
Abstract
Enterocutaneous fistula is a dreaded complication by most surgeons especially after emergency abdominal surgery. It can also occur spontaneously from an underlying disease. The pathology is demanding both mentally and physically and causes medical and nursing problems for the affected individual. In this case report we present a timeline of a young 4-year-old boy who sustained penetrating abdominal-perineal injury from a fall and later presented with peritonitis. His condition progressed to complicate into enterocutaneous fistula and succumbed unfortunately due to multifactorial reasons. This shows the impact and burden of the disease pathology not only on patients but also on the medical system as a whole.
Introduction
The management of enterocutaneous fistula (ECF) has always been a challenge to surgeons globally because of its associated complications like malnutrition, prolonged hospital stay, and electrolyte imbalances. 1 Management of ECF is complex and requires a multidisciplinary approach, however, the general principles of management of ECF have remained the same which include infection control, wound care, nutritional and psychological support, and timed surgery.1,2 ECF is globally associated with substantial morbidity and mortality; Fischer et al. report mortality rates between 7% and 20% in non-trauma patients.1,2 The authors found that those with open abdomen had a higher risk of ECF (8% vs 0.5%) and lower rate of spontaneous closure (37% vs 45%) and in their results, the mortality rate of ECF was 14%. 1 There are many causes of ECF and can be classified as infective such as Tuberculosis, malignancy like gastrointestinal cancers, inflammatory like Crohn’s disease, and trauma for example from abdominal surgery or penetrating injury. 2
The challenges faced to manage ECF are considerably high in resource-limited settings due to the lack of trained personnel, medical equipment, and therapeutic agents like total parenteral nutrition (TPN), and most importantly majority of the patients are financially constrained. 3 In many third-world countries the abuse of antibiotics and their resistance leads to fatality. Sepsis, electrolyte and fluid imbalance, and malnutrition are known as the “fistula triad” for the leading cause of death related to ECF. 4 Despite the medical advancement the mortality remains as high as 50%; though there is a relative reduction in the development of ECF, once it develops the mortality rates are significant. 5 Herein we share our experience of the course of the disease in a young boy leading to fatality as a result of limitations in resources available.
Case presentation
A 4-year-old Maasai boy fell from a tree of unknown height, landing on a sharp piece of wood that pierced him in the inguinal region. He presented to our center 5 days after the fall. He had started to develop progressive abdominal distension, associated with generalized colicky abdominal pain and vomiting of greenish-yellow contents. He was accompanied by his father. The father also reported episodes of low-grade fevers that were responsive to IV Paracetamol, which was given at the peripheral health center before referral to our tertiary center. The boy had no other comorbidities with no history of prior hospital admissions. Following the fall, the boy did not report the incident at home as he was well until he started to experience the above abdominal symptoms.
On presentation, he was alert but weak, warm to touch, mild conjunctiva pallor, moderately dyspneic with nasal flaring, not cyanosed, not jaundiced, no peripheral edema and nasogastric tube (NGT) draining gastric contents. Peripheral intravenous line was secured with a 20G cannula for drugs and fluid resuscitation, and a 10 Fr catheter was inserted to monitor urine output. He had an axillary temperature of 38.2°C, blood pressure of 120/86 mmHg, pulse rate of 136 beats, saturating at 99% on 1 L/min through nasal prongs, and respiration rate of 22 breaths per minute. His body weight was 15 kg at admission. His abdomen was grossly distended and moved with respiration and there was a 5 cm linear scar just lateral to the root of the penis (healed penetrating wound scar) (Figure 1). On palpation he had generalized tenderness with positive guarding and rebound tenderness, the abdomen was hyper-tympanic on percussion with reduced bowel sounds. On rectal examination, he had normal anal verge, normal sphincter tone, empty rectum, normal rectal mucosa, and gloved finger that was stained with feces. His other systems were otherwise normal.

Clinical photograph showing healed inguinal scar—site of penetration (red).
His blood investigations revealed leucocytosis of 14.02 × 109/L, hemoglobin of 10.4 g/dl, platelet count of 496 × 109/L, raised erythrocyte sedimentation rate (ESR) of 37 mm/h and serum potassium and sodium within normal range. Initial abdominal-pelvic ultrasound showed dilated small bowel loops measuring 31.3 mm with ineffective peristaltic movement. A computed tomography (CT) scan of the abdomen-pelvis was then done and revealed a linear foreign body in the peritoneum measuring 8 cm long, air pockets in the right psoas muscle, and peritoneal collection (Figure 2).
