
Abstract
Diagnosis of fluoroscopy-induced radiodermatitis remains challenging for dermatologists. We present a case report where a patient had predictable risks of developing chronic radiodermatitis, yet the diagnostic was delayed for over a year and a half. In the current absence of appropriate follow-ups in some institutions, dermatologists should keep high suspicion for chronic fluoroscopy-induced radiodermatitis when encountering lesions characteristic of radiation dermatitis without a history of radiotherapy, prompting the necessity to inquire about antecedents of fluoroscopy-guided interventions.
Keywords
Introduction
Radiodermatitis in the context of radiotherapy isn’t new for clinicians. However, they need to recognize the role of fluoroscopy in this pathology. Fluoroscopy-induced radiodermatitis (FIRD) is underreported and its incidence is increasing due to the growing use of fluoroscopy for procedures that are more complex and lengthier. 1 Furthermore, FIRD are more often reported in radiology and cardiology journals than in dermatology literature. 2 In addition, patients tend to consult dermatologists instead of the clinician who performed the fluoroscopy-guided interventions (FGIs). 1 It highlights the need to raise awareness among dermatologists.
Case report
A 70-year-old white woman presented in June 2021 with an erythematous and pruritic plaque on her left flank. Her medical history included rheumatoid arthritis (inactive for decades), atherosclerotic disease, and metabolic syndrome (body mass index of 34.06). She reported no radiation exposure. At first, her wound was misdiagnosed as cellulitis and dermatitis, which were treated without success. The lesion evolved into a purpuric retiform infiltrated patch about a year later. Ulceration started in March 2022 and worsened.
Moreover, the patient’s wound had debilitating impacts. She reported a very pruritic wound, which eventually became painful, partially relieved with Pregabalin and Hydromorphone. In addition, she experienced sleep issues and feelings of desperation.
To eliminate angiosarcoma, three punch biopsies were performed through June/July 2022. The samples likely contributed to the spreading of the ulceration as demonstrated in Figure 1. Moreover, histological analyses were consistent with small and medium vessel vasculitis. Radiation injury was mentioned, but less likely because of the vasculitic changes.

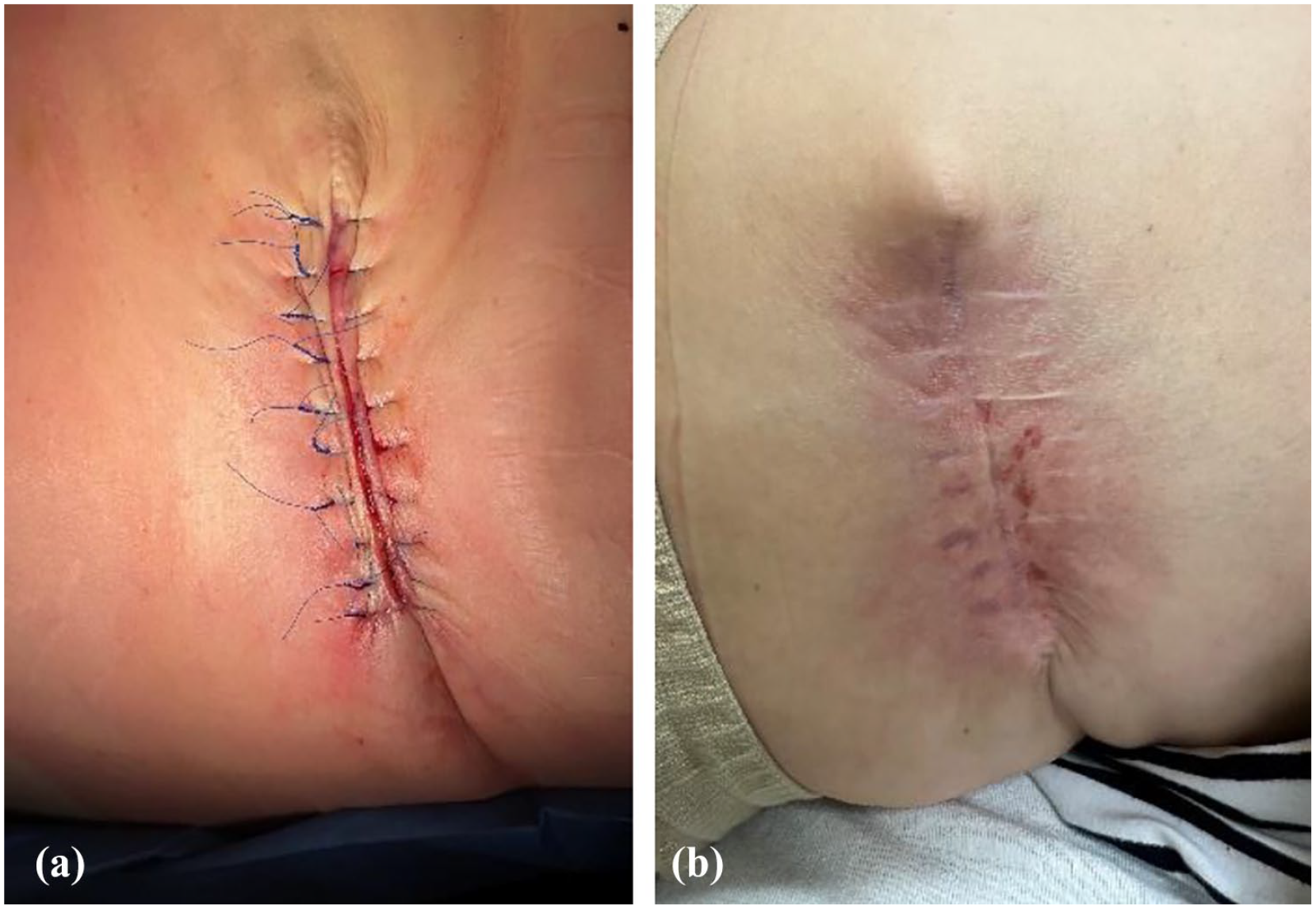
(a) Shows chronic FIRD before biopsies. Note erythematous border with central ulceration. (b) After punch biopsies: worsening of the ulcer with a reduction in redness.
The patient’s wound care was unsuccessful, and the ulcer required surgery in January 2023 (see Figure 2). As of July 2023, the patient reports a complete recovery with a well-healing scar (see Figure 3).

