
Abstract
Intramuscular Myxomas are rare benign soft tissue tumors which usually occur between the ages 40 and 70 years and are more common among females. A thorough history and examination can help with diagnosis and it can be confirmed via histological examination. A 40-year-old female presented with a swelling in the medial aspect of right thigh which measured about 5 × 5 cm. Ultrasound, magnetic resonance imaging, and histopathology examination confirmed the diagnosis and a complete surgical resection was performed to remove the mass. Intramuscular myxoma should be included in differential diagnosis of sarcomas, hemangioma, desmoid tumor, clear cell sarcoma, and lipomas. Magnetic resonance imaging should be the investigation of choice, and histopathology remains the gold standard of investigation. Complete surgical excision with negative margins is the treatment of choice.
Introduction
Intramuscular myxomas are benign rare soft tissue tumors of mesenchymal origin. These typically present as deeply seated swellings and are classically described as hypocellular and hypo-vascular lesion with large extracellular myxoid matrix deposition. However, intramuscular lesion shows heightened cellularity and vascularity that can proceed to misdiagnosis of sarcomas. Other tumors which can exhibit myxoid feature or may be subclassified are: aggressive angiomyxoma, chondrosarcoma, embryonal rhabdomyosarcoma, leiomyoma, leiomyosarcoma, liposarcoma, and neurofibroma. Immunohistochemical analysis may or may not reveal desmin or vimentin proteins. Incidence of intramuscular myxoma varies from 0.1 to 0.3 per 100,000 individuals. 1 Individuals between the ages of 40 and 70 years are affected the most and it is more common among females (66%). 1 In light of the literature available to date, intramuscular myxomas most commonly occur in the muscles of thigh, with less common sites being the shoulder, buttocks, lower leg, and upper arm.1,2 Intramuscular myxoma share the same anatomical location as fibrous dysplasia, which is known as Mazabraud’s syndrome. 5 Diagnosis can be made with good history and examination; however, a robust diagnosis can only be made upon histological examination. Histology, usually shows plenty of mucoid material and relative hypocellularity and loose reticulin fibers. The shape of the cells is stellate with a hyperchromatic pyknotic nuclei and little amount of cytoplasm. Some myxomas may show focal areas of hypercellularity; however, absent mitotic figures, nuclear atypia, or necrosis help exclude malignancy. 1 Magnetic resonance imaging (MRI) can also prove to be helpful. Treatment of choice is complete surgical excision and the rate of recurrence is very low. 1 This case report aims at highlighting a rare case of intramuscular myxoma presenting as a swelling in the thigh.
Case presentation
A 40-year-old female with no known comorbidities presented to the outpatient department with a complaint of swelling over the inner right thigh observed 3 months ago. She did not complain of any pain associated with the swelling or discharge. The patient was however concerned about its gradual increase in size, which she stated was the size of a pea and now is the size of a lemon. She has no difficulty in walking or weight bearing and is able to perform regular routine activities. She does not give any similar history of swelling elsewhere in the body and neither a positive family history for lumps. Review of systems is unremarkable and she hails from a moderate socioeconomic background.
On examination there is a 5 × 5 cm swelling over the medial aspect of upper right thigh with no overlying skin changes, difference in color, or punctum. The swelling is non-tender and firm in consistency. It appears to be fixed to the underlying structure with slight mobility, is not attached to the overlying skin, and is non-fluctuant. Neurovascular exam of the affected limb was unremarkable and no lymphadenopathy was associated. Routine blood and urine examination showed no abnormalities.
Ultrasound of the swelling displayed a well-defined hypo-echoic solid lesion measuring 2.2 × 2.9 cm at the lower aspect of the right thigh representing benign lesion. An MRI was performed, which showed well-defined focal cystic lesion in substance of vastus medialis muscle approximately 3.2 × 3.5 cm without any bony erosion (Figures 1, 2, and 3).

MRI scan showing the swelling. Coronal MRI section showing high intensity on T2 imaging in soft tissue mass.