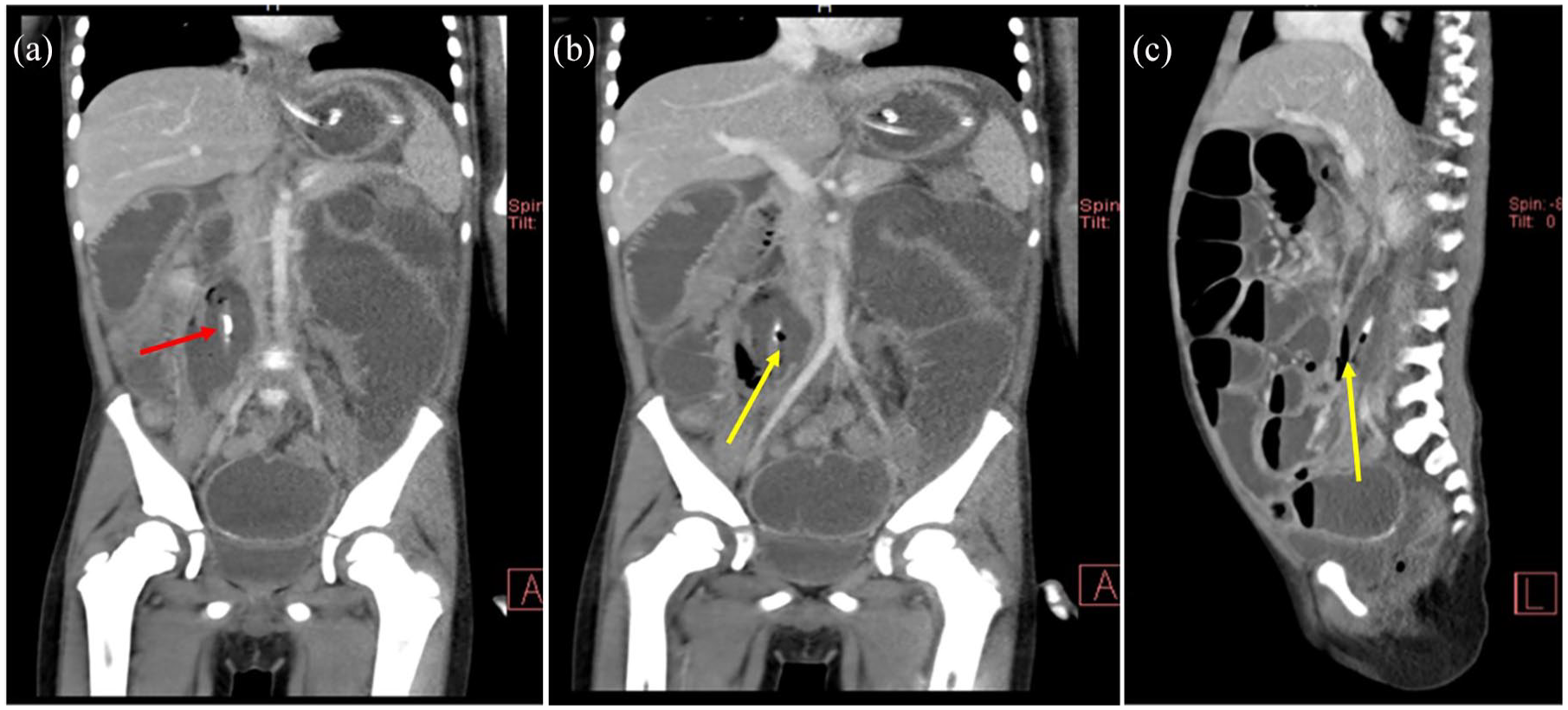
(a) and (b) Coronal abdominal CT scan showing air pockets (yellow) in the right psoas muscle and a hyper-dense object (red), (c) Sagittal Abdominal CT scan showing air pockets in the right psoas muscle and a hyper-dense object (yellow).
