
Abstract
Granulomatous dermatitis is a common tissue reaction pattern seen in the skin or systematically in various presentations. Granulomatous dermatitis can be subclassified into infectious and non-infectious categories. This article focuses on a patient with non-infectious granulomatous dermatitis followed for many years. Past medical history included bilateral total shoulder arthroplasty complicated by prosthetic joint infections. In its early stages, the axillary rash was painful and had many fluid-filled blisters. Ultimately, the histology of the rash deemed the lesion non-infectious and mostly due to an inflammatory process. Specifically, ionizing radiation was used for this patient. The category of granulomatous processes is broad and there are many subtypes. Other treatment options for non-infectious granulomatous processes may include corticosteroids, phototherapy, and interferon-gamma injections. The differential for granulomatous processes is extensive and treatment should be decided on a case-by-case basis.
Introduction
Granulomatous dermatitis is a common tissue reaction pattern seen in the skin or systematically in various presentations. A granuloma is composed of epithelioid cells with a varying amount of lymphocytic inflammatory cells and giant cells; however, the etiology of this process is not well understood.
Granulomatous dermatitis can be subclassified into infectious and non-infectious categories. Infectious causes of granulomatous dermatitis are seen in developing countries more often, whereas the non-infectious forms are prominent in the US. Due to the diversity in types of granulomatous processes, treatment options vary, and it may be hard to find a curable option.
Case presentation
A 72-year-old male presented to the Department of Radiation Oncology with aseptic granulomatous dermatitis, related to a previous shoulder arthroplasty and infection, immediately status post-coronary artery bypass graft.
The arthroplasty was originally complicated by a prosthetic joint infection which required three revision procedures of debridement, antibiotics, and implant retention (DAIR). The infection was due to methicillin-sensitive Staphylococcus aureus (MSSA) and the patient was started on doxycycline for treatment. After 3 years, the patient underwent left reverse shoulder arthroplasty. After the patient’s reversal surgery, the patient developed edema, erythema, and pustules at the site of the incision, similar to the right shoulder. Subsequently, the patient underwent four DAIR procedures on the left shoulder. Cultures of the site were positive for Propionibacterium. Joint aspiration of the left shoulder was completed which yielded MSSA. At that time, surgery recommended resection arthroplasty followed by reimplantation arthroplasty of the left shoulder. These surgeries were performed and following the reimplantation arthroplasty, 6 weeks of ceftriaxone was given. Cultures after the 6 weeks of medication grew MSSA, and the patient has been on suppressive doxycycline since that date.
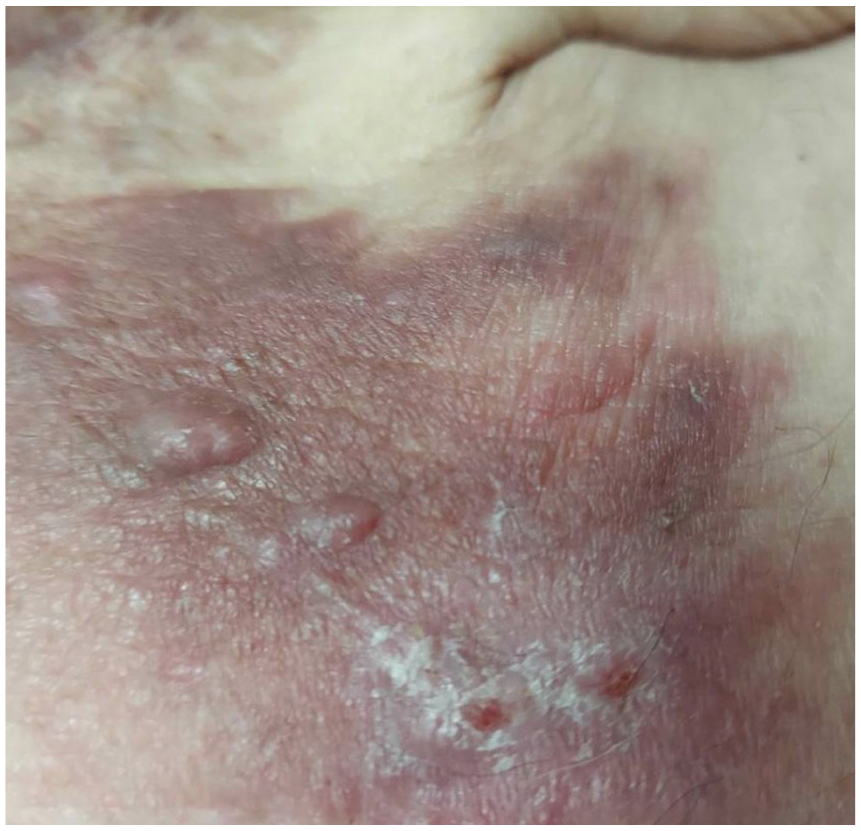
The patient then noticed a vesicular rash in the left anterior axilla/chest and was evaluated by dermatology at another institution and underwent two biopsies (Figure 1). Upon biopsy, dermatology noted that the rash bled easily. At that time, results showed granulomatous inflammation stains and cultures were negative. The patient’s QuantiFERON, Blastomyces, VZV PCR, HSV 1 and 2 PCRs from the left upper chest were all negative.

