
Abstract
Myxomatous degeneration of a valve is a non-inflammatory degenerative process due to the disruption of the fibrous layer of the valve with mucopolysaccharide accumulation. It is mostly seen in the mitral valve but involvement in only aortic valve is rare. Here we present a case report of a 37-year-old man who came with shortness of breath for the past three months and was diagnosed with severe aortic regurgitation due to myxomatous aortic valve causing rupture of the non-coronary and right coronary cusp. After preoperative workup, he was taken for aortic valve replacement surgery. Intraoperative findings confirmed the rupture of right and non-coronary cusps from their annular attachment and the myxomatous nature of the aortic valve. Histopathological examination confirmed the myxomatous changes in the valve. The patient underwent aortic valve replacement with a 23 mm TTK Chitra valve and on follow-up, he is doing well. Although aortic valve regurgitation is a common disease, myxomatous degeneration of isolated aortic valve leading to aortic regurgitation is rare. This patient did not have any signs of connective tissue disorders like Marfan’s syndrome, Ehlers-Danlos, etc., but presented with myxomatous aortic valve throwing an insight into further research into this rare disease.
Keywords
Introduction
Aortic regurgitation is a condition where the blood from the aorta goes back to the left ventricle because of non-coaptation of leaflets or dilatation of the aortic root. The most common cause of aortic regurgitation in India is rheumatic heart disease. Other causes include infective endocarditis, congenital valvular diseases, connective tissue disorders like Marfan’s syndrome, etc. 1 Rheumatic heart disease is the most common cause for AR in India and South Asian countries, whereas bicuspid aortic valve and connective tissue disorders are common causes in western countries. Myxomatous degeneration is usually seen in the mitral valve causing prolapse of its leaflets and leading to mitral regurgitation, 2 but in a few cases, it has been reported in the aortic valve leading to aortic regurgitation.3–7 Here we report a rare case of a 37-year-old male with no comorbidities, no signs of Marfan’s syndrome, or other connective tissue disorders having isolated myxomatous aortic valve causing severe aortic regurgitation.
Case presentation
A 37-year-old male came with chief complaints of shortness of breath for the last three months which was progressive in nature. The patient had a history of hospitalization at a local hospital one month ago due to heart failure where he was diagnosed with aortic regurgitation. The patient came with similar complaints to our hospital and was admitted. He denies a history of rheumatic fever and has no signs of rheumatic heart disease, no symptoms, and no signs of infective endocarditis. He had no history of fever, and his Anti-streptolysin O titers and C-reactive protein were normal. There were no signs like Osler’s nodes, Janeway lesions, etc. which are seen in infective endocarditis.
The patient’s height is 174 cm and weight is 70 kg. He has no signs of Marfan’s like wrist sign or thumb sign and did not have facial deformities like sunken eyes, flexible skin, etc. that are seen in Ehlers-Danlos, etc. The patient did not have signs of hypertelorism, cleft palate, signs of aortic aneurysm, etc. that are seen in Loeyz-Dietz syndrome. Differential diagnoses included connective tissue disorders, infective endocarditis, and bicuspid aortic valve disease which were ruled out by history, clinical examination, and investigations like transthoracic echocardiography and intraoperative transesophageal echo.
His vitals were BP of 130/40 mm Hg in the right arm and a heart rate of 90 beats per minute with bounding peripheral pulses. On auscultation, there was an early diastolic murmur in the aortic area of grade 3/6. ECG showed LV volume overload features. Preoperative echo revealed a myxomatous aortic valve with rupture of the right and non-coronary cusp from their annular attachment causing severe eccentric aortic regurgitation. The aortic valve was tri-leaflet with normal ascending aorta and aortic root. The aortic annulus was 2.7 cm and the ascending aorta was 3.2 cm, with normal mitral valve anatomy and trivial mitral regurgitation, dilated left ventricle, and good left ventricular function with EF of 65% as shown in Figure 1. The patient was planned for aortic valve replacement surgery.
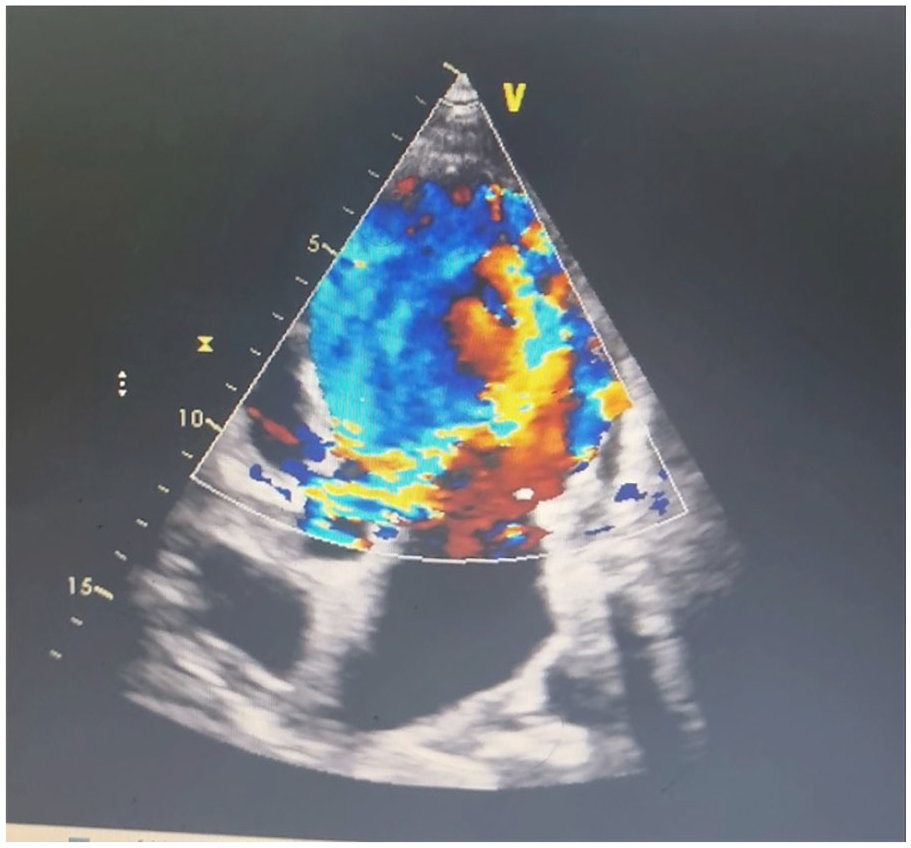
Transthoracic echocardiography image shows severe eccentric aortic regurgitation.
