns were expected to heal without surgical intervention and were being managed by the Plastic Surgery service. Ophthalmology was consulted for the management of ocular exposure (Figure 3) and ordered aggressive irrigation, cyclopentolate drops, moxifloxacin drops, prednisolone drops, and erythromycin ointment. Critical Care Surgery was consulted for the ICU level of care and additionally ordered albuterol-ipratropium bromide and heparin nebulizers to help maintain airway patency. Lastly, Toxicology was consulted in the setting of anhydrous ammonia exposure and agreed with the current management, noting that care was largely supportive.

Clinical picture of ocular exam on arrival, which was consistent with toxic keratopathy secondary to anhydrous ammonia exposure.
On hospital day four, despite optimal medical management and ventilation strategies for acute respiratory distress syndrome (ARDS) (ventilator settings unchanged other than an increase in positive end-expiratory pressure to 12 cm H2O) including permissive hypercapnia, paralytic with cisatracurium, and trial of proning, the patient continued to be hypoxemic and hypercapnic with progressive worsening in lung compliance. His arterial blood gas at that time was pH 7.30, PaCO2 69, PaO2 63, and HCO3 33.7, with a SaO2 of 88%. After multidisciplinary discussions, it was decided to transfer the patient to the Cardiothoracic Surgical ICU and initiate VV-ECMO. After cannulation, his initial ECMO settings were a flow of 5.4 LPM, sweep of 8 LPM, and FdO2 100%. On hospital day six, the patient underwent an uneventful percutaneous tracheostomy with anticipation of prolonged hospitalization. Notably, early bronchoscopies showed sloughing of the airway epithelium (Figure 4). Successive bronchoscopies revealed significant mucosal casts requiring graspers to remove. Over the subsequent 5 days, the patient continued to be hypoxemic and hypercapnic despite increasing VV-ECMO settings to a flow as high as 6.5 LPM, a sweep of 11 LPM, and FdO2 continued at 100%. The ventilator was left on pressure control ventilation throughout this time period with an inspiratory pressure of 20 cm H2O, FiO2 100%, respiratory rate 10, and positive end-expiratory pressure of 10 cm H2O. During this time frame, the patient was also being considered for possible lung transplantation, which would have required transfer to another center as our institution does not perform lung transplantation. While these discussions of transfer were ongoing, and after a week on VV-ECMO (hospital day 11), his hypoxemia and hypercapnia began to slowly improve. Over the following 6 days, the ECMO settings were weaned primarily by decreasing flow and FdO2, with minimal decreases in sweep. On hospital day 18, the sweep was weaned successfully to a low of 3 LPM and subsequently 1 LPM the following day. On hospital day 19, after 2 weeks on VV-ECMO, the patient was successfully decannulated with continued improvement in compliance and gas exchange of native lungs.

Early bronchoscopy image showing sloughing of the epithelium which would go on to form bronchial casts requiring frequent bronchoscopies for removal and airway clearance.
Post-decannulation, the patient was debilitated and continued to require positive-pressure ventilation via continuous mandatory minute ventilation settings before he was eventually able to tolerate open-ended pressure support 2 weeks later (hospital day 33). Otolaryngology (ENT) was consulted after abnormal findings were noted during fiberoptic evaluation of the patient’s swallowing (hospital day 37). Upon further examination, the patient was noted to have his epiglottis tethered to the pharyngeal wall. These epiglottic adhesions are thought to be the result of extensive mucosal damage secondary to anhydrous ammonia inhalation and exposure. On hospital day 40, the patient underwent a supraglottoplasty procedure with ENT in which there was successful excision of multiple supraglottic adhesions utilizing a carbon dioxide laser (Figure 5).

Top left: tethered epiglottis shown at the beginning of laryngoscopy with ENT, others: images during and after carbon dioxide laser procedure which freed the epiglottis and allowed resumption of normal physiologic function.
Regarding his vision, there was concern that the patient would have permanent vision loss due to toxic keratopathy and the extensive epithelial defects present on an initial exam (Figure 6). Our Ophthalmology colleagues followed the patient extremely closely throughout his hospital course and, in addition to the aforementioned recommendations, also placed Prokera lenses bilaterally that stayed in place for 23 days post-admission. Prokera lenses are cryopreserved amniotic membrane that supports the corneal healing process. 2 Ultimately, he had a near complete recovery of his vision with final visual acuities of OD 20/20 (baseline 20/20) and OS 20/30 (baseline 20/25).

Clinical image showing fluorescein staining under cobalt blue light with extensive ocular epithelial damage on left (a) and right eye (b), respectively.
A repeat laryngoscopy was performed by ENT on hospital day 44, which showed a patent airway and properly functioning epiglottis. The patient progressed to being able to eat a regular solid and thin liquid diet post-laryngoscopy. His tracheostomy was subsequently decannulated on hospital day 47, after which he required no oxygen at rest and 3 L nasal cannula with activity. A complete pulmonary function test near discharge was consistent with severe obstructive disease (FEV1 14% predicted) with a severely decreased diffusing capacity of the lungs for carbon monoxide (DLCO). The patient was able to be safely discharged home on hospital day 51.
Since discharge, the patient has had one other admission, experiencing shortness of breath at home and being found to have a small, unilateral, and apical pneumothorax. He was admitted for observation initially and discharged on hospital day 2 after conservative treatment. His most recent chest CT imaging is much improved (Figures 7 and 8) compared to admission. His pulmonary function tests, which continue to improve, show FEV1 22% predicted, FEV1/FVC ratio 36%, and DLCO 64% predicted, consistent with very severe obstructive pulmonary disease with mild diffusion defects. He continues to follow closely with our pulmonology colleagues with the hope of continued recovery in pulmonary function. At the time of this publishing, he has been on a stable medication regimen and is able to enjoy normal activities of daily life.

