
Abstract
Radicular cysts are rarely present in the primary dentition because of the distinct biological cycle of primary teeth. Cyst formation in children may cause bony expansion and resorption, malposition, delayed eruption, enamel defects, or damage to the developing permanent successors. Various treatment modalities for the management of radicular cysts have been reported in the literature. In this case, the preferred treatment approach is window decompression surgery (WDS) combined with gap retainers. Long-term follow-up revealed good healing of the bony lesion. The present case involved an abnormally large radicular cyst in a 7-year-old girl. After surgery, WDS was performed, and a gap retainer was provided. At the 9-month follow-up, the radicular cyst had healed and the impacted tooth had erupted. The aim of this study was to explore the clinical effectiveness of WDS for impacted teeth within root radicular cysts.
Introduction
Radicular cysts originate from epithelial remnants of the periodontal ligament as a result of inflammation and associated inflammatory cell infiltration, which is usually a consequence of pulp necrosis. These cysts usually involve the apex of the affected tooth. 1 Caries is the most frequent etiology of radicular cyst formation in primary dentition. Compared with that in permanent teeth, the incidence of radicular cysts in deciduous teeth is lower. The reason for this discrepancy may be that deciduous teeth exist in the oral cavity for a short period, inflammation in many accessory root canals, pulp, and periapical tissues is more likely to cause drainage, and symptoms may appear later, which can cause the rate of early visits for a cyst to be relatively low.2,3 The common deciduous teeth in which cysts occur are mandibular molars (67%) because they are prone to caries, and the mandibular cortex is thick, making it difficult for fistulas to form. Inflammatory exudates are not easily drained, resulting in radicular cysts. Cyst formation in children may cause bony expansion and resorption, malposition, delayed eruption, enamel defects, or damage to the developing permanent successors. 4 One of the most suitable treatment options for these patients is window decompression surgery (WDS), which involves extraction of the associated primary teeth and preservation of the permanent teeth. In most cases, impacted teeth erupt spontaneously, even if they are initially in an unfavorable position. 5
This article presents a case of a large radicular cyst resulting from periapical periodontitis in the deciduous molar region of a 7-year-old child. After the patient’s deciduous teeth were extracted, the cyst cavity was irrigated with physiological saline, and the wound was packed with a small amount of iodine-impregnated gauze to ensure proper drainage. After 9 months of follow-up, the development of the permanent tooth germ continued, demonstrating effective treatment outcomes. The aim of this study was to explore the clinical effectiveness of WDS for impacted teeth within root radicular cysts.
Case presentation
A 7-year-old girl sought medical attention due to uneven dentition, and examination revealed a cyst on the right side of the mandible. The oral examination revealed residual roots of the first and second primary molars in the lower right region, accompanied by slight enlargement in the buccal vestibular area. There was no active discharge of pus and no palpable lymph nodes were detected (Figures 1(a) and 2(a)). Radiological examination (RE) revealed a round radiolucent unilocular lesion with smooth and well-defined borders extending 17 × 18 mm in the periapical area of the lower right first and second primary molars. The integrity of the permanent tooth embryonic bone crypt was damaged. Distant displacement of the tooth embryo and discontinuous imaging of the tooth sac bone wall were observed (Figure 1(b)). The initial diagnosis, on the basis of the clinical and RE findings, was a radicular cyst. The preferred treatment approach is WDS combined with gap retainers. For preoperative preparation and wearing of gap retainers, the primary right first and second deciduous molars were extracted intraoperatively. A fenestration procedure was performed through the extraction socket, and iodoform gauze strips were placed inside the cyst. A tissue sample was also taken for biopsy.
