
Abstract
Pseudomonal ecthyma gangrenosum is a well-known condition in immunosuppressed patients. However, ecthyma gangrenosum associated with Klebsiella pneumoniae is a rare entity that requires early recognition and optimal antibiotic and surgical management. We herein report the first case of colistin & carbapenem-resistant Klebsiella pneumoniae ecthyma gangrenosum in an acute myeloid leukemia patient. A 30-year-old female with acute myeloid leukemia received induction chemotherapy at the National Institute of Blood Diseases and Bone Marrow Transplantation hospital. Post-chemotherapy, she developed fever and a necrotic erythematous papule on right forearm. Colistin-susceptible carbapenem-resistant Klebsiella pneumoniae was isolated in cultures. Susceptibility testing was performed by microbroth dilution method. Worsening necrotic lesion prompted surgical debridement. Histopathology of debrided tissue revealed necrotic inflammation, and tissue cultures grew colistin-resistant carbapenem-resistant Klebsiella pneumoniae (colistin minimum inhibitory concentration >4 µg/mL). We speculate that colistin resistance was acquired due to impaired antibiotic penetration in necrotic nidus. A higher incidence of carbapenem-resistant Klebsiella pneumoniae-associated ecthyma gangrenosum is anticipated in hem-oncology patients, and timely diagnosis, appropriate antibiotics, and surgical debridement remain the only potential cure.
Introduction
Ecthyma gangrenosum (EG) was identified in the year 1950 as a pathognomic feature of pseudomonal bloodstream infection, mainly in immunocompromised hosts.1,2 EG may develop both through hematogenic seeding or direct skin inoculation. It initially appears as a single erythematous papule or a hemorrhagic blister that evolves into a necrotic ulcer with a black eschar and a red halo. 3 Pathophysiologically, it is the venular obliteration and thrombosis by the infective pathogen that culminates in epidermal dissection and necrotic ulceration.
Various host, disease, and treatment-related factors contribute to the immunosuppressed state of patients with hematological malignancies. Rapid emergence of antimicrobial resistance and nosocomial infections has created an additional significant risk of lethal infections for this immunocompromised population. Klebsiella pneumoniae (KP), a gram-negative bacteria, is notorious for acquiring extensive drug resistance through mechanisms other than selection pressure like horizontal gene transfer and gene transfer factors (transposons and integrons). 4 KP is the main carbapenem-resistant (CR) organism belonging to Enterobacteriaceae. Carbapenem resistance is directly acquired through the production of various carbapenemases, for example, KPC type carbapenemases, metallo-β-lactamases, or oxacillinases. However, extended spectrum beta-lactamases, AmpC enzymes, and porin loss can also impart reduced susceptibility to carbapenems.5,6 Colistin is considered to be the last resort antibiotic for carbapenem-resistant Klebsiella pneumoniae (CR-KP). 7 CR-KP can also acquire colistin resistance while on colistin treatment through various intrinsic chromosomal and plasmid-mediated mechanisms, plausibly through antibiotic-induced bacterial stress response.8,9
So far, only a single case of EG secondary to a compound infection with KP and Streptococcus vestibularis has been reported in the literature. 10 We herein report the first case of colistin-resistant CR-KP EG in an acute myeloid leukemia (AML) patient.
Case presentation
A 30-year-old female patient with a recent diagnosis of AML received standard induction chemotherapy, with 3 days of daunorubicin and 7 days of cytarabine, at the National Institute of Blood Diseases and Bone Marrow Transplantation.
On Day +11 post-chemotherapy, she started spiking fever without any clinically apparent focus. She was empirically started on meropenem and vancomycin, as per institutional policy for the management of patients with febrile neutropenia and central line in place. During the initial 36–48 h, she remained hemodynamically stable. However, she developed a red erythematous lesion on her right forearm that progressed overnight into a necrotic lesion (Figure 1). KP was isolated from blood cultures. Other cultures, that is, urinary, stool, and induced sputum cultures turned out to be negative. Radiological investigations performed as part of surveillance during neutropenic phase were also negative. Antibacterial susceptibility pattern revealed CR-KP sensitive to colistin. Susceptibility pattern was determined and confirmed by broth microdilution method, which reported minimum inhibitory concentration (MIC) values of 4 and <2 µg/mL for meropenem and colistin, respectively (Clinical and Laboratory Standards Institute (CLSI) and European Committee for Antimicrobial Susceptibility Testing (EUCAST), 2019). After acquiring susceptibility results, patient was switched to a combination of extended dose meropenem infusion and colistin.

