
Abstract
A 67-year-old woman with morbid obesity and severe obstructive sleep apnea presented to the emergency department with 2 days of productive cough, fever, shortness of breath and loose stools. A chest x-ray showed extensive bilateral infiltrates, and she was quickly intubated for acute hypoxic respiratory failure. A urine legionella antigen test was positive, and she was admitted to the intensive care unit with a diagnosis of severe legionella pneumonia. She improved over the next week with a course of levofloxacin. Once improved, the state health department visited her home and interviewed her husband and determined that she had not been cleaning her continuous positive pressure mask, tubing and humidifier appropriately. They concluded that the legionella likely came from her continuous positive airway pressure equipment. Cases of legionella pneumonia have frequently been reported through infected water supplies and even respiratory equipment. It is crucial that the mask and tubing used with these devices are cleaned appropriately to minimize the risk of infection.
Introduction
Legionella pneumonia is an infection caused by bacteria of the Legionella species, a ubiquitous, naturally occurring, aquatic organism. While various incidences have been reported, Legionnaires’ disease seems to account for 1% to 8% cases of community-acquired pneumonia (CAP) cases.1,2 Legionella infection is equally common in ambulatory and hospitalized patients, and incidence of legionella infection is also increasing in the United States. 3 The mortality rate of appropriately treated community-acquired Legionnaires’ disease in immunocompetent patients is <5% 4 but is clearly higher if not recognized or in immunocompromised hosts. 5
Legionella is generally transmitted to humans through exposure to infected water supplies or water-containing devices. Community-acquired cases have been reported via inhalation of colonized aerosols or droplets from drinking water, cooling towers, whirlpool baths, air conditioners, shower heads, spas and other water sources. Nosocomial cases have been reported due to infected water supplies in hospitals and nursing homes and also through respiratory therapy devices such as nebulizers and non-invasive pressure ventilation devices.6,7
The prevalence of obstructive sleep apnea (OSA) has increased dramatically over the last 20 years and is now estimated to affect over 25 million people in the United States. 8 Continuous positive airway pressure (CPAP) is one of the cornerstones of therapy for OSA, shown to decrease both blood pressure and sleep apnea intensity. It is difficult to get a true estimate of the number of CPAP devices utilized worldwide; however, their numbers are also likely increasing. While all masks are generally recommended to be cleaned every day after use, either with distilled water or warm tap water and then allowed to air dry, the patients utilizing these masks likely represent a growing group of patients at risk of developing legionella.
Case study
The patient was a 67-year-old woman with past medical history of morbid obesity, OSA, diabetes mellitus type 2 and hypertension who presented with 1 day of worsening cough and shortness of breath. She also noted three cases of loose stool, and she presented to the emergency department. In the emergency department, she was treated for presumed influenza and discharged with a prescription of oseltamivir. When she went home, she continued to have shortness of breath, worsening malaise and green productive sputum, so she called for an ambulance the following day. Emergency services found her at home in respiratory distress and with an oxygen saturation of 72% on room air and brought her to the hospital. In the emergency room, she was found to have an oxygen saturation of 96% on 5 L/min of O2, temperature of 37.3°C, RR 32 and blood pressure of 172/80. She was admitted to hospital with a diagnosis of CAP and treated with intravenous ceftriaxone and azithromycin.
Upon admission to the hospital, she quickly deteriorated with worsening hypoxia. On the day after admission, she was admitted to the intensive care unit (ICU) and intubated for acute hypoxic respiratory failure. Initially she was treated with ceftriaxone and azithromycin, but when the urine legionella testing came back positive, she was changed to high-dose levofloxacin at 750 mg/day. She remained on the ventilator for 4 days, was extubated and was able to be discharged to a rehabilitation facility at day 11 with plans to continue levofloxacin for a total of 14 days.
Her chest x-ray (Figure 1) showed multifocal airspace opacities which were read as possible pneumonia, aspiration or pulmonary edema.
