
Abstract
Segmental Darier’s disease is an uncommon subtype of Darier’s genodermatosis, resulting from a mutation in the ATPase type 2 during early embryogenesis. It typically presents as a persistent, pruritic papular eruption following the lines of Blaschko. Histopathology of Darier’s disease demonstrates acantholysis, dyskeratosis, and corps ronds. First-line treatment includes topical retinoids, calcineurin inhibitors, and synthetic vitamin D analogues. Severe disease may require systemic therapy with oral retinoids, immunomodulators, magnesium, and low-dose naltrexone. Segmental Darier’s disease is important to recognize both clinically and histologically as it may resemble other acantholytic Blaschkolinear dermatoses and should be considered in individuals presenting with a chronic localized papular eruption in a Blaschkoid distribution. Herein, we present a case of a 48-year-old male with segmental Darier’s disease who improved significantly following acitretin treatment.
Introduction
Darier’s disease (DD), also known as keratosis follicularis, is a rare genetic acantholytic dermatosis that is inherited in an autosomal dominant pattern with high penetrance but variable expression. 1 It is caused by a mutation in the ATPase type 2 (ATP2A2) gene in keratinocytes, which results in loss of intercellular adhesion and subsequent acantholysis.2,3 Its prevalence ranges from 1 in 30,000 to 1 in 100,000 in the general population and affects males and females equally, and typically presents in the second or third decade. 4 DD most commonly presents as pruritic, generalized, symmetrical keratotic papules and plaques with a predication for the seborrheic and intertriginous areas of the body. In skin of color, Darier’s may present as hypopigmented macules in a perifollicular distribution. 5 Furthermore, a minor subset of patients with DD present with localized lesions, including the segmental subtype. On histology, DD typically demonstrates acantholysis with suprabasal cleavage, dyskeratotic keratinocytes, corps ronds, and grains. DD can be complicated by superinfections, such as by herpes simplex virus, which carry significant morbidity and mortality. 6 DD can have a significant impact on patients’ quality of life by negatively affecting self-esteem and social relationships. 7 Studies have also demonstrated a potential comorbidity of DD with neuropsychiatric disorders.8,9
Case report
A 48-year-old male presents with a several years history of a recurrent and pruritic right-sided papular eruption on his body. The eruption first developed following injury during military service in Afghanistan. It flares with stress, during which the eruption appears vesicular, erythematous, and is painful and significantly pruritic. Between the flares, he has a baseline erythematous, mildly pruritic rash that lasts 4–5 months post-flare. On physical examination, the patient had Fitzpatrick phototype II skin, and erosive pink papules forming curvilinear plaques following the lines of Blaschko were noted (Figure 1). No mucosal, acral, or palmoplantar involvement was noted. His past medical history is significant for Celiac disease (on gluten-free diet with negative duodenum biopsies), hemochromatosis (receives regular phlebotomies), and degenerative disc disease. There is no known family history of similar rashes or autoimmune disease. His medications include medical cannabis, nortriptyline, and trazodone. He is a former smoker with a 10 pack-year history and does not consume alcohol or illicit drugs.
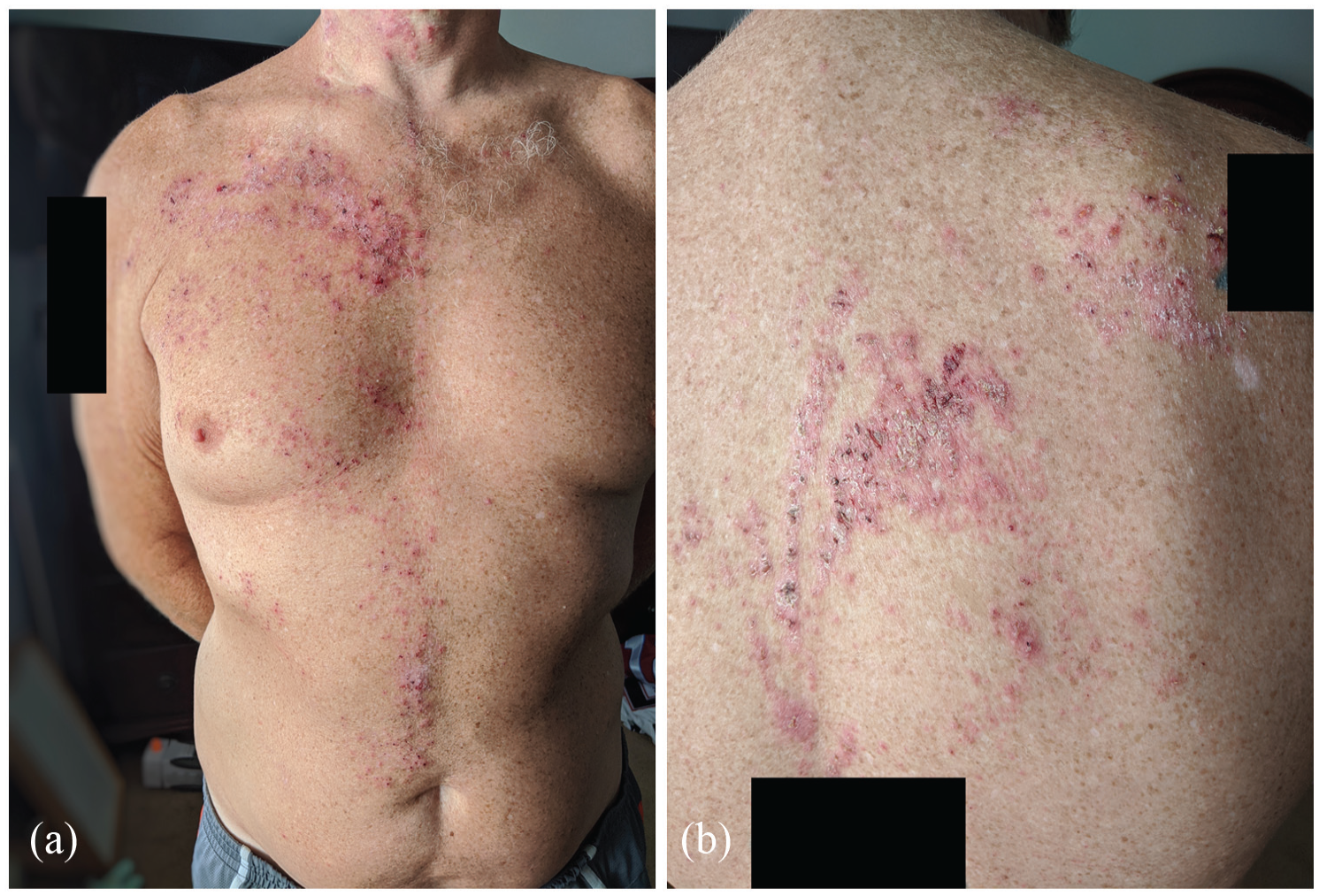
(a) Over the right anterior shoulder, chest, and abdomen, there are clustered pink papules with areas of excoriation, forming curvilinear plaques following the lines of Blaschko. (b) Over the posterior upper back, pink papules clustering in plaques in a Blaschkoid distribution are noted.