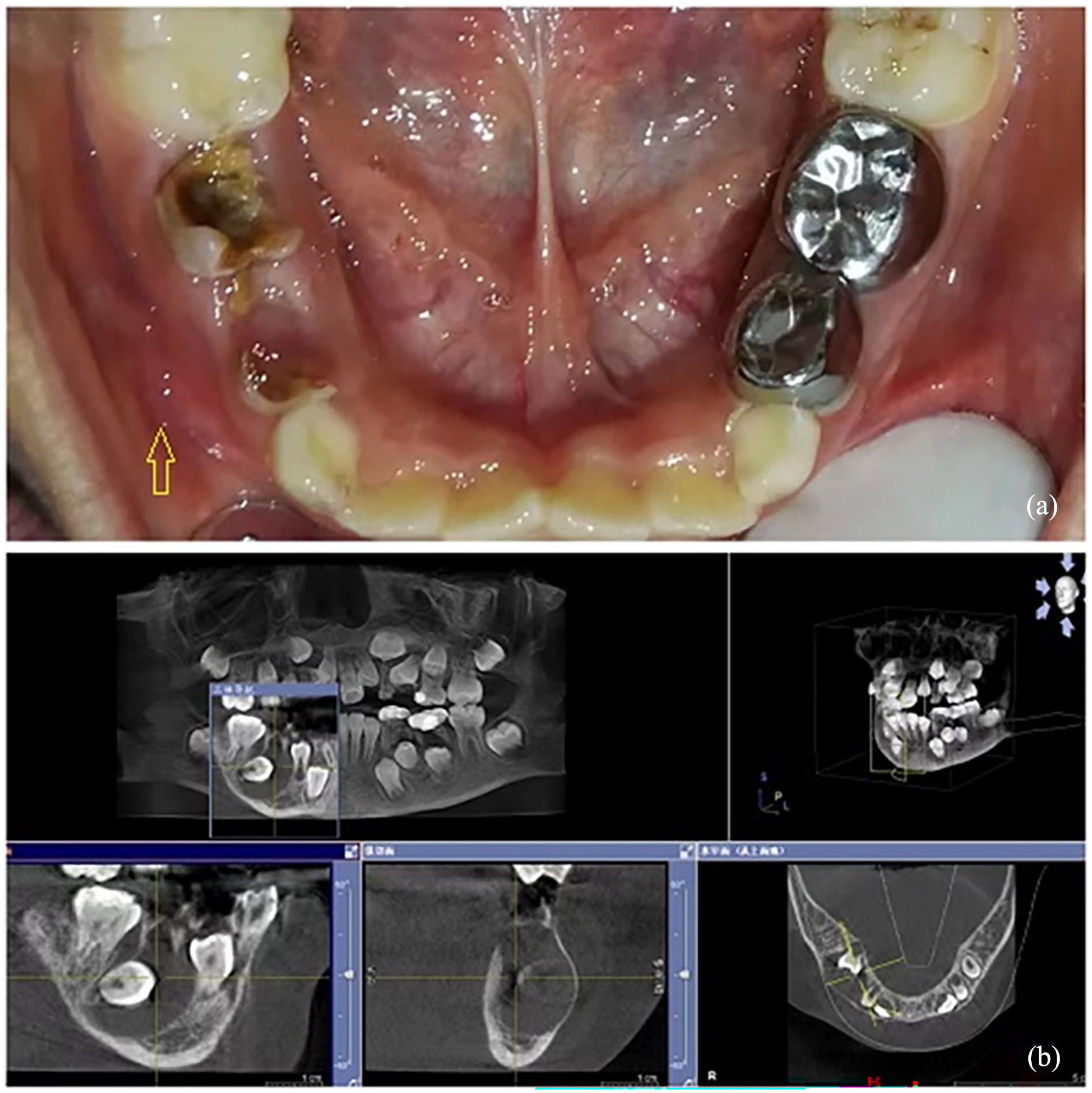
(a) Preoperative intraoral view of the patient. (b) Preoperative cone beam CT images.

(a) Preoperative panoramic radiography of the patient. (b) Postoperative radiography of the patient at the third month. (c) Postoperative radiography of the patient after 5 months. (d) Postoperative panoramic radiography at 9 months.