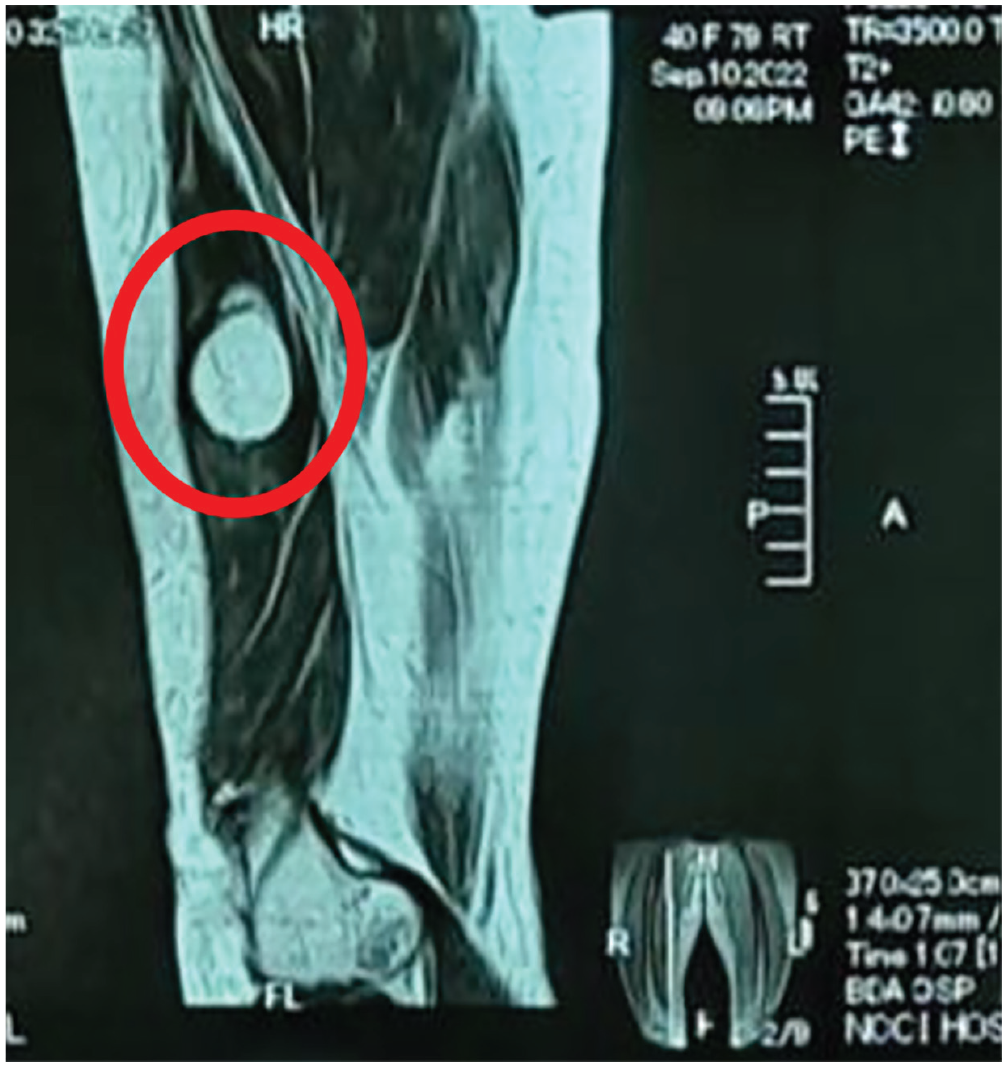
MRI scan showing the swelling. Sagittal MRI section showing high intensity on T2 imaging in soft tissue mass.

MRI scan showing the swelling. Axial MRI section showing high intensity on T2 imaging in soft tissue mass.
The patient underwent excision of the swelling under spinal anesthesia. Postoperatively, the swelling was found embedded in the vastus medialis muscle, and a careful excision was done without damaging the surrounding tissue (Figure 4). Postoperatively, the patient was discharged home the next day and was called for follow-up after a period of 7 months. Ultrasound done showed no signs of recurrence and now patient will be kept on follow-up after 3 months.

Macroscopic gross picture of the swelling.
Definitive diagnosis was made using hematoxylin and Eosin staining at ×100 and ×400 magnifications. Microscopic features revealed benign hypocellular lesion surrounded by collagenized capsule composed of bland spindle-shaped cells in basophilic matrix. This confirmed intramuscular myxoma as the diagnosis.
