
Abstract
The common carotid artery bifurcates into two terminal branches—the external and internal carotid arteries. The head, neck, and face regions principally get their blood supply from the external carotid artery and its branches. Some previous articles have mentioned the abnormal pattern of the external carotid artery branching and its variable origin. In this article, a rare case has been documented, having the combination of anomalies of the high carotid termination and bilateral variable origin of the ventral branches of the external carotid artery encountered during routine dissection of the head and neck region of a 55-year-old male cadaver in the Department of Anatomy. In this instance, on the right side of the neck, we observed the presence of a thyrolinguofacial trunk which arose from the ventral surface of the external carotid artery, and on the left side, the linguofacial trunk emerged from the ventral surface of the external carotid artery while the superior thyroid artery branched off directly from the left common carotid artery. This apart, there was bilateral high termination of the common carotid artery. Although the exact embryogenesis of such common arterial trunks anomalies and high carotid termination is not clear, detailed and precise anatomical knowledge of such a combination of anomalies will provide further insight for better radiological evaluation and to avert iatrogenic vascular injuries during any surgical procedures of the head and face region.
Introduction
The brachiocephalic trunk and arch of the aorta give rise to the right common carotid artery and the left common carotid artery, respectively. Normally, the CCA (common carotid artery) terminates into the external and internal carotid arteries at the superior border of the thyroid cartilage, which is at the intervertebral disk level between the third and fourth cervical vertebrae in the neck region. Usually, the arterial branches that arise from the ECA (external carotid artery) are the superior thyroid artery (STA), lingual artery (LA), and facial artery (FA) from its ventral surface, the occipital and posterior auricular arteries from its posterior surface, the ascending pharyngeal artery from its medial surface, and the maxillary and superficial temporal arteries as its terminal branches. 1 Previous articles have documented some common origins of ventral branches of ECA such as linguofacial trunk (LFT), thyrolingual trunk (TLT), and thyrolinguofacial trunk (TLFT). 2
The ECA and its different branches nourish the head, neck, and face areas. The various branches of the ECA have crucial collateral anastomoses with the vertebral artery and the internal carotid artery (ICA), thus establishing proper cerebral blood flow during obstruction of other great vessels in this region. Before the operative procedure, the concerned consultants must be familiar with the common and uncommon anatomical features of the CCA and its branches otherwise faulty ligation of the ICA can lead to hemiparesis. 3 However, it is also very crucial for surgeons to have a profound and precise knowledge of usual and anomalous anatomical details of the STA, LA, and FA when ligating the vessels during thyroidectomy, laryngectomy, oral and faciomaxillary surgeries, tonsillectomy, glossectomy, cosmetic surgery of the face, surgical emergencies, radical neck resection, arterial angiogram before the operative procedure for better understanding of the exact location, and spread of orofacial malignancies, as the ligation of the wrong artery can lead to grave consequences. The updated knowledge of anatomical variations of different branches of the ECA is also very useful for correct preoperative radiological evaluation that would provide prior inputs to the surgeons. 4
Case report
During a routine undergraduate dissection class of the neck region of a cadaver of a 55-year-old male, we observed high termination of the CCA into the ECA and the ICA, corresponding to the greater horn of the hyoid bone anterior and the body of the C3 vertebra posterior. In the same cadaveric specimen, we also found a common arterial trunk TLFT on the right side and an LFT on the left side, that emerged from the ventral surface of the ECA above the carotid termination. On the left side, the STA arose from the ventral surface of the CCA (Figures 1 and 2).

(a) Photographic illustration of the superficial dissection of the right side of the neck showing TLFT and high carotid bifurcation (at the level of the hyoid bone). The TLFT arising from the right ECA. The common TLFT was divided to give origin to STA and LFT. The LFT further branched off to LA and FA. (b) Schematic representation of Figure 2(a).

(a) Photographic illustration of the superficial dissection of the left side of the neck showing LFT and high carotid bifurcation (at the level of the hyoid bone). The LFT arising from the left ECA. The common LFT gave origin to LA and FA. The STA originated from the left CCA. (b) Schematic representation of Figure 2(a).
