
Abstract
We performed detailed structural analysis of a case of a unilateral lesion of the inferior colliculus using magnetic resonance microscopy on a 7 T system. A 36-year-old right-handed man had an intracerebral hemorrhage circumscribed to the right inferior colliculus. Following recovery from the acute phase, he had only residual left ear tinnitus and left trochlear palsy and no hearing loss. Microscopic imaging analysis on a 7 T magnetic resonance imaging system demonstrated a chronic lesion confined primarily to the right central nucleus of the inferior colliculus. Sound localization was significantly impaired in the contralateral hemispace. The case confirms prior clinical reports of unilateral inferior colliculus dysfunction, the specific anatomic characterization of which was demonstrated in this case by magnetic resonance microscopy. It furthermore supports the notion that central nucleus of the inferior colliculus dysfunction can produce tinnitus and sound localization deficits, without hearing loss
Keywords
Introduction
Animal studies indicate that the central nucleus of the inferior colliculus (CIC) is capable of producing tinnitus.1–4 It has also been consistently demonstrated that intact inferior colliculus (IC) function is essential for sound localization.5,6 Case studies of patients with mesencephalic abnormalities demonstrated various audiological abnormalities, indicating that lesions in IC can cause tinnitus and sound localization deficit in humans as well.7–10 We present here a case of IC syndrome, and the detailed neuroanatomic analysis was confirmed using in vivo microscopic imaging on a 7-T magnetic resonance imaging (MRI) system.
Case report