Most recent chest X-ray showing extensive improvement in consolidations compared with imaging on admission. Residual central bronchiectasis stable post discharge.

(a) Top, coronal slice from most recent CT chest, (b) bottom, axial slice from most recent CT chest showing marked improvement compared to initial imaging but persistent bronchial wall thickening, which is likely from scarring post anhydrous ammonia exposure.
Discussion
Ammonia is one of the most produced chemicals in the United States, the majority of which is used for chemical fertilizers. Household ammonia-based cleaners typically contain 5%–10% ammonia mixed with water and other additives, but in a concentrated or pure form (>99% ammonia) it is referred to as anhydrous ammonia. It is a water-soluble alkali gas that combines with water to form ammonium hydroxide, which is a potent caustic. It is stored and transported in tanks or barrels under pressure in a liquid state, during which it is flammable and presents both a thermal and explosive risk. 2 When released or exposed to air, it expands 850 times in volume to form large vapor clouds that are extremely caustic and may lead to significant injury. Inhalational injury and mucosal membranes are at the highest risk as anhydrous ammonia ingestion is uncommon.3,4
According to the 2022 Annual Report of the National Poison Data System from America’s Poison Centers: 40th Annual Report, 5 there were 1339 single exposures reported that year. The vast majority (90%) of these were unintentional.
Because of its affinity for water, our mucosal membranes are at significant risk when exposed to anhydrous ammonia. 6 It is a powerful irritant and those exposed will usually try to remove themselves from the environment as soon as possible. This is notable for our patient who was found unconscious at the scene of the accident after an estimated exposure time of 40 min. Other individuals in the same or nearby vehicles reported having difficulty breathing, leading to panic and attempting to run from the scene of the accident. Unfortunately, due to the large volume of anhydrous ammonia released and its quick expansion to gaseous form, those exposed were unable to outrun the vapor and may have potentiated inhalational exposure through exerting themselves as they attempted to run away. Unfortunately, two people died at the scene of the accident from anhydrous ammonia inhalation, and three people in a nearby home also died from inhalational injury, including two children. Five exposed patients were airlifted to area hospitals and an additional two patients were treated at the local hospital. 7
With anhydrous ammonia being a potent caustic, the most important target organs are the eyes, lungs, skin, and other mucosal membranes. The lung injury can be significant based on the duration of exposure, and unfortunately, in some cases, permanent. Once exposure has occurred and caustic injury is present, there is no specific antidote or treatment that is more effective than aggressive supportive care. Fortunately, anhydrous ammonia has no real systemic toxicity and should not cause any other organ dysfunction beyond those directly exposed. Serum ammonia levels can be elevated in massive exposures but have not been found to be prognostic.
Patients with short duration/high concentration exposures may fare better than those with extended duration/low concentration exposures, similar to our patient. Extended duration exposures seem to lead to more extensive burns throughout the entire tracheal-bronchial system, perhaps predisposing patients to prolonged ventilatory requirements or even ECMO as a salvage technique. There have been few case reports in the literature about patients with lung injury or ARDS after inhalation of anhydrous ammonia; however, only one regarding the use of ECMO.8,9 A case series published in 2007 covers five cases of ammonia-related inhalational injury of varying severities. 8 Four patients required intubation and were managed on a ventilator and ultimately discharged home. The fifth patient had severe inhalational injury but unfortunately was not an ECMO or lung transplantation candidate and ultimately died. Another published article covers two patients who required ECMO after inhalational injury secondary to anhydrous ammonia. 10 Notably, both patients were successfully weaned off ECMO, but one ultimately succumbed to hematologic complications of mechanical circulatory support. This is the only other published data relating to ECMO use in anhydrous ammonia-related ARDS. The reported death of a patient post-decannulation speaks to the variety of challenges faced in managing these patients, even when apparently recovering from ARDS, and the amount of complications that may occur when ECMO is required. Unfortunately, there is a lack of long-term data as it pertains to these patients related to pulmonary outcomes or even the eventual need for lung transplantation once outside of their initial admission. Our patient continues to see modest improvement in pulmonary function tests but still has severe obstructive disease as was seen in other published cases of anhydrous ammonia exposure. Due to the sporadic nature of these exposures and varying degrees of injury, long-term data will continue to be difficult to obtain, thus, it is important to add case reports to the literature as they occur.
Conclusion
The current case report is significant to the literature for multiple reasons including the exposure mechanism and severity of inhalation, the hospital course of severe ARDS ultimately requiring a 15-day run of VV-ECMO, the extensive sloughing of the respiratory epithelium with necessary removal of tracheal-bronchial casts, supraglottic adhesions secondary to extensive mucosal injury requiring ENT intervention, hospital course involving multispecialty care at a large quaternary burn referral center, and ultimate successful discharge home without the need for lung transplantation. It is our hope that if future unfortunate anhydrous ammonia inhalational injuries occur, this report can serve as evidence that with meticulous multidisciplinary management, patients can recover without the need for lung transplantation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and consent statement
Our institution does not require ethical approval for reporting individual cases or case series. However, patient consent was obtained regarding the publication of the above case report.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.