
Abstract
Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids is a very rare entity which is considered as a treatable condition. In some cases, clinical and radiological findings, associated to favorable evolution on steroids therapy can be sufficiently distinguishable to diagnose chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids. We report the case of a 50-year-old man, suffering from acute dizziness with right facial paralysis and limited ocular abduction with his magnetic resonance imaging showing large confluent T2 and fluid-attenuated inversion recovery brainstem hyperintensities extending into the upper cervical spinal cord, infiltrating the basal ganglia and the thalami, with some punctate hyperintensities “peppering” the medial aspects of cerebellar hemispheres. This case illustrates atypical imaging features of chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids on magnetic resonance imaging and our work also reviews different studies in the literature and highlights the differential diagnosis.
Introduction
CLIPPERS is the acronym for chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids, which is a rare disorder first described by Pittock in 2010 as a distinct form of brainstem encephalitis, with only around 100 cases reported since then. 1 It has some specific clinical and radiological findings. Pittock et al. and Taieb et al. have proposed diagnostic criteria including neuropathological findings. However, even though brainstem biopsy may be an important tool for histologic CLIPPERS accuracy, it has dangerous potential complications (hemorrhage, intracranial hypertension, and edema) which limits its utility. CLIPPERS typically involves the perivascular regions of the brainstem and cerebellum infiltrated by lymphocytes. Magnetic resonance imaging (MRI) mainly shows typical pepper-like speckles in those regions associated to curvilinear enhancement which may extend to the spinal cord. It is treated with steroid hormones and the evolution is favorable.
Case
The patient, a 50-year-old male, was admitted to the hospital for severe acute dizziness. His medical history was unremarkable aside from heavy smoking and occasional alcoholism. The patient presented with paresthesia in both lower limbs and right esotropia accentuating on attempted abduction of the eye and on distance fixation. He was afebrile and his vitals were within normal limits. Clinical examination showed that the pupils were equal in diameter and sensitive to light. Diffuse limb weakness (3 + throughout) was noted with present tendon reflexes. An inability to abduct the right eye was noted with incomitant esotropia. The deviation was greater at distance fixation than at near, and also greater on attempted abduction of the right eye. These signs concurred with right abducens nerve palsy. The face was flat and expressionless on the right side with limited ability to wrinkle the forehead and blink. In conclusion, clinically, it was a 50-year-old patient suffering from dizziness, with right facial nerve and abducens nerve palsies associated to paresthesia.
Hence, cerebral MRI without and after contrast administration was judged necessary. It showed an important brainstem extensive edema with abnormal fluid-attenuated inversion recovery (FLAIR) signal hyperintensities with a “pepper-like” appearance involving the brainstem, predominantly the pons and extending to the middle cerebellar peduncle, to basal ganglia, thalami, and supratentorial white matter (Figure 1).

(a) Axial T2 and (b, c, and d) 3D FLAIR images showing large confluent hyperintensities in the middle stem, pons extending into the upper cervical spinal cord (red arrows). It infiltrates the basal ganglia and the thalami, with some punctate hyperintensities “peppering” the medial aspects of cerebellar hemispheres.
Post-contrast sequences (Figure 2) showed multiple associated patchy spot-like and curvilinear areas of enhancement “peppering” the pons. Those abnormalities were associated to a longitudinally extensive area of T2 increased signal extending from the brainstem to the cervical spinal cord. Curvilinear restricted diffusion areas were found on diffusion-weighted images and multiple hemorrhagic foci in the affected areas were identified on susceptibility weighted imaging (SWI) sequences (Figure 3).

T1 FAT SAT with gadolinium injection shows punctate and curvilinear foci of contrast enhancement. Note extension into supratentorial paraventricular white matter (red arrow).

(a) Axial SWI MIP shows multiple hemorrhagic foci in the middle brain. (b) and (c) Diffusion-weighted sequences with apparent diffusion coefficient (ADC) cartography showing scattered curvilinear restricted diffusion areas (arrows).
