
Abstract
Wheat-dependent exercise-induced anaphylaxis is a rare but severe form of anaphylaxis that occurs after consuming wheat products and engaging in physical activity. A case study of a 30-year-old woman suffering from chronic urticaria for the last 5 years highlights the difficulty in diagnosing this condition, as specific triggers were not identified. A diagnostic study called MADx revealed a positive analysis for omega-5-gliadin, leading to a diagnosis of wheat-dependent exercise-induced anaphylaxis. Delayed diagnosis is a common issue, and it can be challenging to distinguish wheat-dependent exercise-induced anaphylaxis from other conditions with similar symptoms. The treatment involves avoiding wheat products and always carrying an epinephrine auto-injector. When evaluating patients with similar symptoms, healthcare providers should include wheat-dependent exercise-induced anaphylaxis in their differential diagnosis. Patients should be educated about the symptoms, triggers, and management to seek immediate medical attention in an emergency.
Keywords
Introduction
Wheat-dependent exercise-induced anaphylaxis (WDEIA) is an uncommon food allergy that can lead to severe anaphylactic reactions, including respiratory, gastrointestinal, cardiovascular, or urticarial symptoms. The reactions typically occur 1–4 h after consuming wheat, followed by physical exercise. 1 According to an anaphylaxis registry in Europe, individuals experiencing anaphylaxis due to wheat were found to exhibit more severe symptoms (odds ratio of 4.3) and a greater incidence of severe cardiovascular symptoms (87%) compared to other food allergies. 2 The omega-5 gliadin protein found in wheat is crucial in causing WDEIA. Other factors such as alcohol, aspirin, stress, infections, and female sex hormones/menstruation can trigger an immediate hypersensitivity reaction in combination with exercise. 3 Currently, there are no universally accepted protocols for treating patients suffering from WDEIA. 4 A study conducted with a short-term follow-up period5,6 has shown that anaphylaxis can be effectively prevented in nearly all patients with WDEIA by abstaining from wheat consumption in combination with the avoidance of other potential triggering factors or by adhering to diet that is free of wheat.
Case report
The patient is a 30-year-old woman who has experienced chronic spontaneous urticaria for the last 5 years. He could not identify any specific cause and received new-generation antihistamines and systemic corticosteroids several times a month to manage his symptoms. See Table 1 for the test results obtained during the first visit. According to the manufacturer’s instructions, total IgE levels, sIgE and serum Tryptase were measured using the ImmunoCAP system (Thermo-Fisher, Uppsala, Sweden). However, 2 months ago, while commuting to work, she experienced an episode of itching, restlessness, and loss of consciousness. She was immediately taken to the emergency room, received first aid, and was discharged after 12 h of observation. According to the patient, before leaving home, she had breakfast, which included bread and other wheat products. During this period, she did not take non-steroidal anti-inflammatory drugs, had no signs of infection, and had no menstrual period. Following the episode, the patient underwent a diagnostic study called multiplex component-based allergen microarray test (MADx), which revealed a positive analysis for omega-5-gliadin (Table 2). The highest measured IgE concentration per allergen group is as follows: <0.3 kUA/L (negative or uncertain), 0.3–1 kUA/L (low IgE level), 1–5 kUA/L (moderate IgE level), 5–15 kUA/L (high IgE level), and >15 kUA/L (very-high IgE level). There is no clinical relevance for other positive allergens. The patient did not perform skin prick tests because he often uses non-sedating new-generation anti-histamine drugs due to chronic urticaria. Based on these findings, the patient has been diagnosed with WDEIA. After the mentioned episode, the patient is on a gluten-free diet, during which no episode of anaphylaxis occurred. Chronic spontaneous urticaria episodes persist, urticaria control test (UCT) result at last visit was 12 (UCT > 12 is considered disease controlled).
Test result from ImmunoCAP, 2019.

Positive test result from MADx, 2022.
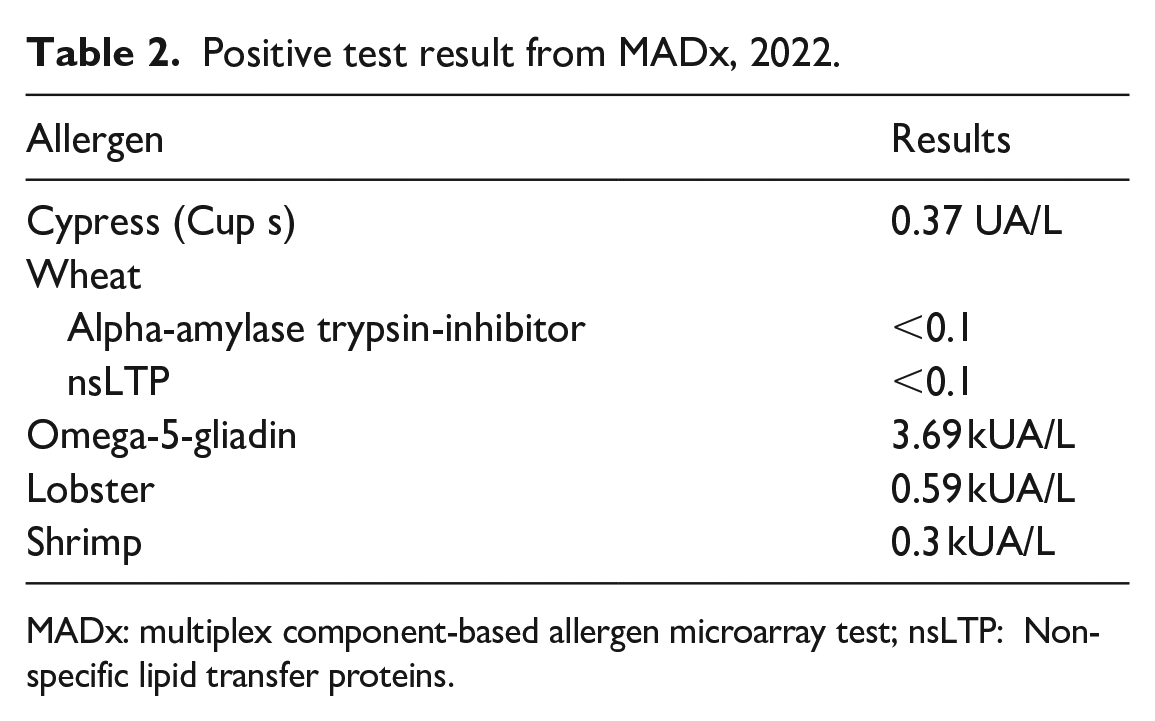
MADx: multiplex component-based allergen microarray test; nsLTP: Non-specific lipid transfer proteins.