Right forearm showing ecthyma gangrenosum.
On Day +13, her neutrophil count recovered, but the necrotic lesion continued to expand along with extensive surrounding inflammation, prompting surgical debridement.
Operative findings showed full-thickness necrosis of right forearm skin involving 80% of flexor surface that had partly extended to the extensor surface along with patchy muscle necrosis (Figure 2). Post-debridement patient remained vitally stable. Samples were sent for histopathology and fungal and bacterial cultures. Histopathology revealed severe necrotic inflammation and hemorrhage. However, fungal microscopy and cultures turned out to be negative.

Lesion after first debridement.
CR-KP was isolated in her tissue and fluid cultures. Organism identification was performed by standard microbiological techniques and routine biological tests. Further organism identification is performed by API 20E. Antibiotic susceptibility testing was performed by broth microdilution method, and antibiotic susceptibility was interpreted according to CLSI and EUCAST (2019). Broth microdilution results showed that none of the fluoroquinolones, aminoglycosides, and penicillins with β-lactamase inhibitors, cephalosporins, and polymyxins was effective against the isolate. MIC values for antibiotics were very high except for cotrimoxazole and tigecycline; piperacillin-tazobactam >128/4 µg/mL, ceftriaxone >4 µg/mL, c >34 µg/mL, gentamicin >16 µg/mL, ciprofloxacin >1 µg/mL, cotrimoxazole <2/38 µg/mL, co-amoxiclav >8 µg/mL, colistin >4 µg/mL, meropenem >4 µg/mL, and tigecycline <1 µg/mL.
After acquiring antibiotic susceptibility testing from the debrided tissue cultures, patient was switched to a combination of tigecycline and trimethoprim/sulfamethoxazole. Surgical site was re-evaluated after a week and partial wound approximation was performed (Figure 3). Currently, she is clinically stable with no signs of infection/sepsis. Her primary disease is in remission, and she has been offered single-agent oral Fms-like tyrosine kinase (FLT3) inhibitor till wound healing and split skin grafting.

Lesion after partial wound approximation.
Discussion
Pseudomonal EG is a well-known entity in immunosuppressed patients. Among other gram-negative organisms, Escherichia coli, Citrobacter freundii, various other Pseudomonas species, and Morganella morganii have been reported as a cause of EG. However, EG associated with KP in hem-oncology patients is a rare entity and is associated with severe limb/life-threatening complications, necessitating early recognition and optimal antibiotic and surgical management.
Viamen et al. have published a retrospective review of 28 reported cases of EG from 2001 to 2015. Of these 28 cases, eight cases were reported in patients with hematological malignancies. 11 Pseudomonas aeruginosa was isolated from the lesions of five patients, and the remaining three patients had Pseudomonas stutzeri, E. coli, and Fusarium solani in their cultures. Most of these patients (80%) had a single EG-like lesion, with limbs being the most common site.
Since 1991, only four cases of KP-associated EG have been reported. Three of these four patients were immunosuppressed secondary to nasopharyngeal carcinoma, diabetes mellitus, and AML. The site of the lesions varied, and multiple lesions were observed to be more common than single lesions.
A recent case report of KP-associated EG in AML was published by Koumaki et al. 10 in 2018. The case has remarkable similarities with our case (Table 1). Both the patients had the same clinical diagnosis and developed KP bacteremia post-induction, with EG involving their upper limb. Both the patients had CR-KP in blood and tissue cultures, and their lesions kept worsening despite adequate antibiotic therapy, prompting surgical debridement to control the condition. In the case reported by Koumaki et al., 10 compound infection with S. vestibularis and KP was established in the patient’s blood and tissue cultures, whereas KP was isolated as a single pathogen in our case. Nevertheless, both the cases highlight the emerging potential of CR-KP as a cause of EG in patients with hematological malignancies as well as the ineffectiveness of conservative antibacterial therapy.
