
Abstract
Paraspinal hematomas are common complications following spine surgery. In general, these hematomas are asymptomatic and resolve without issue. Unfortunately, there is a paucity of literature that describes the recurrence of these hematomas in a chronic setting. This case report describes a patient with a chronic recurrent calcified paraspinal hematoma that first developed over 4 years and then reoccurred 11 years later at the same site. The case features a 53-year-old female presented with severe lumbar back pain and right lower extremity radiculopathy in which she underwent a lumbar decompression posterior spinal fusion from L3 to L5 in 2008. Postoperatively, she developed a lumbar paraspinal hematoma which was treated with aspiration followed by conservative management. Four years later, the patient had a large paraspinal mass removed from a similar location in an outside medical facility. The procedure required the assistance of plastic surgery for flap closure and a pathologic review of the mass revealed a calcified hematoma. Ten years later, the patient sought treatment from her index surgeon for a recurrence of the lumbar mass with new onset radicular symptoms. Magnetic resonance imaging of the lumbar spine confirmed the presence of a large paraspinal mass. The patient proceeded with the removal of hardware, revision of laminectomy, revision of posterior instrumentation from L2 to L5, and removal of the lumbar mass. The pathology report classified the mass as a chronic calcified hematoma. The patient remains symptom-free for 1 year following the revision procedure. This case demonstrates an extremely rare presentation, ill-described in the existing literature, of a recurrent symptomatic calcified lumbar paraspinal hematoma requiring repeat operative intervention.
Introduction
Paraspinal hematomas are common complications following spine surgery. In general, these hematomas are asymptomatic and resolve without issue. Unfortunately, there is a paucity of literature that describes the recurrence of these hematomas in a chronic setting. For this reason, we present this case report with a review of postoperative complications following lumbar spine surgery. In an extensive systematic review by Nasser et al., 105 studies were selected containing 79,471 patients and 13,067 reported complications, the overall incidence of postoperative complications in spinal surgery was observed to be 16.4%; with thoracolumbar procedures carrying a higher incidence (17.8%) compared with cervical procedures (8.9%). 1 Of the thoracolumbar procedure complications described in this systemic review, we found that only 8 of the 75 (10.7%) studies included “hematoma” as a specific complication. A case–control study by Cao et al. observed an 18.02% incidence of wound healing issues following lumbar surgery with a posterior midline approach, including incision exudates, swelling, blisters, bruising, superficial/deep incisional infections, and poor healing, but no mention of spinal masses or chronic hematoma. 2
Symptomatic postoperative hematomas are a known complication in the epidural space with incidence ranging from 0.4% to 0.52% that can lead to paralysis or intractable pain.3–5 Early detection and evacuation of hematomas are the keys to avoiding neurologic deterioration and having better clinical outcomes.3–5 Major documented risk factors contributing to postoperative epidural hematoma development are high-level trauma, advancing age, anticoagulation, vascular malformations, hemophilia, lumbar puncture, spinal anesthesia, tumor, pregnancy, immune-mediated vasculitis, and arterial hypertension.6–8 However, there is much less data regarding chronic symptomatic spinal hematoma. To our knowledge, there has not been a reported case of chronic paraspinal symptomatic calcified hematoma requiring multiple resections following open lumbar spine surgery. In presenting this report, we examined the relevant literature regarding this complication using combinations of the following search terms, “spine,” “hematoma,” “extradural,” “chronic,” “recurrent,” “postoperative,” and “calcified.” Furthermore, we present our experience with this rare complication and subsequent surgical management.