The diagnosis of CLIPPERS was suspected and high-dose steroid treatment was initiated, with the patient showing a spectacular clinical improvement after 10 days. Paresthesia slowly disappeared and the cranial nerves palsies. Unfortunately, the patient did not show up for his follow-up MRI.
Discussion
CLIPPERS syndrome is considered as a rare chronic inflammatory disease of the central nervous system (CNS) which was first described in 2010 by Pittock et al. 2 It is a rhombencephalitis which means the involvement of the hindbrain (brainstem and cerebellum). Histopathologically, it is characterized by a marked T cell predominant lymphocytic perivascular inflammation with possible association to white matter, gray matter, and meninges involvement. 3
It has been reported that the average onset age was of 40–50 years, but many cases were seen in a wider range (13–86 years) with a slight male predilection. 4
Typically, the clinical presentation tends to have subacute onset and progressive aggravation with a wide variety of symptoms, such as cranial nerve dysfunction represented mainly by dysarthria, altered facial sensation, and diplopia. Other signs such as cerebellar signs (e.g. ataxia) or long-tract signs, such as spasticity and altered sensation, may also be present. 5
It can also be accompanied by other non-specific symptoms, such as dizziness, nausea, vomiting, and dysphagia, and spinal cord syndromes can be seen in some patients. However, patients generally remain cognitively intact and do not suffer from other signs of inflammation, such as fevers or meningism.
Enhanced brain MRI is considered as the main imaging modality. Its manifestations include multifocal T2 and FLAIR hyperintensities with punctate or curvilinear enhancement on T1 after gadolinium administration “peppering” the pons and cerebellum. Occasionally, we may have lesions in the midbrain, basal ganglia, and the thalami, cerebral hemispheres, cranial nerves, and spinal cord. 6 In the acute phase, we may also have foci of restricted diffusion with punctate microbleeds in the affected areas on T2* or SWI sequences sometimes identified, which was the case with our patient. However, those are very atypical MRI findings that have been recently reported.7,8 It is important to note the mention by some authors a geographic gradient of lesser inflammation with increasing distance from the brainstem and cerebellum. 9
The imaging features of CLIPPERS can be string striking; however, a relatively wide differential should be considered including tumors (such as CNS lymphoma and brainstem glioma), infective especially entities causing rhombencephalitis-like Listeria rhombencephalitis and tuberculous rhombencephalitis. It also includes paraneoplastic and inflammatory diseases (mainly represented by Bickerstaff brainstem encephalitis, CNS vasculitides, and neurosarcoidosis), and demyelinating pathologies, such as multiple sclerosis (MS), neuromyelitis optica (NMO), and acute disseminated encephalomyelitis (ADEM) (Table 1).