Discussion
Intramuscular myxomas are benign soft tissue tumors, which are rare, mesenchymal in origin, and presents as deeply seated swellings. They are classically described as hypocellular and hypo-vascular lesion with large extracellular myxoid matrix deposition; however, intramuscular lesion shows enhanced cellularity and vascularity that can lead to misdiagnosis of sarcomas. Patients usually present with swelling, which occurs in areas with large muscles like thigh, shoulders, arms, and buttocks. Diagnosis can be made with good history examination and histopathological examination. MRI can also be helpful; however, positron emission tomography scans are rarely used. Treatment of choice is complete surgical excision and reoccurrences are exceptional.1,2,3
The myxoma can present as an isolated lesion or together with fibrous dysplasia or Albright syndrome.3,4 The presence of multiple lesions, which are also associated with fibrous dysplasia, is named as Mazabraud’s syndrome. 5 On examination, intramuscular myxoma manifests as a painless, palpable mass, usually single, firm in consistency, slightly mobile, and often fluctuant. 6 At present, choices of radiological modalities for assessment are ultrasound, computed tomography (CT) scan, and MRI. On ultrasound, the intramuscular myxoma appears as a hypo-echoic lesion with well-defined margins. The CT scan of an intramuscular myxoma shows a well-demarcated homogeneous low-density lesion within the substance of skeletal muscle. MRI of the swelling shows low-signal intensity on T1 and high-signal intensity on T2 weighted, gradient echo, or short tau inversion recovery images. 7
Diagnosis is unclear without biopsy and microscopy; moreover, due to the large amount of myxomatous tissue and poor cellularity, it is often arduous to confirm a diagnosis on fine needle aspiration cytology.6,8 Gross specimen is mucoid or gelatinous, usually poorly demarcated, and may have disrupted borders. Small cyst-like spaces or traversing trabeculae can be appreciated with a disrupted fibrous capsule. 9 Histology usually shows plenty of mucoid material, relative hypocellularity, and loose reticulin fibers. The shape of the cells is stellate with a hyperchromatic pyknotic nuclei and little amount of cytoplasm. Some myxomas may show focal areas of hypercellularity; however, absent mitotic figures, nuclear atypia, or necrosis helps exclude malignancy. Alcian blue, colloidal iron, and mucicarmine stains are positive for mucoid material. A positive vimentin stain and no reaction for S 100 are seen on immunohistochemical studies. 3
The exact cause of Intramuscular Myxoma (IM) is still unknown. However, studies in the literature have shown that mutations in the guanine nucleotide binding protein, alpha stimulating (GNAS) gene are common in IMs. The GNAS gene is responsible for encoding a protein called Gαs, which plays a role in intracellular signaling pathways. Mutations in this gene can lead to abnormal cell growth and contribute to the development of certain tumors, including IMs. To aid in the detection of GNAS gene mutations, new molecular techniques are being developed. Two such techniques are the TaqMan assay and single-molecule tagged molecular inversion probes. These techniques can help researchers and clinicians identify specific mutations in the GNAS gene, providing valuable information for diagnosis, prognosis, and potential targeted therapies.
These GNAS1 mutations are somatic post-zygotic events, meaning they occur after fertilization and result in a mosaic distribution of mutation-bearing cells within the affected tissues. The mutations are not inherited but arise spontaneously in the affected individual. To date, only a limited number of reported cases have identified GNAS gene mutations in IMs. Among these cases, two were non-syndromic IMs with specific GNAS mutations (R201H and R201C), while the other five cases occurred as part of Mazabraud’s syndrome, with four cases having the R201H mutation and one case having the R201C mutation. Further research is needed to better understand the role of GNAS gene mutations in the development of IMs.
The tumor differentials can be aggressive angiomyxoma, chondrosarcoma, embryonal rhabdomyosarcoma, leiomyoma, leiomyosarcoma, liposarcoma, and neurofibroma. 9 Surgical removal is the treatment of choice and there is insignificant chance of recurrence.3,4,6 This presence of an intramuscular myxoma can be considered as an indication for a skeletal survey for silent fibrous dysplastic lesions, which can then be followed up regularly. The case report describes the patient undergoing excision of the swelling, resulting in a successful outcome with no signs of recurrence during the follow-up period. This aligns with the discussion, which mentions that surgical removal is the preferred treatment option and that recurrences are exceptional.
This study is unique in a way that it reports a rare case of intramuscular myxoma of thigh and the limitations associated are that there are no definitive management guidelines in the literature, thus more research in this field is required and this case report, along with other reported cases can be used to formulate a standard management.
Conclusion
To conclude, intramuscular myxomas are benign tumors which are very rare and appear in the long muscles. A patient presenting with a swelling which is soft and solitary should be investigated properly with intramuscular myxoma as a differential diagnosis. Treatment choice is complete excision of the swelling and rate of recurrence is very minimal. The above case report supports all these facts.
Footnotes
Author contributions
S.J. took lead in writing the article and collecting data from the patient. O.K.J. and Z.H.T. edited and designed the final report. All authors provided with critical feedback and helped to shape the final report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Provenance and peer review
Not commissioned, externally peer reviewed.