
Abstract
Carpal joint osteoarthritis and the formation of bony irregularities of the carpal bone cause closed flexor tendon ruptures. This report describes a case of a flexor profundus tendon closed rupture of the little finger due to asymptomatic pisotriquetral osteoarthritis in a 73-year-old woman, which required differentiation from tendon rupture due to hamate bony irregularity due to bone erosion. Computed tomography showed cortical bone irregularities of the hamate and the narrowing of the pisotriquetral joint space, and a bony spur on the radial side of the pisiform. Intraoperative findings revealed the capsule of the pisotriquetral joint was torn on the radial side. Pisiform-hamate ligament disruption and the bony spur on the pisiform were found on this side. However, the flexor tendon floor on the hamate was intact. Surgical resection of the pisiform and a free tendon interposition graft for tendon rupture restored the good function of the little finger. Particular attention should be paid in making the diagnosis in cases with multiple possible triggers for closed flexor tendon rupture.
Introduction
Closed attritional rupture of the flexor tendons around the wrist can develop due to carpal joint osteoarthritis and the formation of bony irregularities of the carpal bone. 1 Pisotriquetral arthrosis, which is induced by pisotriquetral instability and repetitive micro-trauma, causes often ulnar-sided wrist pain and rarely the closed flexor tendon ruptures.2–7 The bony irregularities such as bony spur of the carpal bone and the nonunion of the hook of hamate can cause the spontaneous flexor tendon rupture.1,7–10 This report describes a case of a flexor profundus tendon closed rupture of the little finger by asymptomatic pisotriquetral osteoarthritis in a 73-year-old woman, which required differentiation from the tendon rupture due to hamate bony irregularity by bone erosion.
Case report
A 73-year-old woman, who was a nursing home worker, was referred to our hospital due to the inability to actively flex her left little finger at the distal interphalangeal (DIP) joint. Three days before visiting our hospital, she hit her little finger on a wooden hanger, and the little finger was forcibly bent. After that, she was not able to actively bend the DIP joint of the little finger; however, she was able to actively flex the finger at the proximal interphalangeal (PIP) joint (Figure 1). Other than housework, her daily activities included swimming and mountaineering. She had no history of systemic disease or symptomatic hand disease. Anteroposterior radiographs of the left wrist showed a cystic lesion of the hamate and osteosclerosis of the pisiform (Figure 2). A sagittal ultrasound (US) view showed a bulge at the flexor digitolum profundus (FDP) tendon of the little finger at the palm and distal forearm levels (Figure 3(a) and (b)). Computed tomography (CT) showed the cortical bone irregularities of the hamate adjacent to the cystic region (Figure 4(a)) and pisotriquetral joint space narrowing and a bony spur on the radial side of the pisiform (Figure 4(b)). We speculated that the closure of the FDP tendon of the little finger had occurred due to friction between a bony spur associated with pisotriquetral joint osteoarthritis or cortical bone irregularities of the hamate. For this reason, surgical exploration was performed. Intraoperative exploration revealed the FDP of the little finger was completely torn in the carpal tunnel and the distal tendon end stump was found in the palm of the hand and the proximal tendon end stump at the level of the forearm. The capsule of the pisotriquetral joint was torn on its radial side (Figure 5). Pisiform-hamate ligament disruption and the bony spur of the pisiform were found on this side. On the contrary, the flexor tendon floor on the hamate was intact (Figure 6). When the distal tendon stump was pulled centrally, at that time, the little finger passively exhibited full flexion; the tip of the tendon stump reached the exposed joint site (Figure 7). We diagnosed that the FDP of the little finger disruption is caused by osteoarthritic change of the pisotriquetral joint. The pisiform was removed under the periosteum. The articular surface of the pisiform was eburnated (Figure 8). A palmaris longus tendon graft was used as an interposition graft. From the day after the surgery, early active flexion motion was performed under extension block splint for rehabilitation. At 8 months after the operation, the grip strength of the affected hand was 16.3 kg, while that on the unaffected side was 19.1 kg and she could move the affected finger with full flexion and extension (Figure 9(a) and (b)). She has no restrictions of her activities of daily living, including swimming and mountaineering.