The patient had two biopsies taken of the axilla, both of which were non-malignant. The patient noted no pruritis or pain accompanied by the rash. Vesicles would occasionally drain clear fluid.
The patient underwent aspiration of the glenohumeral joint, and his aspiration cultures grew pan-susceptible Staphylococcus aureus. He was placed on doxycycline, and his MSSA infection was fortunately doxycycline susceptible; therefore, his quiescent infection was appropriately suppressed. Two weeks later, dermatology deemed that the rash was not infectious.
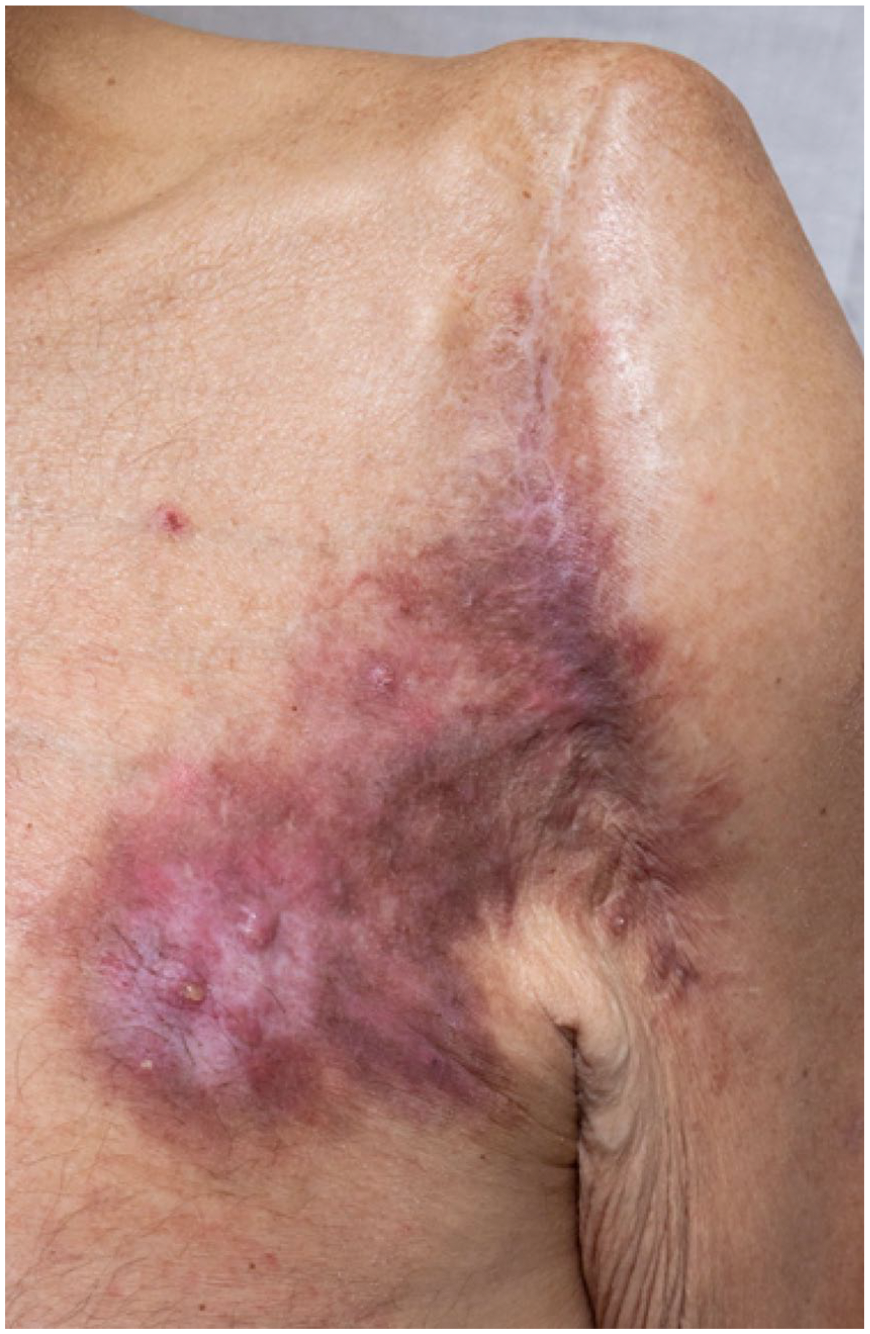
The patient underwent coronary artery bypass graft surgery due to severe coronary artery disease. Eight days after surgery, radiology oncology requested that the patient send photos in 28 days to monitor the progression of the rash (Figure 2). At the 28-day check-in, the patient sent photos and mentioned in his portal that the rash seemed to be healing well (Figure 3).

