
Abstract
The diagnosis of a bullet inside the hip joint is a rare finding. The usual method to treat this condition has been open surgery, with its associated complications and morbidity. The arthroscopic approach has been increasingly utilized for the diagnosis and treatment of several hip conditions, and the number of indications for this technique has been steadily rising. We report the case of a 35-year-old man who suffered a gunshot wound and was operated on for abdominal perforation. He later presented with groin pain that worsened with weight-bearing on his right leg and then underwent arthroscopic removal of a bullet located inside his right hip joint. After a 2-year follow-up, the patient had an excellent clinical outcome, with no radiologic signs of arthritis. The removal of an intra-articular projectile is necessary to avoid complications such as synovitis, osteoarthritis, septic arthritis, and saturnism. The best access to the hip joint remains a topic of debate. Arthroscopy has the advantage of less soft-tissue damage and quicker recovery. The treatment of associated chondral lesions can be done with several techniques, including microfracture, autologous chondrocyte implantation, mosaicplasty, and fresh osteochondral allograft transplantation. There is no consensus as to the best course of treatment for associated chondral lesions in such cases. Hip arthroscopy can be a safe and effective technique for the removal of intra-articular bullets in the hip.
Introduction
Surgical access to the hip joint is usually performed by open approaches. These approaches usually require extensive tissue dissection, causing significant postoperative morbidity. 1 Hip arthroscopy has gained increasing importance in the diagnosis and treatment of hip joint pathology.2,3 Hip arthroscopy offers a minimally invasive access to the joint, with less tissue dissection, thus allowing faster postoperative rehabilitation.3,4 Some of the current indications include: diagnosis and treatment of labral and chondral lesions, synovial chondromatosis, femoroacetabular impingement, fractures, and biopsies.3,5 This list of indications has been steadily growing. 6 In this article, we describe a case in which arthroscopy was used for the removal of a bullet that was located inside the hip joint.
This case report has been written in line with the SCARE criteria. 7
Case report
We present a case of a 35-year-old man, who was a victim of a single pistol gunshot. The input wound was found on the left flank, and no exit wound was found. The patient was hemodynamically stable but had clinical signs of acute peritonitis (involuntary guarding and rebound tenderness). Laparotomy was indicated and two minor small intestine perforations were found, without major vascular injuries. The patient recovered well, without need for abdominal reoperation.
After trying to walk without aid, he complained of pain in the right groin extending to the medial aspect of the ipsilateral thigh. He noted that the pain worsened with full weight-bearing and movement of the hip joint. He also experienced some crepitation with hip joint movement.
A pelvis radiograph was done, and a bullet was identified in the right hip joint. Part of the projectile was in an intra-articular position, confirmed by oblique views and computed tomography (Figures 1 and 2). We presumed that the bullet entered the left flank, perforated the peritoneum and intestine, and then struck the right acetabulum from the inside, losing speed and stopping inside the right hip joint.

Preoperative radiographs: (a) Lequesne false profile view, (b) Dunn view, and (c) anteroposterior view.

Preoperative tomography to identify the exact location of the projectile: (a) sagittal view, (b) coronal view, (c) axial view, and (D) 3D reconstruction.
Removal of the projectile was indicated, using an arthroscopic approach. The procedure was performed in the dorsal decubitus position, on a traction table, under bilateral traction. Modified anterior and anterolateral portals with interportal capsulotomy were performed. A large articular hematoma was evacuated, while multiple bone and chondral loose bodies were observed inside the joint, all of which were thoroughly washed out and removed using an arthroscopic shaver. After extensive joint irrigation, the projectile was clearly visualized in a posterosuperior location in the acetabulum.
Pump pressure was kept as low as possible at all times, to avoid abdominal liquid extravasation and compartment syndrome. Abdominal distension was evaluated clinically in frequent intervals to check for this possible complication. 8
Part of the projectile protruded into the joint surface, with a full-thickness lesion of the posterosuperior acetabular cartilage, measuring approximately 3 × 2 cm (Figure 3). In the same location, we identified a 1 × 2 cm full-thickness mirror chondral lesion on the femoral head.