Punch biopsies of lesional and perilesional skin on his abdomen were taken and sent for hematoxylin and eosin and direct immunofluorescent staining (DIF), respectively. Histologic examination demonstrated intraepidermal acantholytic dermatosis with corps ronds and dyskeratotic keratinocytes. There was no viral cytopathic effect to suggest herpes zoster. The histologic pattern did not suggest dermatitis herpetiformis. DIF staining was negative for IgG, IgA, IgM, and C3.
Prior to investigations, he was diagnosed with refractory herpes zoster and was treated with topical betamethasone valerate 0.1% with no improvement. Following the diagnosis, the patient was prescribed acitretin 10 mg PO OD alternating with 20 mg PO OD daily with good effect, which was stepped down to 10 mg PO twice a week. Skin hygiene measures, that is, cotton clothing, emollients, and sunscreen, were also undertaken. He had a complete and sustained remission of his rash a few weeks later and at 2 years of follow-up.
Discussion
Segmental DD is an uncommon entity, described as a genetic mosaic of DD, with approximately 40 cases documented in the literature to date. It is divided into two main types: type 1 and type 2. 10 Type 1 results from a postzygotic, somatic mutation in the ATP2A2 gene resulting in unilateral, and localized eruptions. On the contrary, type 2 results from a germline mutation in the ATP2A2 gene in addition to a postzygotic mutation in its other allele, leading to localized areas of increased severity in the context of milder, generalized DD. Segmental DD typically manifests as a unilateral eruption of erythematous and keratotic vesicles and papules that follow the lines of Blaschko. Patients with segmental DD tend to present later in life (fourth or fifth decade of life); have no other DD features such as mucosal, nail, or acral involvement; and have no family history. If the genetic mosaicism involves the gonads, there is a theoretical potential for resultant generalized disease in offspring. The differential diagnosis of segmental DD includes Grover’s disease (which tends to be transient), Hailey-Hailey (predominately intertriginous), and autoimmune pemphigus. One study demonstrated the utility of dermoscopic examination in diagnosing DD (including the segmental subtype), whereby the papules display a centrally located yellow-brown polygonal area surrounded by a thin white halo. 11
Treatment of DD involves vitamin A derivatives such as topical and oral retinoids to increase cell turnover, which is thought to be slowed in DD. 12 Antiseptic topical agents may be useful in preventing bacterial colonization and secondary infections. Other therapies are limited, but include topical calcineurin inhibitors, topical synthetic vitamin D analogues, trials of oral corticosteroids, cyclosporin, oral magnesium, and low-dose naltrexone. 13 Topical 5-fluorouracil has also been shown to be effective in DD, albeit with variable success. In addition, adjunctive therapies with dermabrasion, CO2 and Er-YAG lasers, and surgical excision may also be offered to patients, though with caution in skin of color. 13
Our patient presented with a recurrent Blaschkoid eruption of erythematous papules to the right side of his body. His clinical presentation and associated histopathological findings are most consistent with type 1 segmental DD. Given that patients with DD may be at higher risk of developing neuropsychiatric conditions, 8 regular monitoring of mood symptoms, especially for patients started on oral retinoid therapy, may be beneficial. Certain medications such as azathioprine, lithium, and calcium antagonists may worsen the disease. 10 Avoidance of known DD triggers, including ultraviolet light exposure, heat, or friction, is also recommended.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Patient gave consent for their photographs and medical information to be published in print and online and with the understanding that this information may be publicly available.