Eight days after coronary artery bypass surgery.
Twenty-eight days after coronary artery bypass surgery. The patient believed his axillary rash was healing well.
Unfortunately, the rash began to worsen once again (Figure 4). At the time there was no evidence of recurrent infection, and the patient was still on suppressive antibiotics (Figure 5). Following this encounter, the patient received 20 Gy over five fractions to the left chest for 5 days. A few weeks later, the patient sent a follow-up picture showing improvement in the rash itself (Figure 6). Drainage from the shoulder occurred while on doxycycline and cultures tested positive for MSSA. The patient underwent resection arthroplasty of the total left shoulder, and the surgeon placed vancomycin and gentamicin-impregnated cemented prosthesis spacer. The patient was placed on indefinite suppressive doxycycline and has been doing well since.

Rash returned and began to worsen. Radiology oncology noted the axilla needed daily dressing changes at this time.
No evidence of recurrent MRSA infection. The patient was still on suppressive antibiotics.

A few weeks after five sessions of ionizing radiation the rash continued to improve in its appearance.
Discussion
Granulomatous dermatitis is a common tissue reaction pattern seen in the skin or systematically in various presentations. Infectious causes of granulomatous dermatitis are seen in developing countries more often, whereas the non-infectious forms are prominent in the US. Concerning types of granulomatous dermatitis that may be seen in America, there are quite a few including tuberculoid granuloma, suppurative granuloma, interstitial granuloma, and sarcoidal granuloma among a few others. 1
During an innate immune response, macrophages are recruited to the site of inflammation to remove inflammatory debris and return the tissue to its normal state. If the macrophages are unable to remove the debris, more macrophages will be recruited to the site, and they will form a tight formation around the inflammatory stimulus which causes the focus we know as a granuloma. 2
Much research has been conducted surrounding the anti-inflammatory effects of low-dose radiotherapy in the treatment of disease. Specifically, low doses of ionizing radiation stimulate antigen uptake and lower antigen presentation, which causes a suppression of pro-inflammatory markers. 3 A study conducted on mice specifically observing the effects of low dose gamma-irradiation concluded that subtle changed in cytokines post-radiation therapy can boost immune responses in autoimmune conditions without causing detrimental change to hematopoietic components. 4
Concerning radiation’s effect on granulomatous tissue, a study was conducted in 1998 in which chronic granulomatous air pouches were induced into a select group of mice. Like the patient in our case, the mice were given five daily doses of ionizing radiation. After the radiation was given to the mice, it was concluded that the radiation interfered with the nitric oxide and heme oxygenase pathways to control inflammation and inflammatory pain; however, no significant reduction in granulomatous weight was seen. This study helped to show that ionizing radiation may help with the painful side effects of a granulomatous disease but does not fully eradicate the granuloma formation. 5
A case report published in 2019 reported that radiotherapy in the setting of central giant cell granuloma can be used as a rescue treatment to significantly reduce the size of a granuloma. 6 On the other hand, high doses of radiation can also end up causing granulomatous inflammation when delivered to the head and neck region, but these granulomas can be cured at high remission rates. 7
Studies have shown that surgical removal of granulomatous infections is still the primary treatment; however, for the patient presented in this case, ionizing radiation was necessary. 8 After the timeline of the patient receiving multiple surgeries and medications to remove the granulomas of the left shoulder, pain and inflammation persisted. Turning to radiation therapy was the next best option. The radiation aided in acting at the intracellular and nuclear levels to boost immunity and activate the innate immune system. 9
Although radiotherapy for benign disease remains controversial, the benefits of radiotherapy in the setting of benign diseases should be balanced against the risk of secondary malignancies. 10
Footnotes
Data availability
Research data are stored in an institutional repository and will be shared upon request to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
Informed publication consent from the patient has been received