Case description
A 53-year-old obese female with a body mass index of 50, a history of type 2 diabetes, hyperlipidemia, and hypertension presented to the orthopedic surgery office with severe, debilitating back, neurogenic claudication, and right lower extremity radiculopathy due to central stenosis. A decompression laminectomy of L3–L5 with bilateral fusion, L3–L5 with posterior segmental instrumentation, and local bone autograft was performed in February 2008 (Figure 1). Following surgery, the patient developed a hematoma under the surgical incision. Of note, the patient takes 81 mg of aspirin daily. Aspirin, as well as rivaroxaban, and clopidogrel have been noted as a potential risk factor in cases of spontaneous spinal epidural hematomas.9,10 She denied any other history of anticoagulation use or coagulopathy. The surgeon attempted to aspirate this mass at a subsequent visit to the office but was unsuccessful. There were no further documented aspiration attempts. The patient was asymptomatic from the mass until she presented to a different neurosurgeon 4 years later due to discomfort from a large posterior lumbar mass. She said it was tender to touch and was having difficulty sleeping due to not being able to lie on her back. On examination at that time, there was a moveable firm mass approximately 5″ deep, 8″ long, and 4″ wide, just deep to the previous surgical incision of the lumbar spine. A normal neurological examination was documented during this visit. Magnetic resonance imaging (MRI) of the lumbar spine showed a large capsulated partially calcified hematoma which was primarily subcutaneous, but superficial to the muscular fascial layer. Due to the significant discomfort that the hematoma was causing, she opted to have this hematoma operatively removed. Plastic surgery was consulted for assistance in closure due to the size of the mass which led to large flaps of thin skin that were difficult to close appropriately. Surgical removal of the hematoma was performed in October 2012. The previous surgical incision was excised and extended with the capsule discovered half an inch deep in the skin. The skin was then dissected away from the right side of the capsular mass. The caudal and cephalad poles were then identified. The caudal aspect of the mass was then incised, and chronic amber fluid was drained which decreased the volume of the mass by about 25%. Then the cephalad aspect of the mass was grasped and dissected from the anterior muscular fascia. The mass was then excised en bloc. The mass was measured at 5″ wide, 8″ long, and 3″ deep following removal. The plastic surgery team arrived at this time to assist in the closure of the wound. There was no further obtainable documentation for follow-up after this operation.
Preoperative X-ray demonstrating prior lumbar fusion.
In November 2022, the patient presented to the emergency department with a complaint of low back pain with radiation into bilateral legs down to the knees. She denied numbness, tingling, or difficulty walking. Exam at that time revealed 5/5 strength L2–S1 on manual motor evaluation with intact sensation. X-rays in the emergency department demonstrated no acute abnormalities. She was discharged with close primary care follow-up where an MRI of the lumbar spine was ordered, and the patient was referred to her index orthopedic surgeon who performed her procedure in 2008. It was noted at this orthopedic appointment that the lumbar mass had reoccurred. The MRI at that time did not demonstrate any evidence of vascular anomaly. The patient had reported a recurrence of her significant tenderness over the dorsal mass. The patient once again had a normal neurological lumbar spine examination at this visit. The patient was then seen a month later after completion of her lumbar spine MRI (Figure 2). She continued to complain of mechanical pain from pressure on her lower back. She also complained of neurogenic claudication with pain radiating into the buttocks and lateral aspect of both legs. The patient expressed increased frustration as pain impaired her ability to stand and walk. MRI demonstrated hypertrophic facet arthropathy, moderate narrowing of a central canal, and moderate to severe narrowing of both neural foramen at L2–L3. The MRI also demonstrated a significant mass in the lumbar spine appearing superficial to the thoracolumbar fascia (Figure 2). The mass did not appear to connect to the dura through the previous surgical site. The surgeon offered aspiration of the mass, but the patient declined as it was unsuccessful in the past. It was recommended to the patient that to treat her neurogenic claudication due to adjacent segment disease at L2–L3, removal of the hardware from L3 to L5 with posterior instrumentation from L2 to L5, revision bilateral laminectomy with medial facetectomies and foraminotomies with excision of large paraspinal mass was warranted. During this revision procedure, a posterolateral fusion procedure was also performed. The patient consented to the procedure described above and the operation was performed in February 2023. The patient’s previous incision was utilized and carried proximally up to the level of L1 and down to the S1 level. Sharp dissection was carried down through the skin and subcutaneous tissue. Just deep to the superficial subcutaneous layer, a large mass was identified. Meticulous dissection was performed around the mass maintaining the integrity of the mass capsule. The mass successfully excised en bloc despite an intraoperative violation of the lateral mass wall. The excised mass was then sent to pathology for evaluation which classified the mass as a chronic calcified hematoma, measuring 14 × 7 × 6.3 cm and weighing 299 g which was a 51% increase in size from the previous hematoma (Figure 3). Postoperative imaging following the revision procedure are seen in Figure 4.

Axial and sagittal MRI demonstrating large paraspinal mass.

