
Abstract
This report discusses a case of linear and whorled nevoid hypermelanosis associated with cerebellar atrophy, ocular and developmental anomalies compatible with Joubert syndrome. Linear and whorled nevoid hypermelanosis is a rare disorder of skin pigmentation characterized by swirls and whorls of hyperpigmented macules in a reticulate pattern along Blaschko’s lines. Neurologic, cardiac, skeletal and developmental anomalies have been reported. We present a case of linear and whorled nevoid hypermelanosis on an 18-year-old woman who also presented with cerebellar atrophy, jerk nystagmus, macrocephaly and developmental delay. Those symptoms were compatible with Joubert syndrome. A complete work-up failed to reveal other systemic or skeletal anomalies. No chromosomal alteration was found on karyotyping carried out on a skin specimen. Much remains to be known about linear and whorled nevoid hypermelanosis. It is generally a benign condition but association with various congenital anomalies have been reported. Proper work-up is advised in order to exclude congenital anomalies.
Keywords
Introduction
Linear and whorled nevoid hypermelanosis (LWNH) is a rare disorder of skin pigmentation characterized by swirls and whorls of hyperpigmented macules in a reticulate pattern along Blaschko’s lines. 1 Neurologic, cardiac, skeletal and developmental anomalies have been reported. 2
Our primary objective is to present and discuss a case of LWNH associated with cerebellar atrophy as well as ocular and developmental anomalies compatible with Joubert syndrome. To our knowledge, association of LWNH with Joubert syndrome has rarely been described. Our secondary endpoint is to discuss reported systemic associations and devise a proper work-up in order to exclude congenital anomalies.
Case report
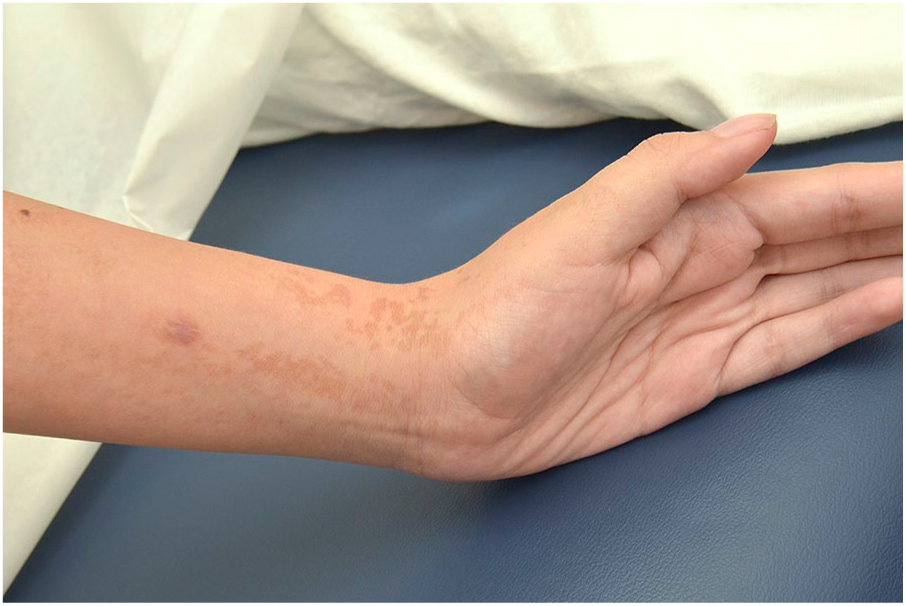
An 18-year-old woman presented with asymptomatic linear and reticular hyperpigmentation on upper and lower limbs following Blaschko’s lines (Figures 1–3). Lesions appeared shortly after birth and did not change throughout the years. Mucosae, palms, soles and skin appendages were unaffected. Parents denied any history of vesicular lesions at birth or similar pigmented lesions on other members of the family. There was no history of verrucous or hypopigmented lesions. Five café-au-lait macules were also found on physical examination. Cutaneous and systemic investigation did not show any other classical sign of neurofibromatosis.

Linear and whorled hyperpigmented macules on patient’s leg.
Linear and whorled hyperpigmented macules on patient’s left arm.

Linear and whorled hyperpigmented macules on patient’s right arm.
The patient also presented with cerebellar atrophy, jerk nystagmus, macrocephaly and developmental delay. Those symptoms were compatible with Joubert syndrome, an autosomal recessive disorder caused by mutations related to cell structures called primary cilia.3,4 Comparative genomic hybridization carried out on blood sample had failed to show differences in DNA sequence and number.
A complete work-up failed to reveal other systemic or skeletal anomalies. Family history revealed consanguinity between the parents. No chromosomal alteration was found on karyotyping carried out on a skin specimen.