A 36-year-old right-handed man experienced sudden occipital headaches, diplopia, tinnitus, nausea, vomiting, and left facial numbness. Neurological examination disclosed left trochlear palsy, bilateral gaze-evoked nystagmus, buzzing in the left ear, and hemihypesthesia and hemihypalgesia on the left side of the body and face. Imaging revealed a small intracerebral hemorrhage in the right midbrain tegmentum, including the right IC, and blood in the subarachnoid and intraventricular spaces. A month after the acute event, he had residual left ear tinnitus and left trochlear palsy. He was referred to the Center for Integrated Human Brain Science of University of Niigata for further testing of his apparent CIC dysfunction.
High-resolution (156 × 156 μm) MRI images were obtained using a General Electric Signa Excite 7T research system equipped with a 900 mm bore superconductive magnet and maximum gradient strength of 32 mT/m.11,12 Single 5-mm-thick slices were obtained using fast spin echo (FSE) sequencing with peripheral gating. The main parameters were repetition time, five cardiac cycles; echo time, 19.5 ms; trigger delay, 300 ms; field of view, 8 × 8 cm; matrix size, 512 × 256; NEX, 2; and echo train length, eight. Representative images are shown in Figure 1. Corresponding schematic figures are shown in Figure 2. Anatomical analysis clearly demonstrated that the main damage involved the right CIC as well as pre-decussation fibers of the trochlear nerve.
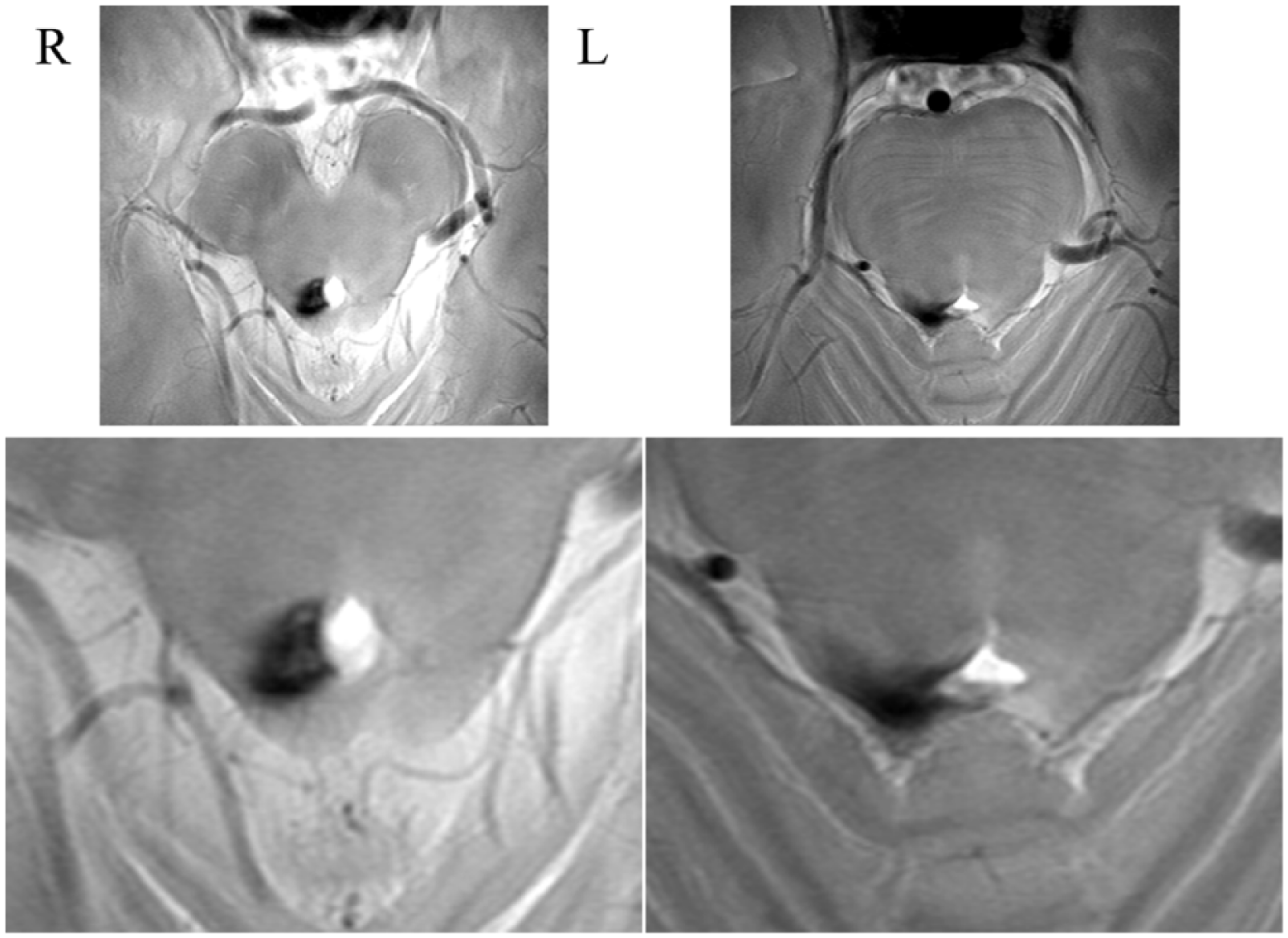
High-resolution images on 7 T MRI. (Upper) Original slice images and (lower) affected region enlarged.
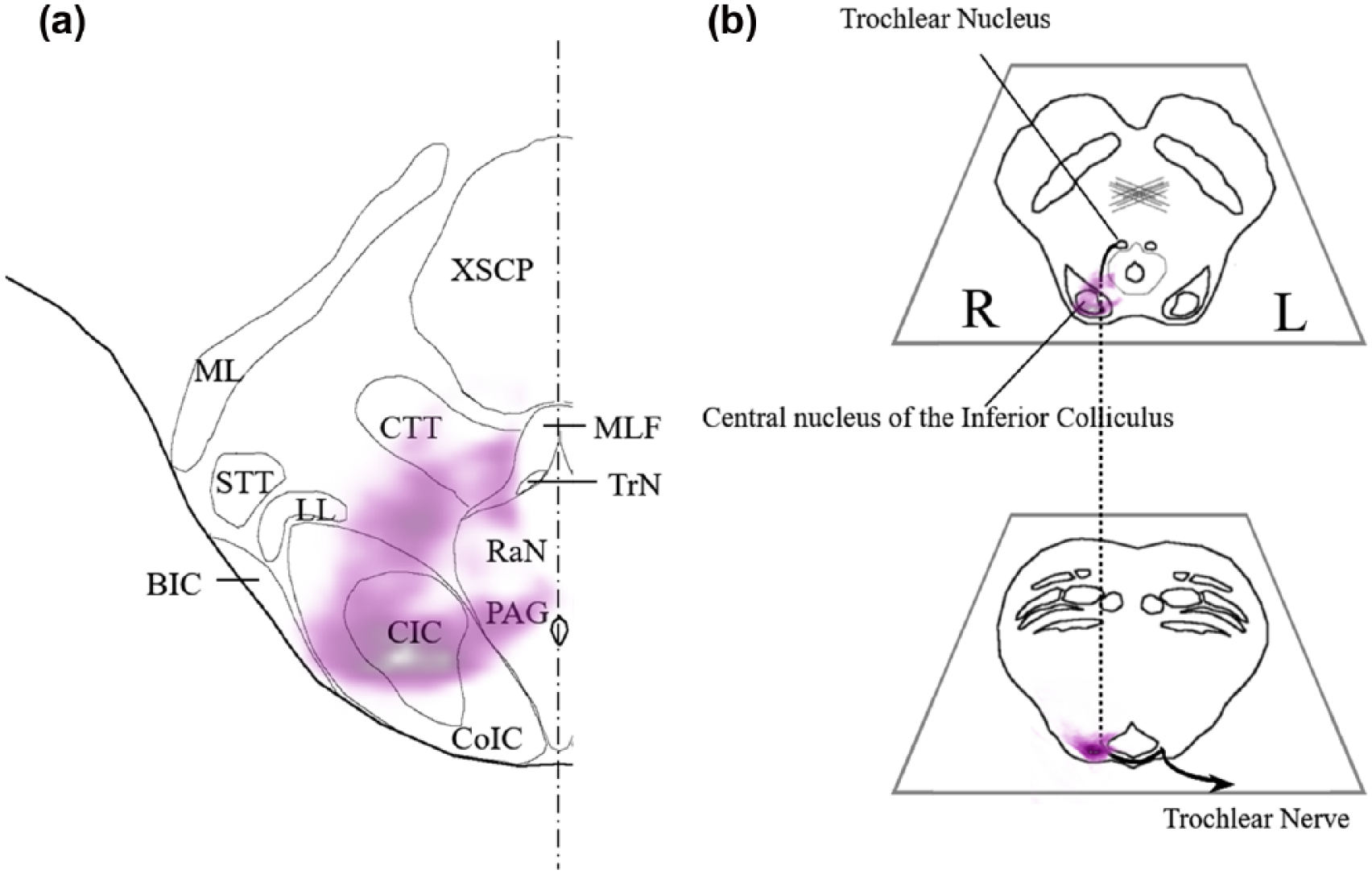
Schematic representation of anatomical structures. Light purple area represents lesions determined using 7T MRI shown in Figure 2. (a) Midbrain slice showing CIC lesion and (b) midbrain and upper pontine slices showing pre-crossing left trochlear nerve involvement.