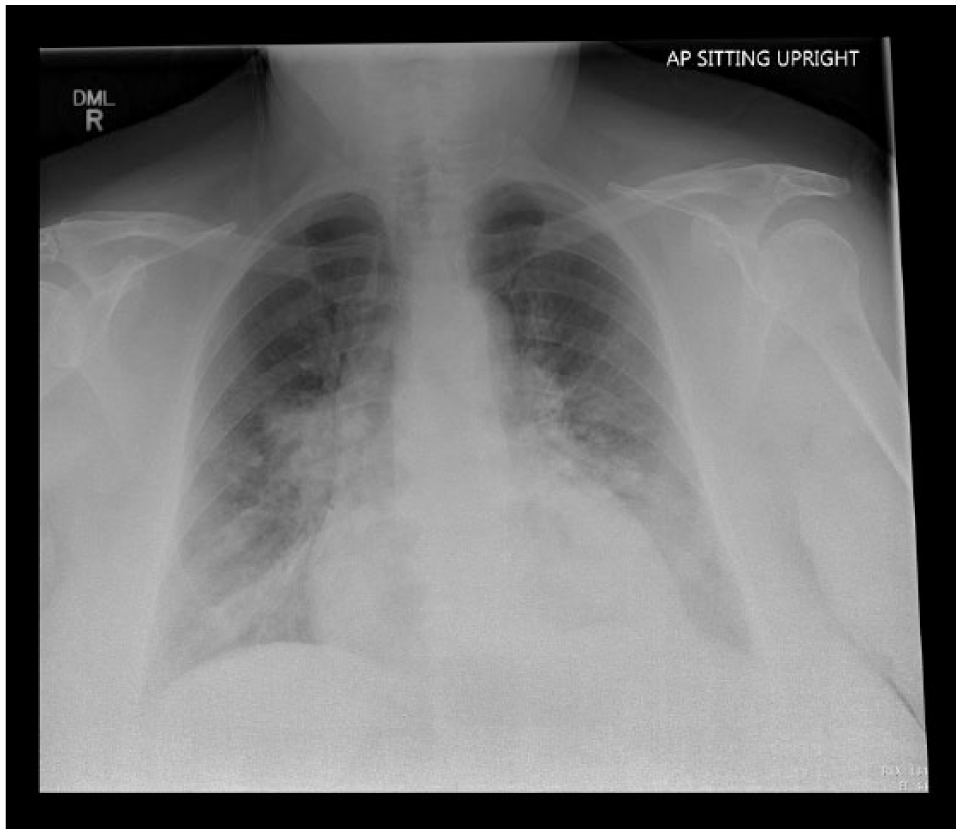
Chest x-ray of patient when she represented to the hospital emergency department. Significant for multifocal infiltrates with a differential of multifocal pneumonia, aspiration or alveolar edema.
As an outpatient, she has utilized CPAP with a humidifier with settings of 12 cm H2O since 2008 with good adherence before this admission. Cleaning recommendations were given to the patient during multiple visits and included daily cleaning of the face mask and weekly cleaning of the tubing with detergent and water. In addition, recommendations to replace the entire interface every 6 months were also made. During the inpatient admission, the case was reported to the State of Rhode Island Department of Health (DOH) as required by local laws. The DOH investigated the case, visited the patient’s home and interviewed the patient’s husband. They found used CPAP equipment which did not appear to be regularly cleaned and expect this was the cause of her legionella pneumonia. They did not test the equipment specifically for legionella. They recommended that she discard the old machine, tubing and humidifier and get new equipment.
In follow-up, the patient has done well after discharge, obtained new equipment and continues to use CPAP for her OSA.
Discussion
Legionnaires’ disease was first described after an outbreak in 1976 at an American Legion convention in Philadelphia. 9 Another large outbreak of Legionnaires’ disease occurred in Spain in 2001, where 800 cases were suspected and 449 cases were confirmed, and the epidemiologic investigation implicated the cooling tower of a city hospital. 10 Many individual cases and several outbreaks have been reported since then, usually able to be traced to a contaminated water supply11,12 and even pools and decorative fountains. 13
Non-invasive positive pressure ventilation and CPAP, with its associated masks and tubing, are also potential sources of legionella infection, especially if the equipment is not cleaned appropriately. Use of non-invasive positive pressure ventilator was epidemiologically linked to nosocomial Legionnaires’ disease in 18 patients over a period of 2 years when this equipment was cleaned with only tap water. 6
As the number of obese patients is increasing, associated chronic illnesses linked to obesity, such as OSA, are also increasing in number. 8 Many of these patients will be treated with CPAP at home and must be instructed how to clean their devices appropriately. The mask, which touches the patient’s face, should be cleaned daily with distilled water. Rinsing the face mask or tubing with tap water, instead of using distilled water, or adding tap water in the humidifier is a potential source of legionella colonization. Most recommend that the tubing and humidifier be cleaned at least weekly. Some suppliers also recommend cleaning the mask and tubing with vinegar and water daily. 14 In addition, masks and tubing are designed to be disposable; they should not be used more than their recommended periods, which is generally 3–6 months for CPAP masks.
Conclusion
In this report, we present the case of a woman with OSA on home CPAP who developed a severe case of legionella pneumonia, most likely due to a contaminated CPAP machine and equipment. She had not been cleaning her mask, tubing and humidifier as recommended. This case demonstrates an important public health concern. As more and more people use home CPAP and nasal intermittent positive pressure ventilation (NIPPV), they need to be educated about the importance of cleaning their equipment in order to minimize the risk of infection.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.