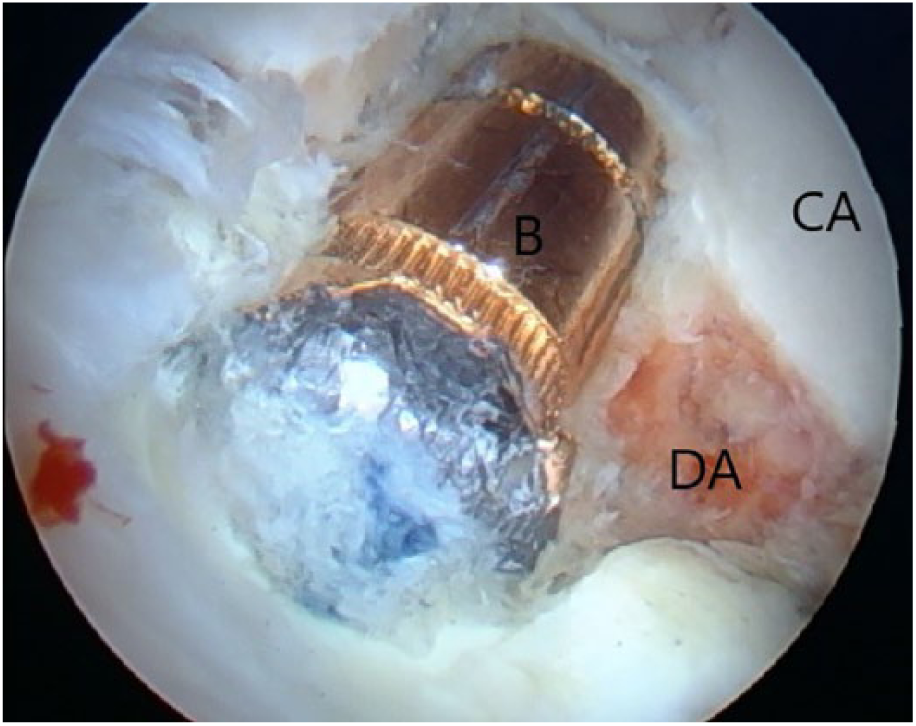
Intraoperative photo with projectile located in the intra-articular position, within the acetabular cartilage in the posterosuperior acetabulum. Full-thickness chondral lesion around the projectile. Maceration and fragmentation of the surrounding cartilage.
The projectile was removed arthroscopically, without the need for an open arthrotomy. After the projectile was removed, the chondral defects were extensively debrided (Figure 4).
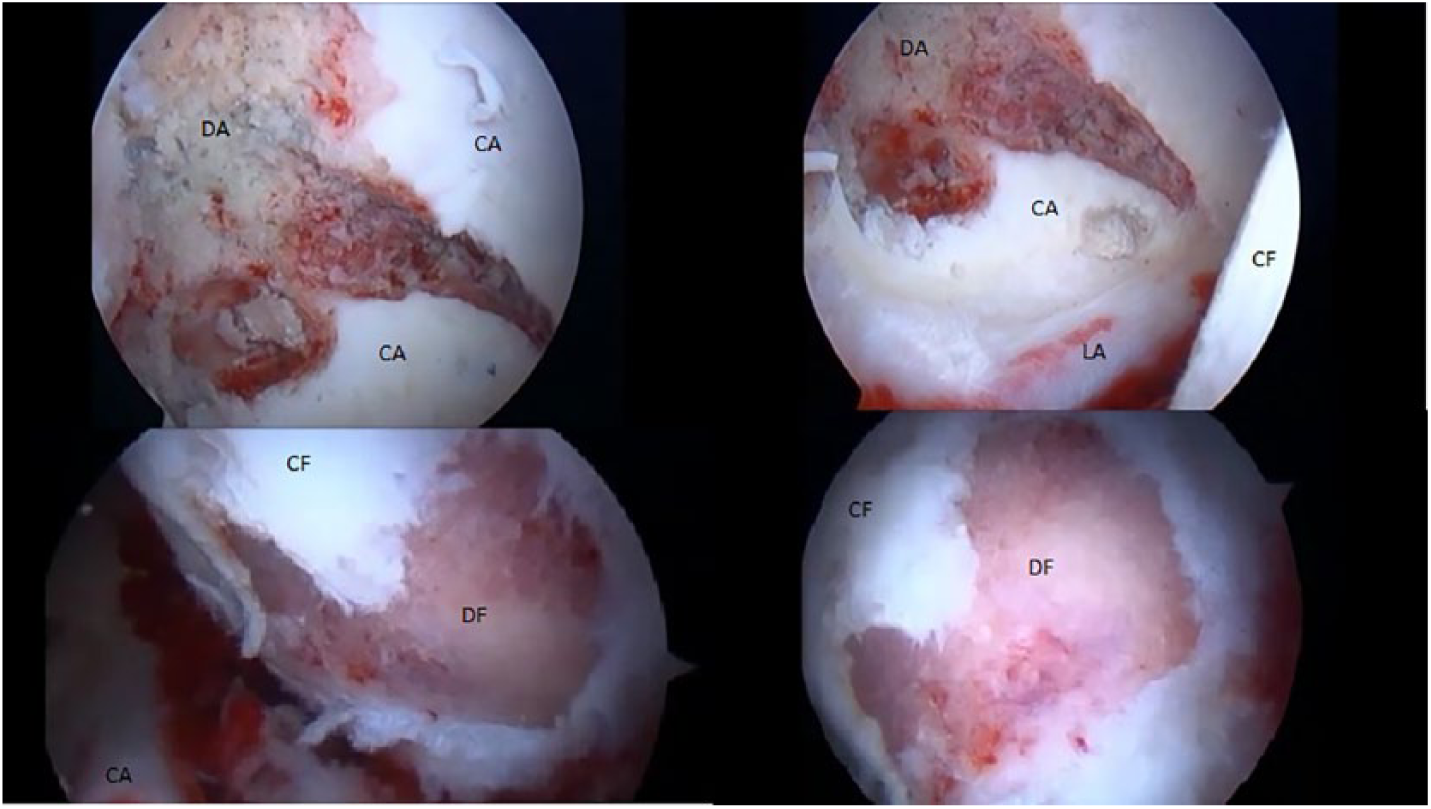
Intraoperative photos without the projectile—extensive chondral defect in the acetabulum and femoral head after removal of the projectile and loose chondral fragments.