Discussion
WDEIA is a rare form of anaphylaxis after consuming wheat products and engaging in physical activity. It is caused by an IgE-mediated reaction to wheat proteins, specifically omega-5-gliadin. The symptoms can be severe, ranging from urticaria, angioedema, and gastrointestinal symptoms to hypotension and loss of consciousness. 7 In our case, the patient had been suffering from chronic urticaria for the last 5 years, which could have been an early sign of her allergy to wheat. However, the absence of specific triggers made it challenging to diagnose.
Diagnosing WDEIA has long been challenging. 8 The delay time of diagnosis was different between studies. In a study by Wong et al., 9 the average time for WDEIA to be diagnosed was 28.5 (2–62) months. Half of the patients had a delay of 32–62 months before diagnosis. Meanwhile, in Kennard et al.’s 4 retrospective study of 132 patients with WDEIA in four UK centres, 66.7% of patients had a delay in diagnosis of >1 year, including 40% of patients with a delay in diagnosis of 1–5 years and 29% with a delay in diagnosis of >5 years. In our case, the delay in diagnosis was 36 months.
The delay in diagnosis can be attributed to the fact that in our country, there is no auto-injector adrenaline available, but dexamethasone and other steroids are sold without a prescription. Patients with allergies (urticaria, angioedema, drug allergy, and insect bite allergy) will most likely take one steroid dose with them. Therefore, when symptoms appear, it is used immediately. The above circumstance explains why detecting the diagnosis in such a situation was difficult beforehand.
The studies results indicate that 6.8% of patients with recurrent urticaria were allergic to wheat, and they had a potential risk of WIA/WDEIA. This highlights the importance of examining patients with recurrent urticaria for wheat allergy. Identifying wheat allergy patients when they manifest as recurrent urticaria and giving appropriate education is helpful to prevent severe allergic attacks. 10
In some cases of WDEIA, it may not be possible to demonstrate sensitization to the full food allergen source (eg, wheat extract or native wheat) but only to molecular allergens (eg, omega-5-gliadin, Tria19) or gluten. In the study of 17 German patients with WDEIA mentioned previously, 82% had IgE to omega-5 gliadin, although other allergens (alpha, beta, and gamma gliadins or lipid transfer protein Tri a14) might be also important, as demonstrated with experimental assays. 11
During the WDEIA evaluation, it is necessary to conduct tests of high precision and sensitivity. According to some studies, standard wheat skin prick tests were much less accurate than specific immunoglobulin determinations for omega-5-gliadin. 12 In our case, it is interesting that the specific immunoglobulin IgE for the food mixture (milk, egg, wheat, peanut, soy, fish mixture) performed on the first visit was negative, and the molecular diagnostics performed after the reaction allowed us to verify the nature of the response. In case of chronic spontaneous urticaria, omega-5-gliadin test is not recommended according to international guidelines. However, its early detection during multicomponent tests can prevent serious complications.
Treatment for wheat-dependent exercise-induced anaphylaxis involves avoiding wheat products and using epinephrine in case of anaphylactic reactions. 13 In our case, the patient was given appropriate recommendations, including a wheat-free diet and always carrying an epinephrine auto-injector. The patient was also advised to wear a medical alert bracelet to inform others of her condition in an emergency. It is essential to spread awareness of this condition and educate patients and healthcare providers about the symptoms, triggers, and management. Patients should be advised to seek immediate medical attention if they experience symptoms after consuming wheat products and engaging in physical activity.
The main point of our case is that a patient can have chronic urticaria, be negative for specific IgE to wheat, and at the same time have a positive test for omega-5-gliadin. Therefore, implementing a wide range of component-resolved diagnostics (CRD) in practice allows avoiding such complications.
The limitation of the study is that no provocation test was conducted, it was difficult for the patient to agree to the mentioned procedure.
Conclusion
WDEIA is a rare but potentially life-threatening condition that can be challenging to diagnose. Testing for sIgE to omega-5-gliadin should be considered in patients with exercise-induced urticaria/anaphylaxis, idiopathic anaphylaxis, and recurrent acute urticaria. Early diagnosis and appropriate management can prevent severe and fatal outcomes. Healthcare providers should be aware of this condition and include it in their differential diagnosis when evaluating patients with similar symptoms.
Footnotes
Acknowledgements
The author(s) do not have any acknowledgement to report for this manuscript.
Author contributions
B.K. contributed to the data collection, manuscript writing, revision editing, final manuscript review and production, and approved the final version. M.G contributed to the final manuscript review and production and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.