
Abstract
Pemphigus foliaceus is a superficial autoimmune blistering disorder of the skin. Localized forms of pemphigus foliaceus are rare. Only a few cases have been described. We report a case of an 81-year-old man with pemphigus foliaceus who initially presented with localized dermatomal facial lesions. Due to this atypical presentation, making the diagnosis was challenging. To our knowledge, this is the first case of localized pemphigus foliaceus with a dermatomal distribution to be recorded.
Introduction
Pemphigus foliaceus is a superficial autoimmune blistering disease caused by immunoglobulin G (IgG) autoantibodies against desmoglein-1 (Dsg-1), a protein implicated in epidermal cell–cell adhesion and expressed mostly in the superficial layers of the epidermis. 1 Cutaneous lesions typically present as erosions in a seborrheic distribution. 2 Mucosal lesions are rare. Localized cases are infrequent and diagnosis is often delayed. 3 We describe the case of an 81-year-old man with initially localized facial pemphigus foliaceus presenting in a dermatomal distribution. This presentation is atypical and was never described before.
Case report
An 81-year-old male was referred to the Dermatology clinic in May 2023 for a 1-month-old erythematosquamous non-infiltrated plaque on the right temple. The lesion was not responsive to low-potency topical corticosteroids. Past medical history was significant for diabetes, hypertension, dyslipidemia, and benign prostatic hyperplasia. The patient’s medication list was as follows: Saxagliptin, gliclazide, metformin, dapaglifozin, propranolol, amlodipine, perindopril-erbumine, rosuvastatin, domperidone, Tamsulosin, dutasteride, and vitamin B12. The patient had no history of skin cancers. The remainder of the skin exam was unremarkable. An incisional shave biopsy was done. The histopathologic report showed parakeratosis, acanthosis, and spongiosis of the epidermis. No atypias or signs of squamous cell carcinoma (SCC) were noted.
In September 2023, the lesion had expanded and was now occupying the right temple and part of the right cheek (Figure 1). Important pruritus was present. The patient had been applying bacitracin ointment occasionally on the lesion with no improvement. He visited the emergency department and received cefadroxil, diphenhydramine, and fucidic acid ointment with little improvement. No evidence of cellulitis was noted and an allergic contact dermatitis to bacitracin was suspected. Hydrocortisone valerate cream was prescribed.

Erythematosquamous plaque on the right temple and cheek in September 2023.
At follow-up 2 weeks later, progression of the lesion was noted, now adopting a strikingly dermatomal distribution mainly in V2 territory (Figures 2 and 3). New lesions were visible on both sides of the nose. No vesicles, bullae, erosions, or crusts were noted. A skin culture, a Polymerase Chain Reaction (PCR) test for HSV-1/HSV-2/VZV and 2 incisional punch biopsies were made (right cheek and left nose). The patient had no history of herpes simplex virus (HSV) or varicella zoster virus (VZV). Valacyclovir and cefadroxil were prescribed. The skin culture and PCR came back negative. Moderate potency topical corticosteroid and wet compresses were initiated.

Progression of the erythematosquamous plaque in a dermatomal distribution (V2–V3). Note the sparing of the superior eyelid and the lesion on the nose.