After thorough counseling, the father, the boy was taken for an emergency laparotomy whereby intra-operatively there was approximately 1500 ml of foul-smelling pus which was sucked and irrigated out. A terminal ileum perforation was found where a wooden stick (foreign body) was lodged. This foreign object had caused a 5 cm tear, 20 cm from the ileocecal valve, and penetrated to the retroperitoneal area (Figure 3). There was a second perforation, less than 5 mm in size which was 30 cm proximal to the first one. Approximately 10 cm of the terminal ileum was resected then end-to-end ileo-ileal anastomosis was made about 10 cm from the ileocecal junction. The smaller perforation was repaired primarily in two layers. Abdominal lavage was done, one peritoneal drain was kept and the abdomen was closed in layers. The patient recovered well from anesthesia and was nursed in pediatric surgery wards on broad-spectrum intravenous antibiotics, fluids, and analgesia according to local guidelines. The NGT was removed and he was initiated on a liquid diet 24 hours postoperatively after auscultation of bowel sounds.

(a) and (b) Intraoperative photograph showing foreign body (wooden stick) penetrating through ileum, (c) Wooden stick after extraction from the peritoneum.
In the wards, the boy could not tolerate oral feeds and developed abdominal distention and spikes of fever reaching 38.8°C on day 3. He was then transferred to the pediatric ICU and NGT was re-inserted for decompression. On day 5 he developed signs of peritonitis and his midline laparotomy wound gapped (Figure 4) and developed into a burst abdomen. He was then taken for second emergency laparotomy, whereby the anastomosis and repaired sites had given away. The terminal 10 cm of the ileum was gangrenous and hence was resected. The remaining ends were fashioned into a double-barrel ileostomy. Postoperatively the boy was nursed in ICU for 3 days and then transferred to the general pediatric surgery ward. Besides the primary surgeons, he was reviewed and managed by nutritionists, psychologists, and pediatricians. He unfortunately continued to deteriorate clinically as he developed severe acute malnutrition and peri-stoma fecal discharge 10 days later after the second laparotomy (Figure 5). Unfortunately, neither the patient nor the family had medical insurance and low economic status hence could not afford many of the ongoing investigations like serum electrolytes, albumin, and creatinine, along with parenteral nutrition. Some of the medications and lab investigations were assisted financially by some staff members of the ward and other good Samaritans (relatives of other patients in the ward).