Microfractures were then performed on the acetabular bone, aiming to stimulate the formation of fibrocartilage to fill in the chondral defect.
The patient underwent standard physiotherapy for arthroscopy, with early joint mobilization. No weight-bearing was allowed on the affected limb for 8 weeks. The patient had an uneventful recovery, with healing of the portals and no infection. After a 27-month follow-up, he only felt occasional mild pain. He had total and symmetrical hip range of motion, reporting no analgesic or anti-inflammatory use, and no limitations of activities of daily living. Follow-up images demonstrated no signs of hip chondrolysis, osteonecrosis, or arthritis, including a magnetic resonance imaging (MRI) exhibiting the bone and chondral defects filled by nonspecific scar connective tissue (Figure 5).

Follow-up images: (a) AP radiograph, (b) profile radiograph, (c) coronal MRI, and (d) sagittal MRI.
Discussion
The first report of the use of arthroscopy to remove a projectile located in the hip joint occurred in 1998 by Cory and Ruch. 9 The removal of the projectile intends to avoid complications such as synovitis, post-traumatic osteoarthritis, septic arthritis, and lead poisoning (saturnism or plumbism).9–11 This occurs because the synovial fluid allows for a greater systemic absorption of the metal that can cause central nervous system disease, renal toxicity, hypertension, memory loss, fatigue, insomnia, loss of libido, and depression. 10
Therefore, the removal of the projectile is indicated when it is intra-articular. Nevertheless, the best access to the hip joint remains a matter of controversy. The most widely accepted open access option is the controlled dislocation technique described by Ganz et al., 12 that was used by Delaney et al. 13 in a similar case in 2011. The authors chose the open approach due to a displaced fracture of the femoral head. The projectile was in the posterior aspect of the femoral head, where arthroscopic access is difficult. Surgical dislocation provided global visualization of both the femoral head and the acetabular surface, allowing fixation of large fractures of the head as well as repair of associated chondral and labral lesions in any region of the joint. Nevertheless, this technique carries possible complications including sciatic nerve injury, failure of the large trochanter fixation, heterotopic ossification, and scarring. 12
In this case, the arthroscopic approach was chosen because of the absence of fractures to be treated, the lower risk of complications, and the possibility of accelerated postoperative rehabilitation. Howse et al. 11 described their technique for arthroscopic bullet removal in the hip. The authors successfully retrieved intra-articular bullets in four patients. Interestingly, they found that hip arthroscopy was also a possible treatment method for bullets located in the peripheral compartment, including around the femoral neck. Three of the four patients underwent an exploratory laparotomy, as did the patient presented in this report.
The treatment of associated lesions, mainly acetabular and femoral chondral damage, also deserves discussion. According to El Bitar et al., 14 most treatment options for these lesions are imported from the knee literature and require scientific validation in the hip. Among these techniques, microfracture is an inexpensive option especially for smaller lesions that can be performed arthroscopically, even in lesions not previously diagnosed. 15 Autologous chondrocyte implantation (ACI) is an option for larger lesions, between 3 and 10 cm2. 16 It is done in two stages: the first procedure is the collection of chondrocytes in a healthy joint, and the second procedure is a controlled dislocation, for chondrocyte implantation after laboratory ex vivo culture. In addition to causing morbidity in the donor area, it presents the risks associated with an open surgical dislocation. Stem cell scaffolds could be an alternative, with less donor site morbidity. 17 Mosaicplasty is a technique in which osteochondral lesions are repaired by harvesting and transplanting cylindrical plugs of bone and cartilage. Another option would be a fresh osteochondral allograft transplantation, for which an osteochondral cadaver graft is used, for defects larger than 2.5 cm2. Its disadvantages are the risk of disease transmission and the low availability of allografts in many hospitals.16,17
In this case, an arthroscopic technique was successfully used for the removal of an intra-articular projectile in the hip, with good clinical outcome.
After a 2-year follow-up, our patient had total and symmetrical hip range of motion. He reported no medication use, and had no limitations of activities of daily living. Follow-up images demonstrated no signs of short-term complications such as chondrolysis or osteonecrosis. At this time, it is not possible to know if he will develop arthritis over the long term. There is no consensus as to the best treatment for chondral lesions in similar cases.
Conclusion
Hip arthroscopy can be a safe and effective technique for the removal of intra-articular bullets in the hip.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the local ethics committee—Hospital De Acidentados.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.