
Abstract
We present a case in which renal mixed epithelial and stromal tumor (MEST) was considered in the differential diagnosis based on preoperative imaging findings. A 38-year-old woman was found to have a right renal tumor during an abdominal ultrasound examination conducted as part of a health checkup. Contrast-enhanced computed tomography revealed a 50 × 40-mm mass in the middle of the right kidney. The possibility of papillary renal cell carcinoma was considered. However, given the patient’s age, sex, and characteristics of the mass, MEST was also considered a differential diagnosis. The patient underwent laparoscopic radical right nephrectomy. The tumor was diagnosed as MEST.
Introduction
Mixed epithelial and stromal tumor (MEST) is a relatively rare neoplasm. MEST of the kidney is typically benign and predominantly occurs in middle-aged women. A definitive diagnosis is challenging using imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI), and it usually necessitates pathological examination. In this report, we present a case in which renal MEST was considered in the differential diagnosis based on preoperative imaging findings.
Case presentation
A 38-year-old woman presented to our hospital following the detection of a right renal tumor during an abdominal ultrasound examination conducted as part of a health checkup. The patient had no history or comorbidities, was not taking any medications, and had no allergies. Contrast-enhanced CT was performed, which revealed a 50 × 40-mm mass in the middle of the right kidney. The mass exhibited well-defined and smooth margins, consisting of a progressively enhancing solid component and cystic portion (Figure 1). Due to the presence of a solid component, the possibility of papillary renal cell carcinoma was considered. However, given the patient’s age, sex, and characteristics of the mass, MEST was also considered as a differential diagnosis. Based on the results of CT, we recommended surgical treatment for the patient. However, the patient expressed a preference for less invasive treatment options and sought a second opinion at another institution, where surgery was also recommended. We subsequently presented the patient with a choice between radical nephrectomy and partial nephrectomy as treatment options. The patient requested a radical nephrectomy. Consequently, she underwent a laparoscopic radical right nephrectomy. Macroscopically, a well-circumscribed 5 × 4 × 3.5-cm whitish tumor was observed, comprising both cystic and solid components (Figure 2). Microscopically, the tumor tissue exhibited a mixture of stromal areas of collagen fibers and spindle-shaped cell proliferation with vitrification and various glandular luminal structures formed by poorly atypical epithelium (Figure 3(a) and (b)). Immunohistochemically, the stromal component was positive for estrogen receptor (ER), progesterone receptor (PgR), and desmin (Figure 3(c) and (d)). The epithelial component was positive for AE1/AE3, PAX8, and CK7. Based on these findings, the tumor was diagnosed as MEST. The patient has experienced no recurrence for approximately 1 year postoperatively.

CT findings. CT revealed a 50 × 40-mm mass in the middle of the right kidney. The mass exhibited well-defined and smooth margins, consisting of a progressively enhancing solid component and cystic portion (arrow). (a) Axial, arterial phase. (b) Coronal, arterial phase. (c) Axial, nephrographic phase. (d) Coronal, nephrographic phase.

Macroscopic findings. A well-defined, milky-white mass measuring 5 × 4 × 3.5 cm was observed. The interior of the tumor consisted of a mixture of cystic and solid components (arrow).

Pathological findings. (a) Pathological examination with hematoxylin-eosin staining revealed areas with a leaf-like structure, fibrous stromal components, and various glandular formations composed of epithelial cells with low-grade atypia. (b) Some areas of cystic expansion were lined with hobnail-shaped epithelial cells. The stroma exhibited a focal proliferation of spindle-shaped cells with a wavy pattern, resembling ovarian stromal cells. (c) Immunohistochemical staining results revealed that the stromal component was positive for ER. (d) PgR also showed positivity.
Discussion
MEST is a neoplasm characterized by the coexistence of epithelial and stromal components. Malignant transformation is rare, and the tumor is typically unilateral and solitary. Historically, MEST has been referred to as “congenital mesoblastic nephroma in an adult,” “adult mesoblastic nephroma,” or “adult cystic nephroma” among others. 1 However, the term MEST is now widely accepted. 2 In addition to the kidney, MEST has also been reported to arise from the renal pelvis and seminal vesicles.3,4 The condition predominantly affects middle-aged women, with a reported female-to-male ratio of 7–10:1. The age range of patients typically spans from 36 to 80 years, with a mean age of 49.7 years.5,6 An association between MEST and estrogen exposure has also been suggested due to the occurrence of these tumors in women undergoing hormone replacement therapy and in men receiving androgen deprivation or estrogen therapy for prostate cancer. 7 However, our patient had no history of hormone replacement therapy.