The anatomical details of the ventral branches of the ECA were explored carefully by meticulous dissection and took digital photos of the rare bilateral variations (right side TLFT and left side LFT trunk). The morphometric details of the TLFT and LFT were calculated with the use of a digital vernier caliper. At the time of measurement, no manual force had been applied to the arteries and its anatomical pattern was maintained. The diameters of the arteries/common arterial trunks were determined 2 mm from their origin. 5
In this cadaveric specimen, the TLFT was the first branch that arose about 4.6 mm above the carotid termination from the ventral surface of the right ECA. The length of the TLFT was 2.1 mm. After giving the STA, this trunk coursed upward, anteriorly, and medially about 11 mm as the LFT and terminated into the LA and FA above the greater cornu of the hyoid bone in the submandibular region. The FA followed the tortuous course through the submandibular region onto the face. The LA showed its characteristic loop pattern and passed medially to enter the sublingual space. The diameter of the TLFT, LFT, STA, LA, and FA was 4.3, 3.5, 1.4, 1.9, and 2.8 mm, respectively. The hypoglossal nerve crossed superficially the linguofacial trunk just below its bifurcation. The right ascending pharyngeal artery was the second branch that originated medially from the ECA just above the TLFT. The other branches of the right ECA had their normal anatomical origin and course (Figure 1 and Tables 1 and 2).
The morphometric details of the TLFT and LFT.

TLFT: thyrolinguofacial trunk; LFT: linguofacial trunk; CB: carotid bifurcation.
The measurement details of the diameter of STA, LA, and FA.
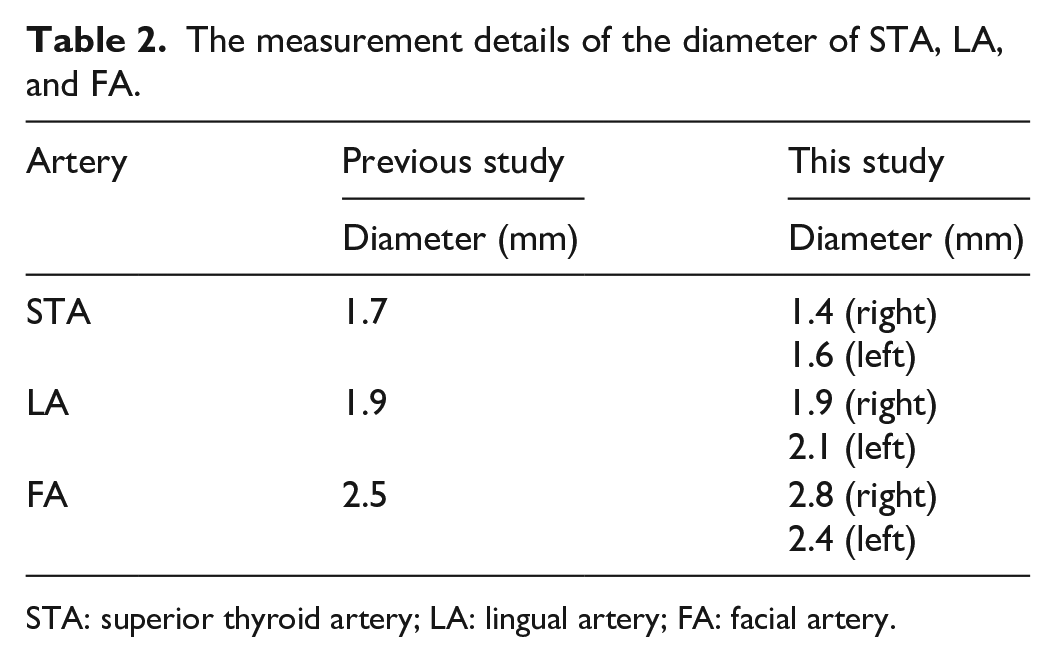
STA: superior thyroid artery; LA: lingual artery; FA: facial artery.