Surgery was done routinely with midline sternotomy, thymus dissection, pericardiotomy, and cardiopulmonary bypass instituted with aortic and right atrial cannulation and LV vent. After cross-clamping the aorta and aortotomy, the heart was arrested with direct osteal cardioplegia using del Nido cardioplegia solution. Intraoperative findings confirmed with 2d Echo findings, which showed a tri-leaflet valve with rupture of both right coronary and non-coronary cusp from their annular attachment as shown in Figure 2 which is unique and rare and not widely reported. Valve cusps were thickened at some points. Repair of the aortic valve was not possible because of extensive rupture of both cusps; hence, AVR was done with a 23 mm TTK Chitra valve using 18, 2-0 polyester non-pledgeted mattress sutures. Part of the valve cusp was sent to microbiology which showed no growth of bacteria.

Intraoperative image shows a ruptured aortic valve cusp (from its annulus).
The remaining part of the operation was uneventful and postoperative stay was also uneventful. Excised valve cusps were sent for histopathological examination which confirmed myxomatous degeneration as shown in Figure 3. Although myxomatous aortic valve disease is predominantly seen in old age group4,5 here it was presented in an otherwise normal 37-year-old individual suggesting further research into this disease. On follow-up, he is doing well.

Histopathological examination slide. HPE slide shows myxomatous changes with mucopolysaccharide accumulation.
Discussion
Aortic regurgitation is most commonly caused by rheumatic heart disease, bicuspid aortic valve disease, infective endocarditis, genetic disorders like Marfan’s syndrome, Ehlers-Danlos syndrome, etc. Myxomatous degeneration of the aortic valve was first described in 1957, although less commonly affected than the mitral valve.3,7 Myxomatous degeneration is characterized by a non-inflammatory process that results in thin and translucent regions macroscopically and disruption of the fibrosa layer due to collagen fiber fragmentation and acid mucopolysaccharide accumulation in the spongiosa microscopically.
In developed countries, the incidence of myxoid degeneration of uncertain origin is about 5% to 10% as per reports suggested by Allen et al. 7 but it was mostly seen in old age individuals of the sixth and seventh decades as per multiple reports.4,5,7
However, in our case report, the patient is a young individual of 37 years of age with no comorbidities, no marfanoid features having myxomatous degeneration of the aortic valve causing severe AR. Though such cases are rare as per Kyi et al., 3 unlike that case, the patient reported here had no history and signs of infective endocarditis and no findings like vegetations on the valve in transthoracic as well as in intraoperative transesophageal echo, thus ruling out infective endocarditis and valve culture was negative.
His other valves were normal and presented with isolated myxomatous degeneration of the aortic valve. According to Akasaka et al., 8 myxomatous degeneration can present as rupture of a part of the aortic valve, however in the case reported, it presented with rupture of both non and right coronary cusps from their annular attachment as depicted in Figure 2, which is unique and rare and not widely reported.
This provides valuable insight into further research regarding rare causes of AR in India which have not been done as per our knowledge. A cohort study reported that myxomatous degeneration has a familial dominance mapped to the Xq28 gene leading to an imbalance between synthesis and degradation of the extracellular matrix. 9 Although myxomatous mitral valve regurgitation repair can be done, for cases of myxomatous aortic valve causing severe AR it is a reasonable option to do aortic valve replacement for complete recovery from symptoms. 1
Conclusion
Myxomatous degeneration of the aortic valve is a rare cause of aortic regurgitation, especially in young individuals with unknown origin of AR. Myxomatous degeneration must be considered in differential diagnosis and further research must be done to know the genetic nature of this disease.
Footnotes
Acknowledgements
None.
Author contributions
R.K.K. first author, manuscript preparation and supervision; V.S.S. corresponding author, manuscript preparation, data collection, preparation of case report; N.A. supervision of manuscript, insight to previous reports.
Data availability
Data sharing is not applicable to this as no datasets were generated in this report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual case reports.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this case report
Consent for publication
Informed consent was obtained from the patient’s legal guardian for the publication of the case report.