
Abstract
In this case report, we describe a rare imaging finding of foveal duplication identified on spectral domain optical coherence tomography (OCT) through undilated pupils in a 49-year-old asymptomatic anxious lady with type 2 diabetes mellitus who visited the retina clinic for diabetic retinopathy screening. A simple patient counseling for cooperation during a repeat OCT scan with dilated pupils revealed that the twin fovea-like duplication was an illusion. This case illustrates the necessity of pupillary dilation and reimaging in the presence of unusual artifacts, such as foveal duplication, to prevent clinicians from ordering unnecessary additional tests.
Introduction
The fovea centralis, also known as the fovea, is a small depression in the center of the macula that is responsible for a person’s central vision. 1 A number of true abnormalities and artifacts at the fovea have been described in the literature, causing distortion of the foveal contour and vision abnormalities that are best identified using non-invasive retinal imaging such as optical coherence tomography (OCT).2,3 One such uncommon artifact reported on OCT in scientific literature is foveal duplication.4–6
In this report, we describe a case of foveal duplication discovered on OCT, which was similar to previous cases reported; however, the foveal duplication disappeared after reacquiring the OCT scans with adequate pupillary dilation.
Case report
A general ophthalmologist referred a 49-year-old asymptomatic female with a known history of diabetes mellitus for diabetic retinopathy screening. She complained of minimal blurring in her right eye, and her documented visual acuity in both eyes was 6/6, N6. Both eyes’ undilated anterior segment examinations were normal, except for a very early cataract haze in both eyes. Because the pupils were miotic, the clinician was unable to properly grade diabetic retinopathy. The patient refused a dilated fundus examination. A horizontal macular cube 512 × 128 OCT scan was performed through the miotic pupil of both eyes on the Cirrus HD-OCT (version 5.0; Carl Zeiss Meditec Inc., Dublin, CA) machine to avoid missing any treatable macular pathology at the fovea. The technician reported that the patient was extremely uncooperative during the scan and that capturing the images was difficult. The OCT scan with a signal strength of 8/10 passing through two different regions of interest showed two similar looking depressions one below the other appearing as a double fovea in the patient’s right eye (Figure 1(a) and (b)). This was confirmed by an internal limiting membrane (ILM)-retina pigment epithelium (RPE) map that showed a more distinct delineation of the twin fovea (Figure 2(a)). The OCT scan of the left eye was normal. The patient was requested for a dilated fundus examination, which revealed that both eyes’ fundus was normal. After adequate pupillary dilation and proper patient counseling to cooperate for the scan, the OCT scans were repeated on the same day to confirm the finding of foveal duplication (Figure 1(c)). The signal strength of the OCT scan was 7/10. This time only one foveal dip was identified and the other one disappeared as seen on the ILM-RPE map, implying a foveal duplication artifact (Figure 2(b)). Written informed consent was obtained from the patient for publication of this case report and any accompanying images.

Optical coherence tomography (OCT) of the right eye before and after pupillary dilation. (a and b) Horizontal macular cube 512×128 scans of the right eye obtained on the spectral domain OCT machine with Cirrus HD-OCT (version 5.0; Carl Zeiss Meditec Inc., Dublin, CA) with signal strength 8/10 at 12.02 p.m. without pupillary dilation showed twin fovea-like depressions at two separate scan co-ordinates, thereby giving the impression of foveal duplication or double fovea. (c) OCT scans were repeated with the same scan specifications mentioned and signal strength 7/10 at 1.05 p.m. after adequate pupillary dilation, which showed the existence of only one foveal depression at its anatomic location.