On the left side, the LA and FA arose as the common LFT from the ventral surface of the ECA about 17.4 mm above the carotid bifurcation (CB) and coursed upward toward the mandible for about 7.6 mm and then divided into FA and LA above the greater cornu of the hyoid bone. The hypoglossal nerve was crossing the linguofacial trunk superficially just below its bifurcation. The diameter of the LFT, LA, and FA was recorded as 3.2, 2.1, and 2.4 mm, respectively. The LA, immediately after its origin, took a downward loop, the convexity of which faced downward. Then, it coursed forward and medially to supply the tongue musculature. The FA was directed upward and forward to reach the facial region. Further course and branching of the FA were of the usual pattern. The left STA originated 2.5 mm below the CB from the CCA and supplied the upper pole of the thyroid gland. The diameter of the STA was 1.6 mm. The left ascending pharyngeal artery was the first branch that arose from the medial side of ECA just above the bifurcation of the CCA. The anatomical origin and courses of other branches of the left ECA were normal (Figure 2 and Tables 1 and 2).
We performed the morphometric study of these rare common arterial trunks and ventral branches of the ECA as well.
Discussion
In the present case, we observed, a rare combination of anomalies in the form of bilateral high CCA termination, the emergence of TLFT and LFT from the ventral surfaces of the right and left ECA, respectively, and the left STA from the left CCA. According to available data, there was no earlier documented literature on such a combination of anomalies. In our report, we have studied the variations and morphometric characteristics of these branches considering the importance of their surgical and imaging points of view. The CCA normally terminates at the level of the upper border of thyroid cartilage (C3-C4 vertebral level). 1 Zümre et al. 6 studied 40 fetuses and mentioned the CCA termination at C3, C4, and C5 levels in 55%, 35%, and 10%, respectively, on the right side; while 60% at C3 and 40% at C4 vertebral level on the left side. In another study, carotid termination was mentioned as 2.7% in C2-C3, 10.4% in C3, 20.9% in C3/C4, 30.2% in C4, 16.3% in C4/C5, and 8.1% in C5 vertebral level. 7 The precise anatomical knowledge of the CCA termination is important to avert critical injury to the lower cranial nerves and other possible risks that may occur during carotid angiography, carotid body tumor removal, endarterectomy, and catheterization. 2
Zümre et al. 6 concluded from their study that LFT was found in 20% of cases, a TLT in 2.5%, and TLFT in 2.5% of the cases of the human fetuses studied. Baxla et al. 8 mentioned a single case of bilateral TLFT in a cadaver.
In this study, the STA arose from the TLFT on the right side and the CCA on the left side. Lo et al. 9 observed that the chances of the STA emerging from CCA have been increased when carotid termination was high. In the previous articles, the range of the arterial diameter of STA was mentioned as 1–3.5 mm and the distance of emergence was 2–10.5 mm when the STA arose from the ECA and 2–10.7 mm when came off from CCA. 10 In this study, the arterial diameter of STA measured was 1.6 and 1.8 mm on the right and left sides, respectively, and the distance was calculated at 2.4 mm when STA arose from CCA (Table 2). The STA is the most inconstant branch of the ECA and has immense clinical significance for surgeons and radiologists during thyroidectomy, tracheostomy, laryngectomy, supra-selective arterial drug therapy, and minute arterial implantation. 2
The FA usually arises from the ventral surface of the ECA above the origin of LA and just above the tip of the greater cornu of the hyoid bone. The distance between the origin of FA and carotid termination varies widely between 7.6 and 20.43 mm. In most of the studies, the LFT was found unilateral, but in some cases, it was mentioned as a bilateral variation. 11 The LA normally comes out from the ventral surface of the ECA between STA and FA. In the present case, the LA and the FA arose from LFT in the submandibular region on both sides. In the previous studies, it was well documented that the average length of LFT before division into LA and FA is measured at 9.4 ± 1.7 mm on the right side and 7.6 ± 1.3 mm on the left side, ranging from 4.3 to 11.4 mm. The distance of origin of LFT from CB ranges from 5 to 40 mm, and its diameter is around 2 mm (Table 1). Iwai et al. 12 mentioned the diameter of TLFT was 4.4 mm, the length of the trunk was 1.7 mm, and the distance from carotid termination was 1.6 mm.
