
Abstract
Granulomatosis with polyangiitis, a type of small-medium vessel vasculitis, can pose diagnostic challenges due to its diverse clinical manifestations. We present a case that mimicked multisystem pyoderma gangrenosum with cutaneous ulceration, renal sparing, and antineutrophil cytoplasmic antibody negativity. Although antineutrophil cytoplasmic antibody is positive in approximately 90% of cases of granulomatosis with polyangiitis, its negativity should not exclude the diagnosis. Additionally, pyoderma gangrenosum-like cutaneous ulcers should prompt consideration of granulomatosis with polyangiitis, especially in the context of multisystem disease presentation. This case underscores the importance of maintaining a high suspicion for granulomatosis with polyangiitis in patients presenting with cutaneous ulceration and respiratory tract disease.
Introduction
Granulomatosis with polyangiitis (GPA), formerly known as Wegener’s granulomatosis, is the most common type of antineutrophilic cytoplasmic antibody (ANCA)-associated vasculitis, affecting 10–20 individuals per one million worldwide annually. 1 The peak incidence of GPA occurs between the ages of 64 and 75. Characterized by a wide range of presentations that can involve various organ systems (Table 1), 2 GPA is associated with significant morbidity and mortality. 1 The life expectancy for individuals with untreated GPA is, on average, 5 months; however, remission can be achieved in more than 90% of patients with appropriate treatment. 2 Treatment of GPA involves immunosuppressive agents such as corticosteroids, cyclophosphamide, rituximab, methotrexate, azathioprine, and plasmapheresis. 1 Given its significant morbidity and mortality, timely diagnosis and management is imperative. We present a case of suspected ANCA-negative GPA that mimicked multisystem pyoderma gangrenosum (PG). This case highlights features of GPA to assist in future diagnoses, particularly when associated with ANCA-negativity or PG-like cutaneous lesions.
Clinical features of GPA.
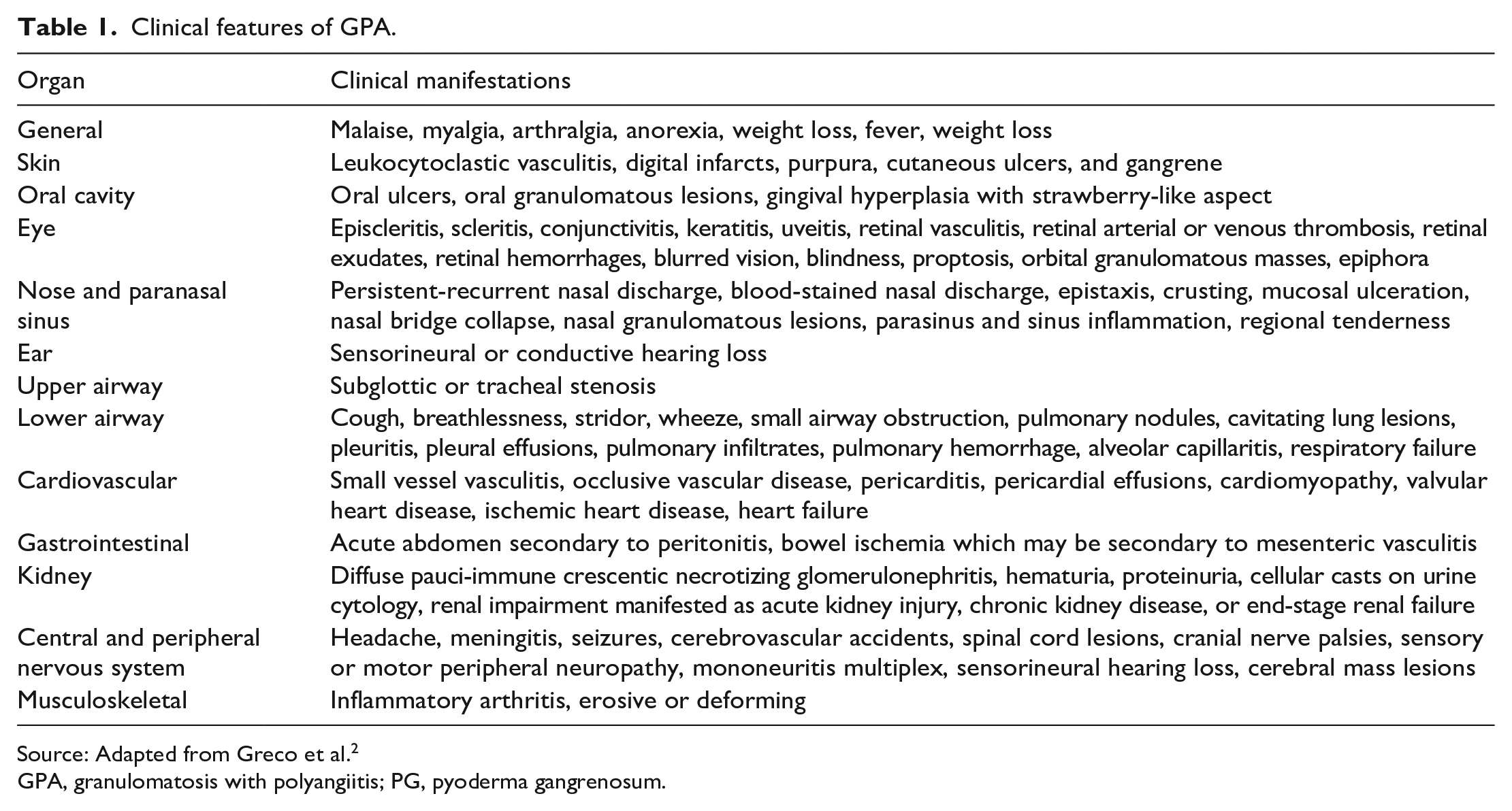
Source: Adapted from Greco et al. 2
GPA, granulomatosis with polyangiitis; PG, pyoderma gangrenosum.
Case report