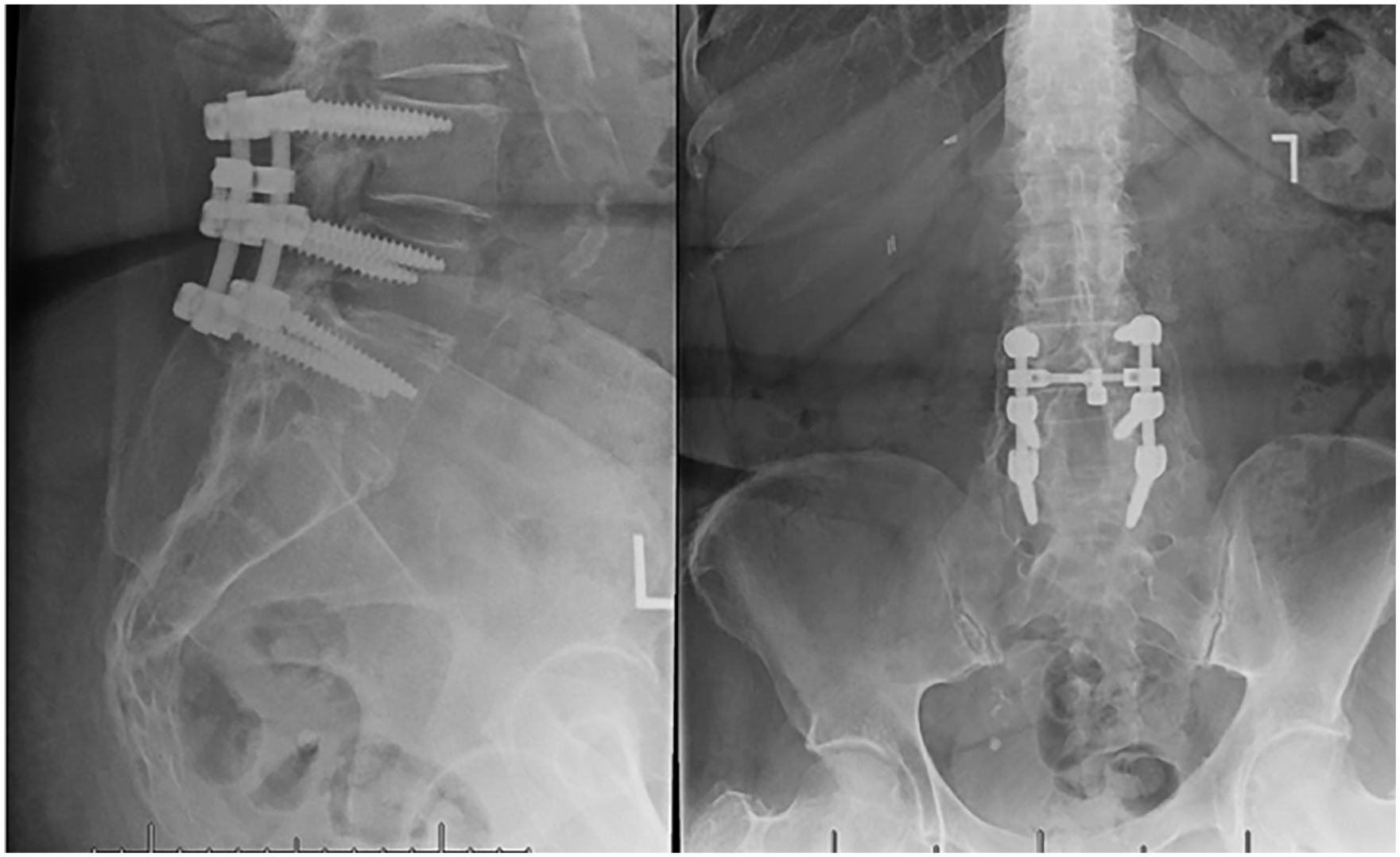
Immediate postoperative X-ray after revision posterior decompression and spinal fusion.

Intraoperative photographs of paraspinal calcified hematoma upon resection.
The patient was seen 2 weeks postoperatively and was doing well. The patient denied radiating lower extremity pain, numbness, or weakness. The patient also stated she had relief from her mechanical symptoms and no longer experienced pain from pressure on her lower back. The patient was then seen again 5 weeks postoperatively and was happy with the results achieved with near full resolution of all her prior symptoms. The patient’s incision was well-healed at that time. Her most recent follow-up was at 1 year, postoperatively where she remains symptom-free and satisfied with her results.