The patient was not able to actively flex the distal interphalangeal joint of her little finger.

Anteroposterior radiographs of the left wrist showed the cystic lesion of the hamate and osteosclerosis of the pisiform.
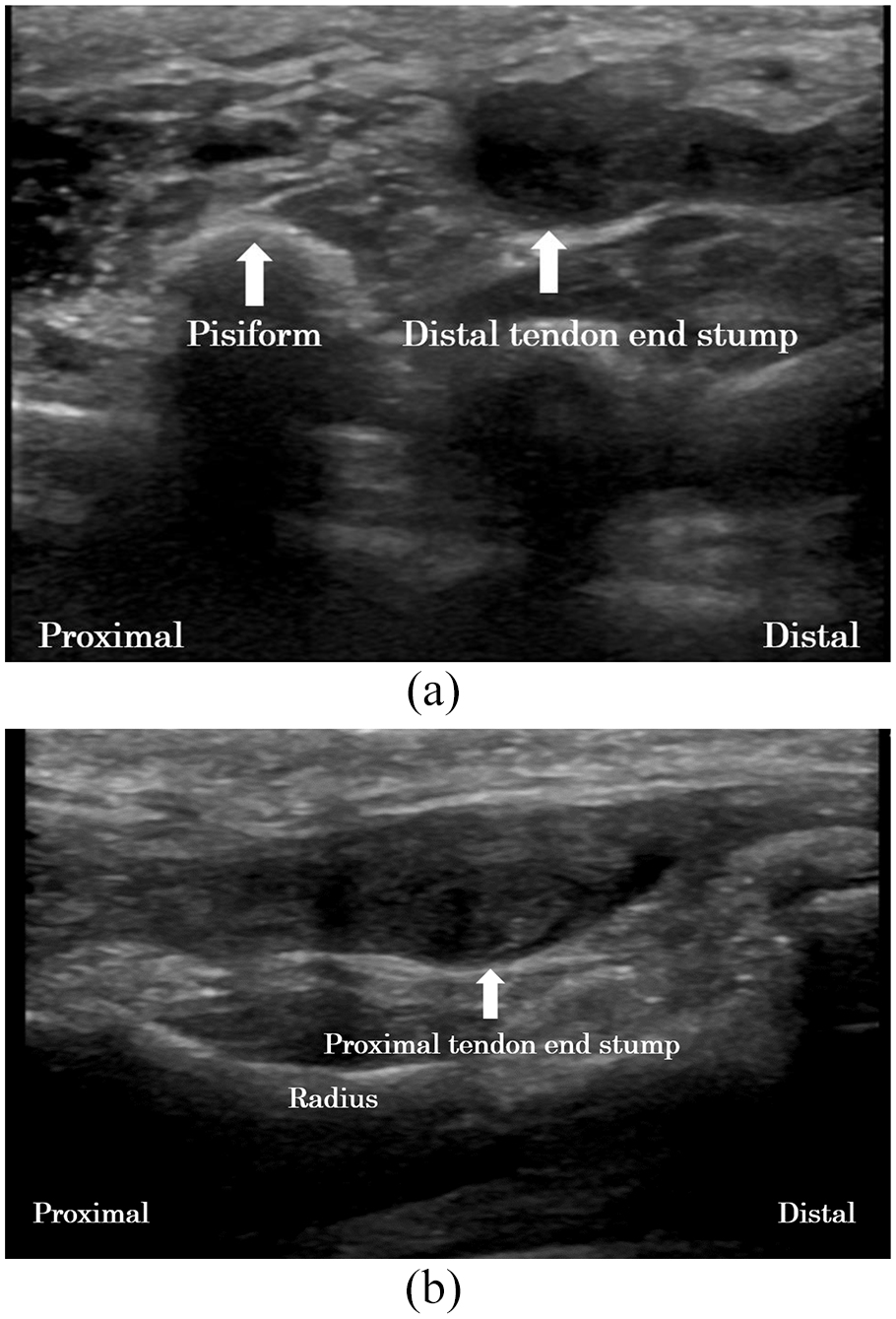
(a) Ultrasonography (sagittal view) showing the bulge of the flexor profundus tendon of the little finger (arrow) at the palm and distal forearm levels. (b) Ultrasonography (sagittal view) showing the bulge of the flexor profundus tendon of the little finger (arrow) at the distal forearm level.