Histopathologic examination of the sample confirmed our initial diagnosis of a radicular cyst (Figure 3(a)). The iodoform gauze strip was replaced once per month for 3 months postoperatively.
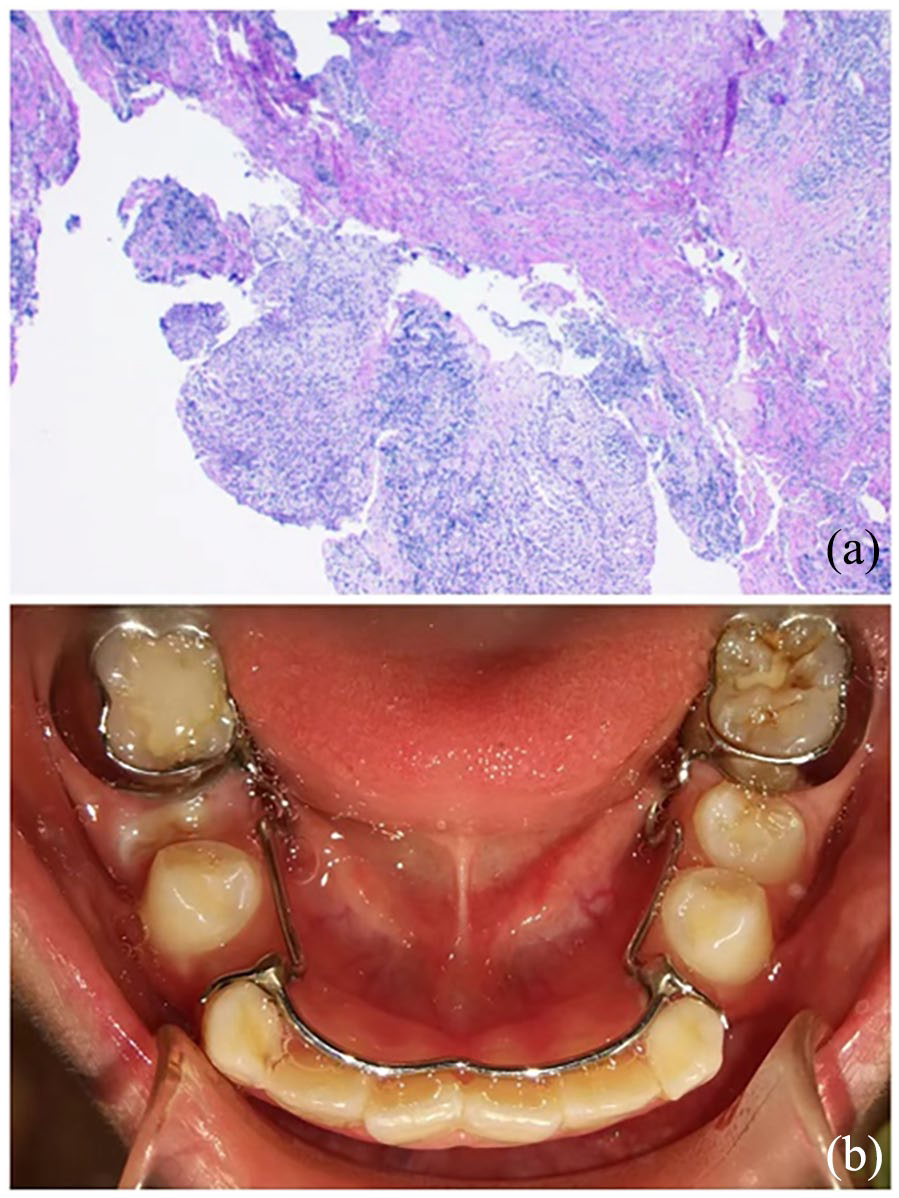
(a) Histopathologic image of the lesion (H&E staining ×200). (b) Postoperative intraoral view of the patient.