Discussion
Current management of postoperative spinal complications varies greatly and is contingent on the complication. In spinal surgery patients, isolated postoperative wound dehiscence accounts for 0.5%, while the rate of wound dehiscence with co-infection accounts for 2.5%, according to National Surgery Quality Improvement Program data. 11 As previously described, postoperative spinal hematomas have an incidence of 0.4%–0.52%.3–5 Typically, postoperative hematomas are treated through sterile evacuation, ligation of bleeding vessels, and reclosure of the wound. 12 The etiology of postoperative hematomas is thought to originate from sustained capillary bed bleeding at or near the surgical site. 13 Prevention of these masses can be addressed at various stages in the patient’s course of treatment. Preoperatively, it is important to screen patients for a history of coagulopathy and to hold the use of anti-platelet or anti-coagulant drugs. Intraoperatively, adequate surgical hemostasis is crucial. This can be accomplished by utilizing tissue sealants, platelet gels, and quilting sutures intraoperatively. Postoperatively, a hemovac drain can be placed to avoid the accumulation of hematoma. 13 To our knowledge, there are no previous reports of a calcified intermuscular hematoma in spine literature. However, Zelmanovich et al. reported an ossified intramuscular hematoma in the erector spinae muscles in 2023, which developed following trauma 15 years prior to its removal. 14 Pathology confirmed that the hematoma was ossified. Similarly to our outcome, they successfully removed the hematoma and primarily closed the wound, leading to the resolution of symptoms without wound-healing complications.
Conventional open approaches in lumbar spine surgery have been associated with prolonged hospital stays, increased perioperative blood loss, and higher infection rates compared to minimally invasive surgery (MIS). 15 Open spine procedures cause increased morbidity due to muscular crush injury from retractor placement, disruption of paraspinal muscle attachments to the spinous processes, and larger surgical corridors compared to MIS techniques.16,17 In addition, open lumbar surgery may lead to paraspinal muscle atrophy possibly due to denervation and direct muscle trauma during surgery, resulting in poorer postoperative outcomes. 18 Another complication after open lumbar surgery includes surgical site infection. This complication is a significant cause of readmission after lumbar spine surgery, contributing to increased morbidity, mortality, and healthcare costs.19–22 O’Toole et al. reported a significantly higher incidence of wound infections with open lumbar surgery when compared to MIS, with some studies reporting up to 10 times greater. 23
To reduce hematoma occurrence, wound dehiscence, and surgical site complications, there has been an emphasis on the standardization of a layered wound closure which has included separating fascial layers, preventing stitch abscesses, and creating a tension-free wound closure.24,25 Inadequate fascial closure causes adverse wound reactions, such as hematoma and oozing, and increases the risk of deep infections. 26 We believe in this unique case, the patient may have had incomplete resolution of the initial hematoma or inadequate deep wound healing. Therefore, it is crucial that surgeons are aware of techniques to ensure proper wound healing. Another aspect of wound closure that has been studied is the spacing of stitches. It was found that stitches too close together may also compromise integumentary blood supply between sutures and cause tissue strangulation. 27 The management of the chronic calcified hematoma in our case involved surgical removal of the mass followed by multilayer closure, resulting in the resolution of symptoms without recurrence. As this appears to be the first reported case of intramuscular calcified spinal hematoma, we present this case report as an illustrative example of a potential treatment option for such cases.
Conclusion
Though it has been documented that postoperative wound complications, including hematomas, are not uncommon in spinal surgery, the occurrence of postoperative calcified chronic symptomatic paraspinal masses has yet to be documented. Notably, this patient had a recurrence of her mass, with approximately a 51% increase in size, despite initial aspiration and subsequent surgical excision without acute complications. This case presents itself with a unique finding that is not well documented and may allow the orthopedic and neurosurgical community to be aware of such complications, and effectively manage them. Furthermore, we may be able to utilize current literature regarding the prevention of postoperative hematomas to decrease the incidence of the aforementioned complication.
Footnotes
Acknowledgements
There are no other acknowledgments to this paper as all who have contributed are listed as authors.
Author’s contributions
Timothy Edwards: contributed to the paper through Conception, Design, Literature review, Writer, and Critical review.
Shaan Sadhwani: contributed to the paper through Conception, Design, Literature review, Writer, Critical review.
Brendan Sweeney: contributed to the paper through Conception, Design, Literature review, Writer, Critical review.
Antonio Almeda-Lopez: contributed to the paper through, Literature review, Writer.
Walter C Peppelman: contributed to the paper through Supervision, Critical review.
William J Beutler: contributed to the paper through Supervision, Critical review.
Data availability
Data sharing is not applicable to this article as no new data were created or analyzed in this study. This case was presented at Philadelphia College of Osteopathic Medicine’s Research Day on May 1, 2024, as a poster presentation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This report has been approved by our institution’s institutional review board. Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.