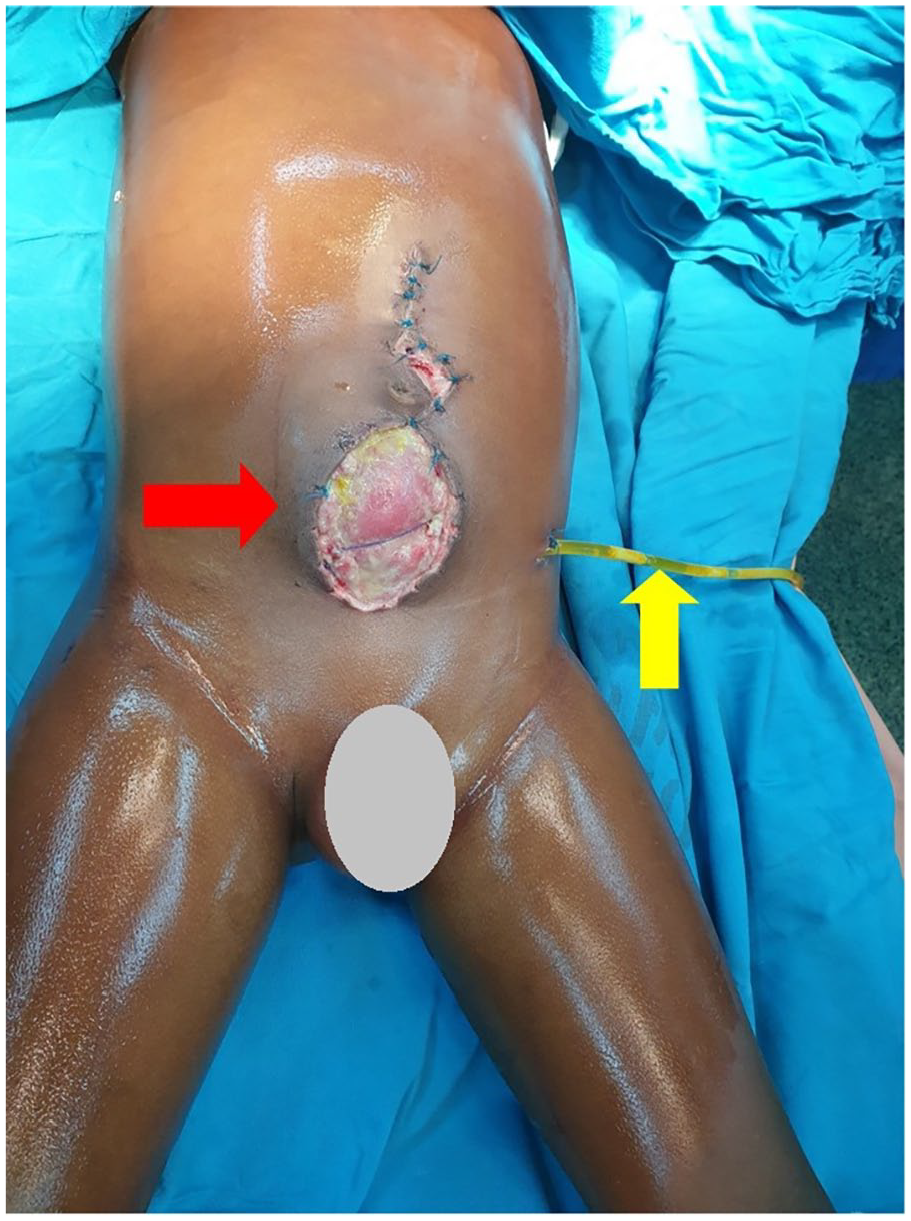
Photograph showing burst abdomen (red) with exposed bowels and drain (yellow) draining gastrointestinal contents.

Photo showing the patient 10 days post the second laparotomy with ileostomy (blue) and visible fecal discharge from the midline incision and peri-stomal area (red).
The patient was then managed as intestinal failure due to ECF with malnutrition with a multidisciplinary team approach. He was kept on oral slow-downs, oral rehydration fluids, a high-protein diet, prophylactic antibiotics from blood culture results, and oral proton pump inhibitors and the wound was dressed with zinc oxide cream up to four times a day. Despite the efforts the child’s condition continued to deteriorate due to unavoidable socio-economic circumstances of the caretakers leading to missed doses of medications and investigations. The child experienced anterior abdominal wall skin excoriations (Figure 6), severe weight loss of 12 kg, and also developed pressure ulcers. Unfortunately, the child succumbed 2 months later in the ward with the cause of death being multi-organ failure and disseminated intravascular coagulopathy secondary to sepsis.

Photograph showing anterior wall skin excoriations and prominent ribcage due to severe malnutrition.
Discussion
In this case report, we present a 4-year-old Maasai boy who sustained a penetrating abdominal injury from a fall from an unknown height. He presented late to our tertiary center with signs of intestinal obstruction and peritonitis. This case highlights poor health-seeking behavior and negligence due to low socio-economic status and education levels. It also reflects delays in the referral system at various levels, including delays by primary healthcare workers.
This child developed a high-output ECF as a result of multiple abdominal surgeries aimed at managing the primary cause. Unfortunately, the child succumbed to the adverse complications of the ECF, primarily sepsis and malnutrition. A multidisciplinary approach was employed; however, due to financial constraints, the caregivers could not afford to support the necessary needs, leading to breaks in the management and ultimately to the catastrophe.
During the management, clinicians volunteered to buy some medications and high-protein feeds, but funding was inconsistent throughout the hospital stay. The child developed significant weight loss leading to pressure sores on his sacrum, skin excoriations from the effluent, and sepsis.
ECF poses a substantial financial burden on the patient and a resource burden on the managing team, requiring close monitoring, intensive nursing care, and a multidisciplinary approach from various subspecialties.