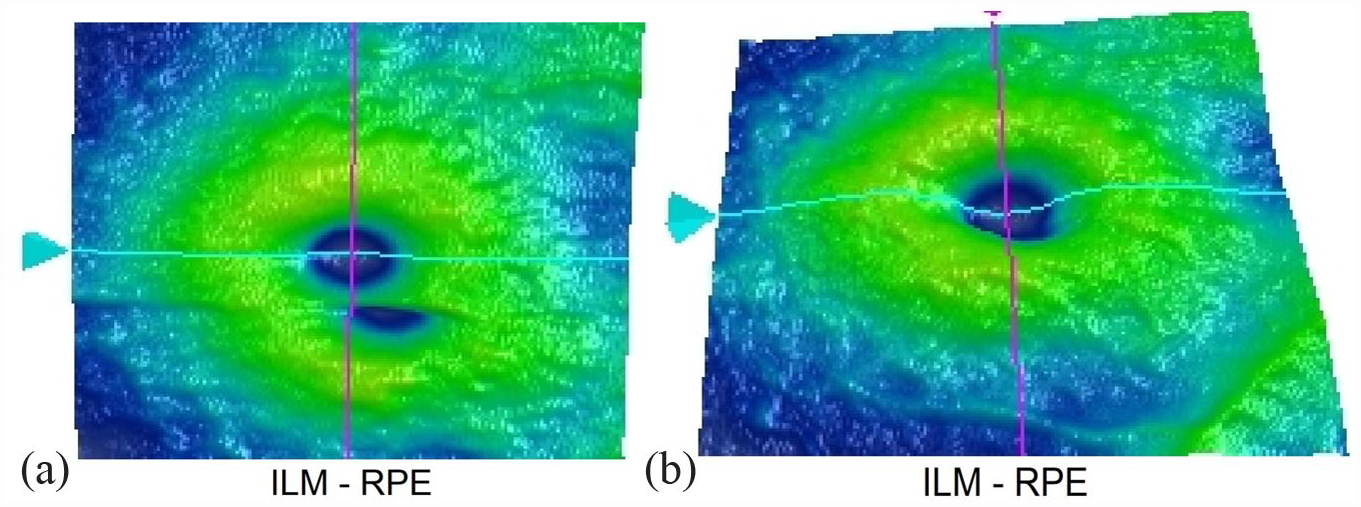
Enface OCT maps before and after pupillary dilation. (a and b) The comparative internal limiting membrane-retinal pigment epithelium (ILM-RPE) maps obtained with the Cirrus HD-OCT (version 5.0; Carl Zeiss Meditec Inc., Dublin, CA) machine before and after pupillary dilation, respectively. The double depression simulating the presence of two foveae on the map before dilation is no longer present after pupillary dilation.
Discussion
As a patient-related artifact, foveal duplication artifact is caused by motion artifact from the eye’s transient upward micro saccade movement, which produces an additional image of the fovea in the downward and then central re-fixation, resulting in a clear double fovea in the OCT image of the same eye. A few cases of foveal pseudo duplication have been reported in scientific literature.4–6 The scans were all acquired after adequate pupillary dilation on the Cirrus® OCT machine, which was a feature shared by the previously reported cases. The foveal duplication artifacts in previous reports were primarily due to poor fixation, which was corrected after repeating the OCT scans with adequate patient fixation. Motion artifacts can be corrected by improving OCT scanning speed and acquisition time, attempting multiple rescans if the motion artifact involves the scan circle, performing the scans on a device with an eye tracking system or motion correction algorithm, and achieving patient steady fixation by explaining the procedure in detail. 7 In our case, the foveal duplication artifact was corrected by repeating the scans through the same areas following adequate pupil dilation and by achieving steady fixation through proper patient counseling. In the presence of adequate pupillary dilation, the motion artifact score decreases significantly, allowing for images of higher quality with fewer artifacts.8,9
Conclusion
With an increase in the number of OCT scans performed under undilated pupillary conditions recently, the number of patient-related artifacts is expected to be high. This case demonstrates the importance of pupillary dilation and reimaging in the presence of unusual artifacts, such as foveal duplication, in order to prevent clinicians from ordering unnecessary additional tests.
Footnotes
Author contributions
ISA, RV—interpreting the findings, writing & reviewing the manuscript.
SK—clinical management.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This retrospective case report review of patient data/images did not require ethical approval in accordance with local/national guidelines.
Informed consent
Written informed consent was obtained from the patient for publication of the details of their medical case and any accompanying images.