(a) CT (axial view) showing cortical bone irregularities of the hamate adjacent to the cystic region (arrow). (b) CT (axial view) showing the PT joint space narrowing and the bony spur on the radial side of the pisiform (arrow).

The capsule of the PT joint was torn on the radial side (arrow).

The flexor tendon floor on the hamate was intact (arrow).

The tip of the tendon stump (arrow) reached the exposed joint site when the distal tendon stump was pulled centrally.

The articular surface of the pisiform was eburnated and osteocytes were observed (arrow).

(a), (b) At 10 months after surgery, the little finger had an active range of motion of 0°–90° at the matacarpophalangeal joint, 0°–90° at proximal interphalangeal joint, and 0°–70° at the DIP joint.
Discussion
Asymptomatic pisotriquetral osteoarthritis accidentally caused a closed FDP tendon rupture of the little finger in our case. Prior studies have demonstrated that a pathological condition of the pisotriquetral joint induced spontaneous flexor tendon ruptures.1–6 Pisotriquetral instability induced by the disruption of ligaments around the pisiform was reported as a cause of closed flexor tendon ruptures. 11 Our patient was a swimming and mountaineering enthusiast. The flexor carpi ulnaris (FCU) is reported to pull the pisiform proximally and ulnarly. 12 It seems that the FCU is mainly involved in pulling water in the crawl stroke in swimming and in pulling ropes in mountaineering. These operations may have induced instability of the pisiform and eventually caused pisotriquetral osteoarthritis, which caused the mechanical friction between the flexor tendon and the bony spur of the pisiform.
Radiography and CT of our case showed cortical bony irregularities of the hamate adjacent to the cystic region. However, the intraoperative findings revealed that flexor tendon floor over the hamate was intact. A bony spur on the carpal bone and the roughened surface of the flexor tendon floor due to an abnormality of the hook of the hamate have been reported to cause spontaneous flexor tendon ruptures.6–11 Closed tendon rupture due to pisotriquetral osteoarthritis occurs in older individuals (mostly in their 60s or 70s) more frequently in comparison to rupture caused by the hamate.2–4,8 However, careful observation is required to prevent the misdiagnosis of the cause of tendon rupture due to secondary pathological changes of the surface, such as pathological fracture caused by intraosseous ganglion in carpal bone. 10 Our case had these image findings that may cause the close flexor tendon rupture. These points were considered by the hand surgeons to be diagnostically instructive in this case.
We excised the pisiform to prevent the recurrence of rupture of the reconstructive tendon. Prior studies demonstrated that excision of the pisiform had no adverse effects on the hand and wrist function from a long-term perspective in patients with this treatment.13,14 At 8 months after the operation, our case was satisfied with her good hand and wrist function in daily life. We performed interposition tendon grafting to achieve good excursion of the FDP muscle of the little finger and early controlled active motion hand therapy. Preparation for flexor digitorum superficialis tendon transfer from the ring to the little finger or transfer of the distal FDP stamp tendon of the little finger to the FDP tendon of the ring finger may be necessary if the condition of the excursion of FDP muscle of little finger is poor. 1
Conclusion
Asymptomatic pisotriquetral osteoarthritis can be the cause of the closed flexor tendon ruptures of the little finger in activity of daily life. It may be difficult to predict the spontaneous flexor tendon rupture in old age by silent pisotriquetral osteoarthritis and a bony spur on the carpal bone and the roughened surface of the flexor tendon floor. However, we should raise awareness of these pathological hand conditions and properly diagnose the cause of the spontaneous flexor tendon rupture and treat the tendon ruptures based on the cause.
Footnotes
Author contributions
Y.H. and T.T. gathered information and wrote the manuscript; T.T. supervised the treatment; T.T., T.K., Y.H. and R.S. treated the patient and gathered information; T.T. and Y.H. analyzed the data and contributed to the discussion of the research; H.C. supervised the research. All authors have read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information and accompanying images to be published in this article.