Pure tone audiogram was completely normal as was speech audiometry. Auditory brainstem response (ABR) on left ear stimulation showed a poorly formed wave V, with prolongation (0.2 ms) of the latency compared to right ear stimulation. Bekesy audiometry showed a Jerger type IV abnormality on 2000Hz stimulation of the left ear indicating auditory fatigue. 14
Sound localization analysis was conducted inside a sound chamber. Loudspeakers were placed at 0°, ± 45°, and ± 90° azimuth. Target sounds were sinusoidal tones (350 ms duration, 100 ms fall-time, 44.1 kHz sampling rate, and 16-bit resolution), tuned to A4 (440 Hz), and generated by STIM hardware and software (Neuroscan). 15 Sounds were presented randomly at a comfortable listening level (approximately 65 dB sensation level (SL)) through one of the five loudspeakers at a rate of one per second, for a total of 250 target sounds (50 each for each azimuth) per session. The patient completed three sessions with 10 min rest between sessions. He was instructed to point to the loudspeaker he believed emanated the sound using a laser pointer. Figure 3 shows the results as error rate. The patient exhibited significant error rates in this sound localization task for left 45° (76%) and 90° (36%) azimuth directions compared to right azimuth directions (less than 1%).

Results of sound localization study. (% indicates % errors exhibited by the patient.)
Discussion
The present case provided a unique opportunity for identifying the specific neuroanatomic correlate of clinical deficits associated with a lesion within the IC. In the chronic state, the patient exhibited subjective symptoms of left ear tinnitus and double vision, while the neurological exam showed left trochlear palsy. Electrophysiological studies demonstrated a Jerger Type IV abnormality on Bekesy audiometry and abnormalities of wave V on ABR associated with left ear stimulation. In addition, the patient exhibited clear cut abnormalities in sound localization in the left extrapersonal space.
Although the primary cause of chronic tinnitus is believed to be related to cochlear dysfunction, it is now generally accepted that alteration of functionality in the central auditory system also plays a role in the pathogenesis of chronic tinnitus. Recent studies implicate that the IC, especially the CIC, an essential relay nucleus in the ascending auditory pathways, can play a role in generating chronic tinnitus.1,2 Stimmer et al. 10 reported a similar case of IC hemorrhage with contralateral monaural tinnitus. The present neuroanatomical analysis case further supports this concept. The patient had no hearing deficit. In vivo microscopic anatomical studies all indicate that the lesion is likely to be confined to the region of the right CIC. Tinnitus started at the onset of the disease process and continued after neighborhood symptoms, such as nausea/vomiting, diplopia, and sensory loss, had subsided. The cause of the tinnitus in this case can be attributed to dysfunction of the contralateral CIC.
Sound localization is believed to be crucially dependent on functionalities of the dorsal cochlear nucleus (DCN).3,4 As shown in animal studies, CIC plays a critical role in integrating neural processes necessary for sound localization in the contralateral extrapersonal hemispace.5,6 Litovsky et al. 9 reported a case of dorsal midbrain hemorrhage including IC with sound localization deficits in the contralateral hemispace. The current case afforded detailed clinical neuroanatomic delineation, further supporting that a lesion of the IC, especially that of CIC, is responsible for the sound localization abnormalities experienced by the patient.
Conclusion
We present a case of a unilateral lesion of the right IC manifesting clinically with chronic tinnitus in the contralateral ear and deficits in sound localization in the contralateral hemispace, without attendant hearing loss. Detailed anatomical investigation using 7 T MRI micro-imaging demonstrated that the lesion is confined primarily to the CIC supporting prior clinical cases and animal studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in this case report involving human participants were in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animal performed by any of the authors. Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants from the Ministry of Education, Culture, Sports, Science, and Technology (Japan).
Informed consent
Written informed consent was obtained from the patient for publication of this case report. Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.