Opening of the wound showing removal of the affected tissue during the surgery in January 2023. Muscles are showing.
(a) Recently closed wound in January 2023. (b) Healed wound 7 months later.
FIRD was diagnosed in January 2023 with the histological analysis of the specimen removed during the surgery. The patient’s wound was explained based on a former abdominal angioplasty. In June 2021, the patient underwent angioplasty of the superior mesenteric artery, through femoral approach, to relieve pain from chronic mesenteric ischemia. The intervention was complicated as the aortic route was obstructed by calcification. The catheter was therefore inserted antegrade via the hepatic artery toward the gastroduodenal artery to reach the superior mesenteric artery retrograde. The intervention achieved with Digital Subtraction Angiography (DSA) was successful but prolonged with a fluoroscopic time of 2 h 34 min, a dose-area-product of 1278 Gy cm2, and a total dose at the reference point of 14.95 Gy.
Discussion
The consequences of X-rays are classified into deterministic and stochastic effects. Stochastic effects notably include secondary cancers. No threshold is safe, but the higher the dose, the more elevated the risk is. 3 At least one poorly differentiated squamous cell carcinoma was reported in 2019. 4 The cancer emerged years later at the site of a chronic radiodermatitis, 4 raising thoughts about long-term follow-ups.
Deterministic effects are based on well-defined thresholds. For instance, chronic FIRD appears when radiation doses exceed 10 Gy. 5 Threshold doses for follow-ups are described in the literature. 3 Doses are detailed in Table 1. The radiation doses recorded in the case report exceeded the recommended follow-up thresholds.
Suggested thresholds for follow-up.

Source: Data are coming from Balter and Patel. 3
In addition, certain characteristics elevate the risk for the patients, requiring clinical judgment. These risk factors, mostly described in the context of radiation therapy, include smoking status, collagen diseases, chemotherapy, hyperthyroidism, fair skin, and others.1,3 Obesity has been identified as a significant predictor of increased radiation exposure in FGIs. 1
Technical parameters are the most easily modifiable factors influencing radiation dose. These include pulsed fluoroscopy, collimation, and low-dose imaging protocols. 6 For instance, in the case report, DSA increased the radiation dose compared to standard fluoroscopy. 6 Also, the beam remained localized on the patient’s flank for a long time, which contributed to the overall risk of FIRD.
Chronic FIRD can take months to years to develop, 5 and the history of FGIs might not always be evident in the patient’s medical records. 1 Additionally, radiation dermatitis is primarily diagnosed based on clinical evaluation. More concretely, physicians should be alerted to FIRD when observing an association between the lesion’s location, shape, and history of FGIs.5,7 A demarcated lesion with distinct square borders is described as a pathognomonic sign of a fluoroscopy-related injury. 3
Biopsies are mainly performed when the diagnosis is uncertain, as in the case of our patient. However, histological changes are not pathognomonic of chronic FIRD. 5 In addition, biopsies may worsen the lesion by acting like pathergy, as exemplified in the case report. Therefore, biopsies are not recommended unless cancer or deep infections are suspected. 7 Moreover, in the case report, biopsies were misleading, as vasculitis is not typically a diagnosis confused with radiodermatitis.
In the case report, the patient had a predictable risk of developing chronic FIRD based on the recommended thresholds for follow-ups, beam placement, and her risk factors (fair skin, obesity, and rheumatoid arthritis). Similar cases have occurred in our hospital, underscoring the importance of follow-ups, as established in other institutions 8 Implementing clinical follow-up protocols should involve dermatologists as there are no evidence-based guidelines for treatments of FIRD. These follow-ups should also include patient education on lesion care, as various traumas can stimulate ulceration in chronic radiodermatitis. 7
To conclude, in the current absence of appropriate follow-ups in some institutions, dermatologists should keep high suspicion for chronic FIRD when encountering lesions characteristic of radiation dermatitis without a history of radiotherapy, prompting the necessity to inquire about antecedents of FGIs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The authors obtained written consent from patients for their photographs and medical information to be published in print and online with the understanding that this information may be publicly available.