A 58-year-old male with a past medical history of intranasal cocaine use, chronic sinusitis, and epistaxis was being investigated by respirology for cavitary lung lesions with radiologic progression despite antibiotics. Autoimmune workup was negative, including ANCA. Lung core biopsy #1 was taken (Table 2), leading to a potential diagnosis of organizing pneumonia. Prednisone 0.625 mg/kg daily was started, resulting in a significant decrease in the size of the lung lesions on computed tomography (CT).
Overview of pathology results.

GPA, granulomatosis with polyangiitis.
One month later, during a prednisone taper, the patient developed painful bilateral lower extremity cutaneous ulcerations. Physical exam revealed multiple well-demarcated ulcers with raised, violaceous borders. Repeat autoimmune workup was negative. Dermatology was consulted and diagnosed cutaneous PG. A skin biopsy was not performed at this time due to concern of pathergy. The ulcers responded well to prednisone 0.75 mg/kg daily and topical clobetasol ointment 0.05% with dressing changes.
A connection between the cutaneous PG-like lesions and lung nodules was considered. The patient did not have any signs or symptoms of inflammatory bowel disease, arthritis, or other autoimmune connective tissue diseases. The possibility of malignancy was also considered. Before further workup could be performed, his ulcers worsened during a prednisone taper, and he was admitted to the hospital for pain control.
While in the hospital, he was seen by dermatology, otolaryngology, respirology, hematology, rheumatology, and infectious diseases. A cutaneous ulcer biopsy showed features consistent with PG with no evidence of vasculitis (Table 2). Serum protein electrophoresis and eosinophil levels were normal. Head CT showed opacification of the right maxillary sinus with loss of the medial sinus wall and a large midline septal defect. Nasal mucosa biopsy #1 and lung core biopsy #2 were performed (Table 2). Given the lack of diagnostic clarity, lung wedge resections were taken (Table 2). The findings were signed as consistent with PG given the clinical suspicion of the same in his skin. The patient was diagnosed with multisystem PG and was started on cyclosporine 5 mg/kg daily, which resulted in a temporary improvement of his cutaneous ulcers (Figure 1). Infliximab 5 mg/kg every 6 weeks was subsequently initiated which resulted in dramatic ulcer healing (Figure 2).