RE at the third-month follow-up visit revealed a decrease in radiolucency at the cyst site (Figure 2(b)). After 5 months, the direction of eruption of the impacted teeth tended to be normal, and new bone formation was evident at the former cyst site (Figure 2(c)). A panoramic radiograph taken at the 9-month follow-up revealed spontaneous eruption of the impacted lower second premolar and first premolar, with no radiolucency around the teeth (Figure 2(d)). The oral examination revealed eruption of the first and second premolars on the right side (Figure 3(b)). The patient’s dentition was moderately crowded, and orthodontic treatment was recommended. The patient’s were satisfied with the current treatment effect and temporarily refused orthodontic treatment.
Discussion
Radicular cysts are a common type of jaw cyst. Typically, they grow slowly with no noticeable symptoms in the initial stages. However, continued growth can cause the bone to swell, resulting in facial deformities. Traditional surgical removal is effective but has numerous drawbacks. Currently, some researchers have adopted WDS, which is straightforward, and minimally invasive, enhances the retention rate of embedded teeth within cysts, reduces the incidence of facial deformities, and enhances the quality of life of patients.
WDS is a minimally invasive surgery performed under local anesthesia that can open the bone, expose the cyst cavity, aspirate the cyst fluid, and fill it with iodine gauze to keep the drainage port unobstructed. The cyst cavity communicates with the oral cavity, alleviating the hydrostatic pressure within the cyst and mitigating or halting bone resorption. Moreover, the diminished pressure within the cyst produces negative charges that can stimulate the growth of osteoblasts and cause the cyst cavity to regress. During surgery, the cyst fluid is also aspirated, eliminating the involvement of adjacent bone resorption in the cyst and causing the growth of bone around the cyst cavity, thereby achieving the goal of shrinking and curing the cyst. Moreover, measures such as systemic anti-inflammatory treatment, local flushing and dressing changes, and iodoform gauze packing can exert anti-inflammatory and anticorrosive effects, which are beneficial for the treatment of cysts. This treatment method can prevent damage to adjacent tooth germs and their roots during scraping surgery.
In this case, following the extraction of deciduous teeth, a fenestration procedure was performed through the extraction socket to minimize surgical trauma. This simultaneously creates a pathway for the embedded tooth within the cyst to erupt, directing its growth into the dental arch and setting the stage for subsequent normal jaw development. Iodine-impregnated gauze strips serve as antiseptic and disinfectant, and their soft consistency minimally interferes with the embedded tooth within the cyst, thereby facilitating its eruption. Additionally, following the removal of deciduous teeth, adjacent teeth often incline and displace into the vacancy. Wearing a space maintainer helps preserve the gap between adjacent teeth, creating an appropriate space for the eruption of the embedded tooth. Compared with adults, children have a greater ability to regenerate bone structures. In addition, teeth with open root tips have great potential for eruption. These factors are highly important in cases of large root cysts in children and are associated with a better prognosis of affected teeth.6,7
The early diagnosis and correct selection of treatment plans for deciduous tooth diseases are particularly important for the healthy development of inherited permanent tooth embryos. For this purpose, it is necessary to conduct regular clinical and radiographic follow-up for deep caries or pulp-treated primary teeth.8,9
Conclusion
The treatment plan for this patient was simple and atraumatic. Postoperatively, all the clinical and radiographic findings revealed normal features, new bone formation, and spontaneous eruption of the impacted teeth in the correct position after only 9 months. Since immature teeth with incomplete root formation and open apices have optimal eruption potential and children have much greater bone regeneration capabilities than adults do, conservative surgical techniques are usually successful for young patients.
Footnotes
Acknowledgements
The authors express their appreciation for the valuable insights from the past literature.
Author contributions
G.S. wrote the manuscript; L.W. performed the data analysis; L.G. performed the formal analysis and validation.
Data availability statement
The data are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Ethics Committee of Tianjin Baodi Hospital (APPROVAL NUMBER lunli 7489). The authors affirm that the parents of the patient depicted in the images or other personal information provided written informed consent for the dissemination of the findings for educational and research purposes.