We should also note that CLIPPERS can be considered as a pre-lymphoma state. This was first reported in 2011 by Limousin et al. 13 with clinical manifestation of CLIPPERS later being diagnosed as being type B primary CNS lymphoma. This was followed by many other cases of CLIPPERS with lymphoma. 14 It is true that neoplastic etiologies are of great concern, that is why we should pay big attention to the exclusion strategy of diagnosing CLIPPERS. 4
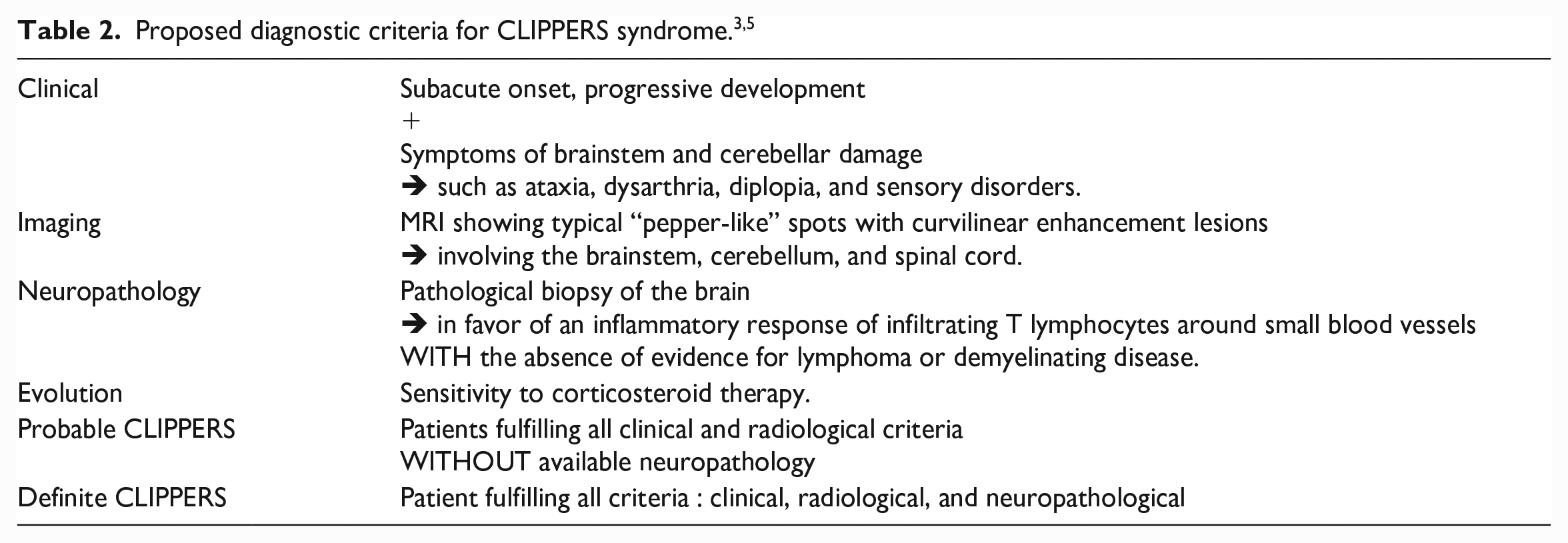
To sum-up, CLIPPERS had been defined by some authors as the combination of clinical, radiological, and pathological criteria, with the later findings being essential for the definite diagnosis; however, biopsy must be limited to patients where another pathology is strongly suspected and other differential diagnosis must be eliminated.3,13,15 Consequently, the term of “probable CLIPPERS” has been introduced, based on the association of clinical and radiological findings when neuropathology is not available, as was our case (Table 2).
A large dose of glucocorticosteroids (GCSs) is considered as the main treatment with spectacular response supporting the diagnosis. Some studies have compared patient’s MRI enhancements with CLIPPERS syndrome before and after treatment which indicated that « pepper-like » signs decreased or disappeared. 5 In addition, trials of immunoglobulin have been reported in the literature, but this protocol may not be effective and remains to be further explored. 16 Some studies have also reported that hydroxychloroquine can be used to treat CLIPPERS syndrome, and not only leads to rapid remission but also effectively prevents recurrence with less adverse reactions. 17
Conclusion
CLIPPERS syndrome remains a controversial nosological entity due to its non-specific focal neurological signs. It can be diagnosed initially as a multitude of other neurological pathologies. Thus, we recommend keeping it as a diagnosis of exclusion, especially when no other definitive diagnosis can be reached. Recent diagnostic criteria can be useful to carry out diagnostic confidence, especially with the presence of “pepper-like” speckles and curvilinear enhancements associated to spectacular improvement after GCs. Biopsy should therefore be limited to cases where alternative diagnoses are strongly suspected. Efforts to answer whether CLIPPERS syndrome is possibly an autoimmune or a systemic disease due to its relapsing and remitting evolution can be an important milestone in learning additionally about its pathogenesis.
Footnotes
Author contributions
Y.E.H. was responsible for article concept, design, and editing and literature search. S.C. helped in article editing and literature search, article editing and article review. K.B. contributed to conception and design. N.E-C.K. contributed to acquisition, analysis, and interpretation. M.F. contributed to acquisition, analysis, and interpretation. M.J. critically revised the article and gave final approval. F.T. contributed to acquisition, analysis, and interpretation; critically revised the article and gave final approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.