The presence of the LFT, FA, and the LA in the submandibular triangle increases the possibility of misidentification of the LA during surgery. Extraoral ligation of the LA is an appropriate and effective procedure during certain surgical emergencies like maxillofacial trauma, intraoral tumor biopsy, after surgical excision, super-selective intra-arterial catheterization, or microsurgical reconstruction for head and neck cancer, and even after minor surgical procedures including tonsillectomy. Anomalous emergence of the LA from the LFT in the submandibular region can hamper the extraoral ligation of the LA during the above surgical emergencies and further add neurovascular complications. 5 Baik et al. 13 stated that LA and FA originating from the LFT are likely to be at greater risk of iatrogenic injury because they may reach very near to the tonsillar fossa. A better understanding of the variable origin and branching pattern of the LFT will avoid injury to the hypoglossal nerve which passes superficially and very close to its termination.
In a few reported cases, it was documented that the sublingual gland was supplied by FA instead of the LA and the submandibular gland got its blood supply directly from the ECA in place of the FA. Hence, the surgeon must take cognizance of these anomalous branches during surgeries performed on these glands.14,15
The exact explanation of the embryological origin of such a combination of anomalies is not clear. Blood vessel development occurs by (1) the vasculogenesis process facilitates the formation of vessels emerged by the coalescence of angioblasts, (2) angiogenesis occurs by sprouting vessels from existing vessels and remodeling of the vascular system, and (3) vascular intussusception (non-sprouting angiogenesis), in which existing vessels are divided to give rise to extra vessels. 16 One hypothesis is that if vascular intussusception does not proceed properly, more chances of fusion of existing blood vessels occur leading to common arterial trunk formation. Mata et al. 17 also suggested that the occurrence of common arterial trunks like TLFT is more prevalent in fetal conditions compared to adults because of more confluence of vessels during the vascular development and later on more resorption of the existing vessels.
According to Schoenwolf et al., 16 the right and left CCA and the initial portion of the right and left ICA arise from the third aortic arch arteries. The remote part of the ICA arises from the cranial continuation of the dorsal aortae, and the right and left ECA sprout from the third aortic arch and may have a contribution from remnants of the first and second aortic arches. According to another hypothesis, the evolution of the cranial and cervical regions is very dynamic which is why the first three aortic arches and their various vascular components may be remodeled into the carotid artery system. 18
In the present case, high carotid termination may be due to complex hemodynamic phenomenon in the developing head and neck region which may be accompanied by more cephalad extension of the truncus arteriosus and contribution from the first and second aortic arches.
Conclusion
The CB point has its significance owing to other important anatomic structures lying in conjunction, including cranial nerves. This point is of surgical importance during the management of carotid atheromatous disease and rarer diseases like carotid body tumors and carotid aneurysms. The anatomical evolution of the ECA system is a very complex mechanism of vasculogenesis being remodeled by angiogenesis, which is governed by the expression of so many factors for the regulation at the molecular level. Deviation at any step of this process would result in several anomalies which might be of much clinical importance. In this present case, it may be postulated as the failure of resorption of existing vessels during the process of remodeling, thus resulting in the persistence of the common arterial trunks which needs to be evaluated. There is a considerable amount of variability in the branching pattern of the ECA in the neck which warrants a clear anatomical understanding of the angioarchitecture. Before proceeding to the surgical procedure in the head and neck region, it is prudent to make out the level of the CCA termination and its emerging arterial pattern with the help of the latest imaging technology. Such precautionary measures will be of much relevance to avert injury to vital structures such as the hypoglossal nerve and minimize the fatal incidence of hemorrhage. Our report is an effort to share the information regarding the rare combination of anatomical variations and also the micrometric values of the ventral branches of the ECA useful for patient health care management.
Footnotes
Acknowledgements
The authors do convey their sincere gratitude to the authority of All India Institute of Medical Sciences, Raebareli, Uttar Pradesh, India, for providing the logistics to support this work.
Author contributions
A.K.S. and R.S.D. contributed equally to the work with regards to the concept, design, manuscript writing, and considered as co-first authors. T.P.M. and B.K.D. contributed by performing the literature search and editing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study has been approved by the Bioethics Cell, All India Institute of Medical Sciences, Raebareli, Uttar Pradesh (India) (2021-15-IMP-1).
Informed consent
Written informed consent has been taken from the legally authorized representative of the deceased person (cadaver).