Imaging findings, although not diagnostically definitive, play a crucial role in the evaluation of MEST (Table 1). CT and MRI are particularly valuable for identifying key features of these tumors. On CT, several small calcifications can be observed within the mass, along with cystic components. The tumor generally presents with a well-defined boundary, displaying both multilocular cystic areas and solid components. The ratio of cystic to solid areas varies widely, with some tumors being predominantly cystic, while others have a larger solid component. The solid areas of the tumor exhibit gradual enhancement after contrast administration.1,8 On MRI, the fibrous septa within MEST appear hypointense on T2-weighted imaging, while the cystic fluid components demonstrate signal intensities similar to that of water. The solid portions of the tumor exhibit signal intensity comparable to the renal cortex on T1-weighted images and show low signal intensity on T2-weighted images, possibly reflecting the presence of abundant fibrotic tissue. Hemorrhagic changes are rare in these tumors.1,9 These imaging characteristics are important for distinguishing MEST from other renal tumors. However, distinguishing MEST from other types of cystic renal carcinomas is challenging when relying solely on imaging characteristics (Table 2). 10 The Bosniak classification system of renal cystic masses divides renal cystic masses into five categories based on imaging characteristics on contrast-enhanced CT and MRI and helps predict risk of malignancy and suggests either follow-up or treatment.11,12 Several reports indicate that MEST cysts observed on CT and MRI scans often correspond to Bosniak classification III.6,13–15 In the present patient, regarding CT findings, the mass displayed well-defined, smooth margins and comprised a progressively enhancing solid component along with a cystic portion (Figure 1). Due to the presence of the solid component, the possibility of papillary renal cell carcinoma was considered. However, based on the patient’s age, sex, and characteristics of the mass, MEST was also considered a differential diagnosis.
Imaging and clinical findings suggesting MEST.

MEST: mixed epithelial and stromal tumor.
MEST versus other adult cystic renal lesions.
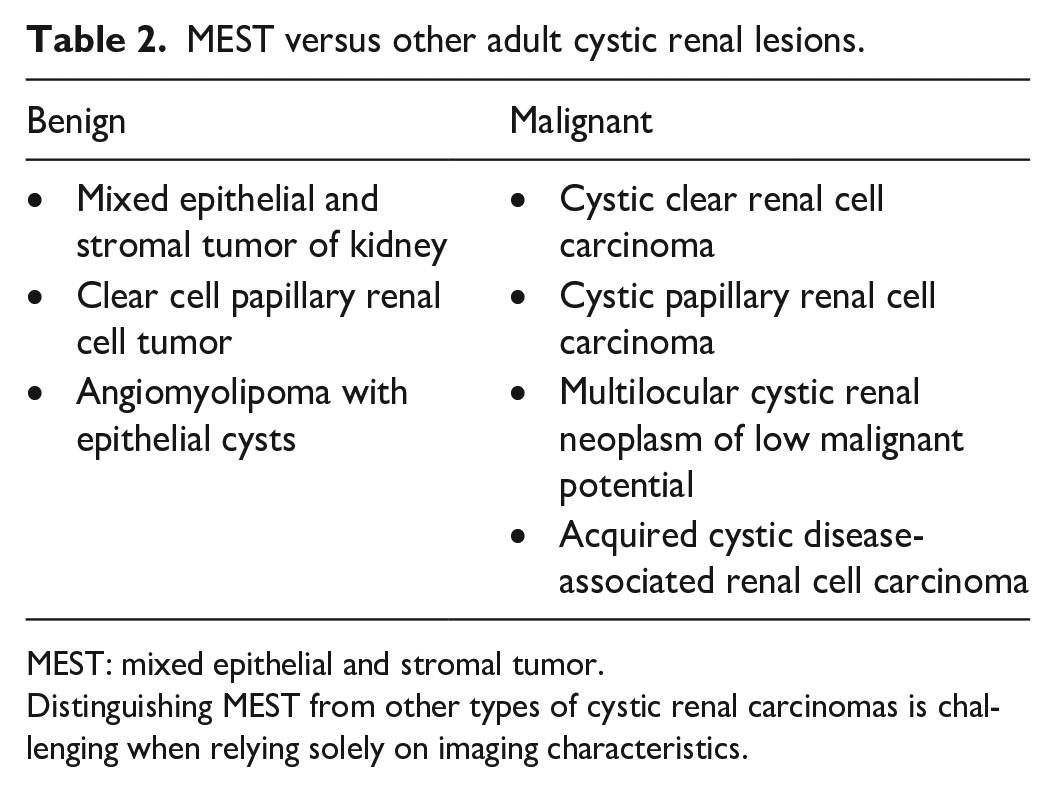
MEST: mixed epithelial and stromal tumor.