Erythematosquamous papules on the nose.
The histopathologic report showed small foci of acantholysis in a follicular infundibulum on the right cheek and possible ancantholysis and dyskeratosis on the nose, raising the possibility of pemphigus foliaceus. Anti-basement membrane and anti-intercellular substance antibody titers were tested in the serum and came back negative.
One month later, the lesion on the right cheek had greatly improved with treatment. However, new lesions had appeared on the left cheek and ear which the patient had not treated. A biopsy and a perilesional direct immunofluorescence (DIF) were obtained. The DIF showed intercellular deposition of IgG and C3 in the epidermis. The pathology showed peeling of the stratum corneum and granulosum. Those findings were compatible with pemphigus foliaceus. Doxycycline was initiated at 100 mg daily and topical treatment was changed for a low potency corticosteroid.
Because of partial amelioration, doxycycline was rapidly increased to 100 mg twice daily. The lesions were solely on the face initially. Around 20 asymptomatic erythematosquamous papules and plaques eventually developed on the trunk (Figure 4) and extremities. Moderate potency topical corticosteroid was prescribed for those lesions with good response on subsequent follow-up.
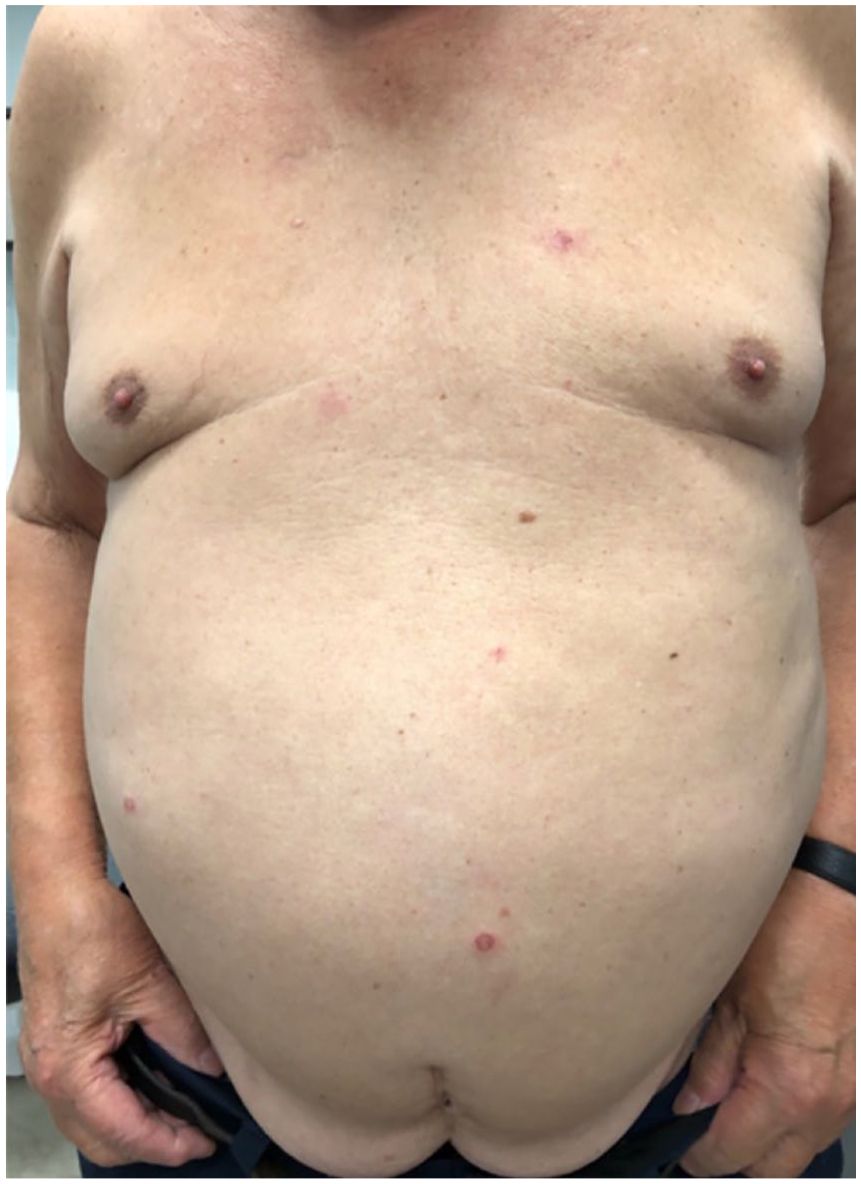
Erythematosquamous papules and plaques on the trunk.
In January 2024, the plaque on the right cheek was 40% better, and five erythematosquamous papules were left on the trunk and arms. The patient was satisfied with the treatment regimen, so it remained unchanged. Further treatment will be considered upon evolution and follow-up with the patient in the next months.
Discussion
To our knowledge, this is the first case of localized pemphigus foliaceus presenting in a dermatomal distribution.
Localized pemphigus foliaceus is rare. Only 15 cases were described in the literature.1–4 Most of them happen in middle-aged patients. Men are as affected as women.1–4 No trigger was identified in our case as in the majority of other cases described. In fact, only two cases had presumed triggers (imiquimod 5% cream and small trauma). 1 In our case, the diagnosis was made in under a year, but it usually takes longer to be established.1,3–5
All reported cases, including ours, arose on the face in one or multiple locations (eight on the nose, six on the right cheek, two on the right temple, two on the left side of the face, two on the left ear, and one on the scalp).1–5 Some authors suggest that ultraviolet rays could enhance the binding of anti-Dsg1 antibodies to the epidermis and activate inflammatory mediators, explaining why localized pemphigus foliaceus is mainly on the face. 4 The nose and the rest of the face are also prone to trauma and friction, which could induce blistering even with low titers of autoantibodies. 5
Localized pemphigus foliaceus usually does not disseminate on the body. Only our case and three others did. 1 Due to the small number of cases reported, it is not possible to identify risk factors of dissemination in initially localized pemphigus foliaceus.
In all the cases, the DIF was positive and compatible with pemphigus foliaceus meaning this test should be done if we suspect the diagnosis. As for pathology, subcorneal blister and acantholysis were often present.1,4 In our second biopsy, acantholysis in the follicular infundibulum was identified. This finding was present in two other cases of localized pemphigus foliaceus. 1 Ohata et al. 3 suggested that it could be an early sign of the disease. It should not be overlooked, as it could allow a more rapid diagnosis, and early treatment could prevent the dissemination of the disease.
It is hard to explain the dermatomal presentation of our case. A number of unrelated dermatoses, like bullous pemphigoid, were described to occur in sites of healed herpes zoster or herpes simplex. 6 This phenomenon is called Wolf isotopic response. However, pemphigus foliaceus was never described in this phenomenon and our patient did not have a history of HSV or VZV at the localization of the lesions. Two cases of linear IgA bullous dermatosis with a zosteriform distribution without a prior history of VZV were described in the literature. 7 We can hypothesize that autoimmune bullous diseases can rarely present in a dermatomal distribution outside of the Wolf isotopic response. The exact pathophysiology remains unknown.
This case demonstrates the importance of adding localized pemphigus foliaceus in our differential diagnosis of an erythematosquamous eruption of the face, even in a dermatomal distribution. It is a rare condition and diagnosis is often delayed, which is why a high degree of suspicion should be kept. If localized pemphigus foliaceus is suspected, a biopsy (with attention to the follicular infundibulum) and DIF should be done.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written consent was obtained from the patient for the images to be included in the article.