Lower extremity ulcers following treatment with prednisone and cyclosporine, prior to initiation of infliximab.

Lower extremity ulcers after treatment with prednisone, cyclosporine, and infliximab.
In the year following discharge from the hospital, his ulcers worsened, and he developed sinus pain, progressive proptosis, and painful periocular swelling. Nasal mucosa biopsy #2 and palate biopsy #1 were taken (Table 2). Repeat ANCA was negative. Head CT showed right-sided pansinusitis and new destruction of the orbital floor and hard palate. Periocular discharge was drained and cultured, showing an abundance of neutrophils and no infection. Prednisone 1 mg/kg daily and infliximab 10 mg/kg every 4 weeks resulted in rapid improvements in his facial pain, proptosis, and periocular swelling. Given the bony necrosis and respiratory tract involvement, the patient was diagnosed with ANCA-negative GPA with PG-like cutaneous changes. The patient subsequently expired unexpectedly at home. An autopsy was declined by the family.
Discussion
We present a case of ANCA-negative GPA with renal sparing and PG-like cutaneous ulcers that mimicked multisystem PG. In GPA, up to 90% of cases are positive for ANCA. 2 Given this, it is imperative that physicians consider GPA in patients with multisystem inflammation or vasculitis, even in the context of a negative ANCA. Diagnosing ANCA-negative GPA can be further complicated when classic findings such as renal involvement are absent.
Renal sparing is often seen in patients with GPA, particularly early in the disease course or when ANCA is negative.1,3 The classic triad seen in GPA includes involvement of the upper respiratory tract, lower respiratory tract, and kidneys. 1 Although 80% of patients have renal involvement within 2 years of disease onset, only 10%–20% have renal involvement at the time of presentation. 1 Additionally, ANCA is negative in an estimated 40% of active, renal-sparing diseases. 3 Similarly to renal involvement, other features of GPA are often absent on workup.
Histological findings of GPA can be absent. The histological findings in GPA include vasculitis, granulomas, and giant cells. 4 In GPA, vasculitis and granulomatous inflammation may only be seen in 21% of head and neck biopsies. 5 Further, only 47% of nasal biopsies in GPA reveal scattered giant cells. In the case presented, multiple biopsies were nonspecific and lacked features classic for GPA. GPA exhibits variable histological findings, and its clinical presentation, including cutaneous manifestations, can also vary significantly.
GPA can present with cutaneous changes, including PG-like ulcers. Although up to 50% of cases of GPA are found to have cutaneous involvement, 1 PG-like ulcers are a rare manifestation.6,7 PG is a rare neutrophilic inflammatory condition that classically presents as painful cutaneous pustules or nodules that evolve into ulcers with purulent drainage and violaceous, undermined borders. 8 Extracutaneous manifestations of PG can also be seen, with pulmonary involvement being the most common. 9 Similarly to GPA, there is a lack of gold standard diagnostic tests for PG. 9 Findings of PG on histopathology are often nonspecific, with neutrophilic inflammation being the most common. It can thus be difficult to differentiate between multisystem PG and GPA with skin and pulmonary involvement.
In summary, diagnosing GPA can pose significant challenges, particularly when ANCA is negative. It is crucial for physicians to consider GPA when ANCA is negative, even if other typical features such as kidney involvement and histologic findings are absent. Additionally, GPA should be considered in patients presenting with PG-like ulcers, particularly when accompanied by inflammation or vasculitis affecting other systems.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Informed verbal consent was obtained from the patient to share the case and photographs.