Discussion
LWNH is a rare disorder of skin pigmentation characterized by swirls and whorls of hyperpigmented macules in a reticulate pattern along Blaschko’s lines. Lesions usually appear within a few weeks from birth and rapidly stabilize within the first 2 years of life. 5 A late-onset form has also been described.6,7
LWNH must be differentiated from many pigmentary disorders. Incontinentia pigmenti presents with a vesicular and verrucous stage prior to the pigmentary appearance. 8 Hypomelanosis of Ito is a sporadic skin condition involving the central nervous system, eyes, and musculoskeletal system. Its main cutaneous feature is hypopigmented blaschkoid lesions, the reverse of LWNH. 9 In an extensive presentation, it may be difficult to determine if the abnormality is the hypopigmentation or the hyperpigmentation and both conditions are sometimes called pigmentary mosaicism. 5 Epidermal nevi differs from LWNH because of its hyperkeratotic plaques. 1 Mosaicism can be ruled out by karyotype. 9
LWNH has been reported as a sporadic occurrence, although there has been one reported case of an affected mother and daughter. 10 In some cases, underlying chromosomal mosaicism and cytogenetic changes have been observed such as trisomy 7, 14, 18, 20 and X-chromosomal mosaicism.1,2,11 A postzygotic mutation in KITLG gene was also identified. 8 The latter is associated with increased KITLG and c-KIT epidermal expression. 8
LWNH may be associated with extracutaneous abnormalities including central nervous system diseases, cardiac defects, psychomotor delay, deafness, brachydactyly and hydrocephalus. 2 The true incidence of such associated systemic features is unknown but some studies have reported a rate between 16% and 31%. 5
Because of possible association with various congenital anomalies, LWNH patients should be thoroughly investigated. 1 Neurodevelopmental and psychomotor development should be closely monitored, as well as limb measurement and head circumference. Ophthalmic and audiologic evaluation should be carried out. Cerebral and heart imaging could be advised upon diagnosis or following symptomatology (Table 1).
Suggested investigation for LWNH.
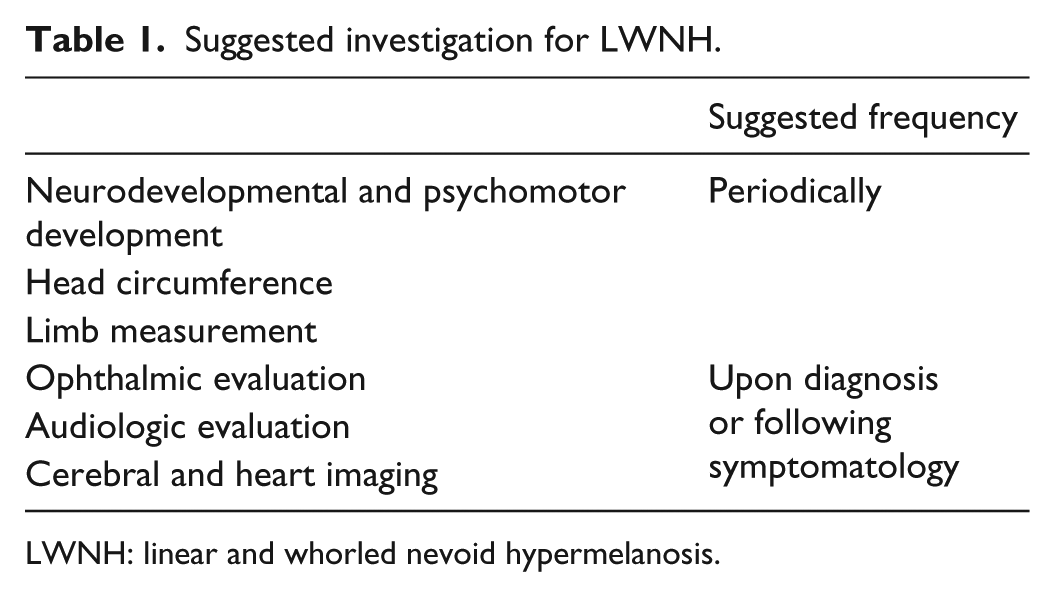
LWNH: linear and whorled nevoid hypermelanosis.
Much remains to be known about LWNH. It is generally a benign condition but association with various congenital anomalies has been reported. To our knowledge, association of LWNH with Joubert syndrome has rarely been described. Proper work-up is advised in order to exclude congenital anomalies.
Footnotes
Authors’ note
This paper was presented as a poster at the Canadian Dermatology Association Conference (June 2019).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patient provided signed informed consent for publication of the case report and images.