In the past, the mortality related to ECF was 40%, but with the improvement of medical knowledge and advancement the rate has decreased to 3.5%–19%, however, management still remains a challenge. 6 Majority of these intestinal fistulas (up to 85%) are iatrogenic, following anastomotic breakdown after abdominal surgeries. Other causes, less seen in the African context, are Crohn’s disease, diverticular disease, bowel ischemia, and radiation-induced enteritis. 7 They can be classified according to their anatomical site; gastric, pancreatic, duodenal, jejunal, ileal, or colonic. They can be also divided in terms of their output as high- (>500 mls/24 h), intermediate- (200–500 mls), and low-output (<200 mls), or, can be classified as primary (due to intestinal disease process) or secondary (as a result of surgery). 8 In the case presented, from estimation the output was more than 500 a day as we had limited access to large colostomy bags and no other options to contain and monitor the effluent.
The overall mortality rate of ECF is between 10% and 30% and is associated significantly with increased odds of readmission. 9 Hatchimonji et al. 9 found out that the rate of readmission was 50% in their study. This shows the need for further research is needed for this group of population. Besides that, the financial burden remains a challenge to medical facilities. For comparison, the medical cost for colorectal surgery is US$ 9000 per stay in the USA compared to US$ 55,000 for the management of ECF. This numbers cannot even be compared to sub-Saharan countries where an individual cannot even earn this amount in a whole year. To date there are only a few studies describing the economic and clinical implications of ECF that are even done in the Western world hence there is a need for such studies in developing countries. 10 Brookes et al stated in their paper that ECF accounted for 230,000 hospital days and US$ 1.5 billion annually, representing a significant public health expenditure in the USA. 10 Financial constraints were evident in the index case and were a major cause of break in the continuity of management of ECF.
Damage control and its principles have become a common practice in trauma care, open abdominal management has become a frequently used practice and may increase the risk of ECF also referred to as entero-atmospheric fistula (EAF) with a risk between 4.5% and 40%. 11 The risks of developing ECF/EAF after trauma are multiple, major cause being injury to hollow viscus; however, the location and number of anastomosis have not been clearly linked as independent risk factors. 11 This can be related to the index case where the independent risk factors are small bowel injury that presented late to our center after the patient developed fecal peritonitis. Wabada et al. 12 states in their paper that trauma is a major threat to child health in Africa and in his study a third had penetrating injury with a male predominance. They continue to state that rarely penetrating trauma in children occurs without underlying visceral injury as the abdominal cavity is fully occupied by viscera. The authors had a complication rate of 33.3%, death was attributed to ECF, and also experienced a delay in presentation. 12
Management of ECF is complex and needs multidisciplinary approach. Newly diagnosed patients need to be thoroughly investigated and resuscitated in terms of fluid correction, management of electrolyte imbalance, controlling and quantifying the output, and treatment of acute infection/sepsis. 13 These patients have increased energy demands due to the ongoing inflammation and hence are at risk of malnutrition, therefore, with aid of nutritionists they have to be monitored closely and on a high-protein and caloric diet. 13 This includes the use of TPN, whereby, in the index case was a great limiting factor due to economic constraints. On the contrary, TPN has its related complications that need to be addressed. 6 TPN was prescribed but was unaffordable for the family. Instead, a high-protein and high-calorie diet was recommended using everyday foods that were easily available at affordable prices, such as eggs, peanuts, milk, and fish (dagaa).
Many fistulas can close spontaneously without surgery in 50%–80% of cases especially those with intact abdominal walls. 9 However, those who failed conservative management require proper intraoperative decision and maximum preoperative optimization. 13 Appliances like vacuum-assisted closure (VAC) dressings have numerous benefits like containing effluent, skin protection, and preventing further tissue breakdown. The mentioned benefits were the complications in our case; however, VAC dressing was not available in our setting. 13 There are other technologically advanced equipment like fibrin sealant, endoscopic clips for laparoscopic management of acute fistulas, fistula plugs/patches, and 3D-printed fistula stents, which are unavailable in resource-limited settings like ours. 13
Conclusion
ECF remains a major surgical problem globally and poses great economic strains on the managing facility and those who are affected. Despite medical advances morbidity and mortality remain high, especially in resource-limited settings. It is also important to quantify the impact of ECF on the health care system, on patients, and on health economics.
Footnotes
Acknowledgements
The authors would like to thank the patient’s father for his permission to share his son’s medical history for educational purposes and publication.
Author contributions
J.L. conceptualized and drafted the manuscript. J.T. and A.H. reviewed the medical records. D.M. was the clinical supervisor. All authors have read and approved the final script.
Availability of data and material
We have not shared patient’s hospital records as they contain personal identification information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.