Distinguishing MEST from other types of cystic renal carcinomas is challenging when relying solely on imaging characteristics.
Macroscopically, MEST is typically unilateral and solitary and composed of a well-demarcated mass that contains both solid and cystic areas. The cystic components vary in size and shape, and they are usually filled with serous fluid. Histologically, MEST is characterized by a mixture of epithelial and stromal components. The epithelial component consists of cysts and glands of varying sizes, while the stromal component ranges from dense to loose connective tissue. A feature of MEST is the significant variability in the morphology of the cells that comprise each component. Immunohistochemically, the epithelial component is positive for markers such as cytokeratin (AE1/AE3), GATA3, PAX2, and PAX8. The stromal component, however, is positive for desmin, ER, PgR, and CD10. 7 In the present patient, immunohistochemically, the stromal component was positive for ER, PgR, and desmin (Figure 3(c) and (d)). The epithelial component was positive for AE1/AE3, PAX8, and CK7. Based on these findings, the tumor was diagnosed as MEST.
In recent years, the determination of histological subtypes through needle biopsy has become increasingly important to select appropriate treatments for renal cancer patients. While it would be ideal to diagnose MEST through needle biopsy, it is characterized by the presence of various cell types and structures, making a definitive diagnosis solely through needle biopsy challenging. There have been case reports where a diagnosis of MEST was confirmed through partial nephrectomy of one kidney, followed by the diagnosis of MEST in the contralateral kidney through needle biopsy, with subsequent observation without surgical intervention. 16 However, no reports were identified where a definitive diagnosis of MEST was made solely through needle biopsy.
In the present patient, the preoperative CT findings indicated the potential presence of MEST. Since the imaging findings did not completely rule out the possibility of malignancy, and considering the tumor’s location and size, partial nephrectomy was deemed challenging. Furthermore, the patient requested a radical nephrectomy, leading to the decision to perform a radical nephrectomy. Considering the patient’s age, sex, and biological characteristics of MEST, partial nephrectomy should have been recommended, even though the tumor’s location posed procedural challenges.
In the differential diagnosis of renal tumors, it is important to consider MEST, especially in middle-aged women who present with both cystic and solid components in imaging studies. While imaging modalities like CT and MRI can suggest the possibility of MEST, definitive diagnosis remains challenging due to the tumor’s histological complexity and variability. Consequently, surgical intervention is often necessary for accurate diagnosis and treatment. Knowledge of the clinical and imaging features of MEST may facilitate a treatment plan that preserves renal function.
Conclusion
MEST should be considered a differential diagnosis for renal tumors when imaging findings reveal well-defined, smooth margins, a progressively enhancing solid component, and a cystic portion. In addition, the patient’s gender and age at the time of diagnosis are important factors to consider. A preoperative diagnosis based on imaging studies can be challenging, and total or partial nephrectomy remains the only definitive method for establishing a specific diagnosis. However, when preoperative imaging and clinical features suggest that MEST should be included in the differential diagnosis, careful consideration should be given to preserving renal function through options such as partial nephrectomy, rather than opting for total nephrectomy, even in the presence of technical difficulties.
Footnotes
Author contributions
H.N. writing – original draft; writing; M.T. writing – review and editing; K.I. writing – review and editing; G.H. writing – review and editing; K.I. writing – original draft; writing; N.H. writing – review and editing; T.N. writing – original draft; writing – review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Registry and registration no. of the study/trial
Not applicable.