Salient features of reported CR-KP ecthyma gangrenosum cases in hem-oncology patients.
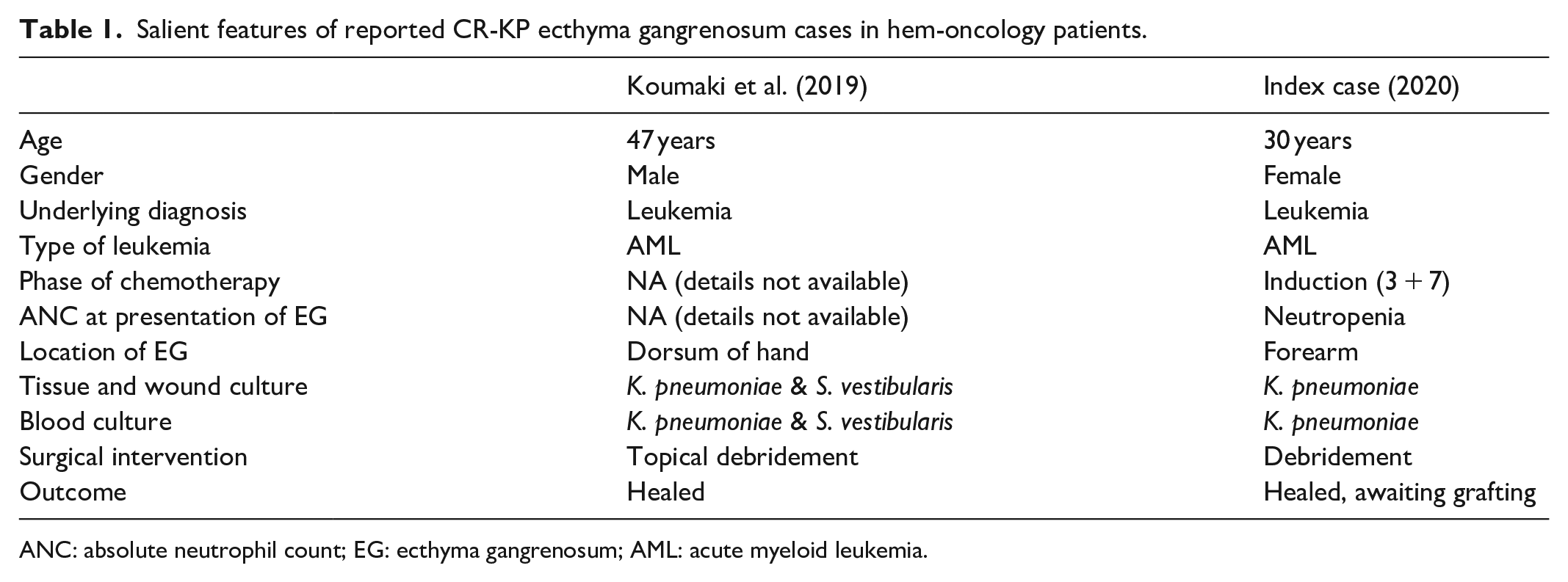
ANC: absolute neutrophil count; EG: ecthyma gangrenosum; AML: acute myeloid leukemia.
CR-KP is the most common CR organism in the healthcare setting. 12 Colistin is considered to be the last resort antimicrobial agent. However, over the last decade, the rate of colistin-resistant CR-KP has steadily increased from 2% to 9%.13,14 Of the various postulated mechanisms of acquiring colistin resistance by CR-KP, the most plausible is the development of resistance while on colistin treatment. 15 Bacterial lipopolysaccharide (LPS) destabilization and lysis through an electrostatic detergent action is the major antibacterial mechanism of colistin. 16 CR-KP modifies the LPS structure by upregulating pmrHFIJKLM, a chromosomal gene responsible for causing anionic neutralization that result in the inhibition of electrostatic interaction and antibacterial action of colistin. A second known mechanism of colistin resistance is through a plasmid-mediated transfer of mcr gene homologues, causing altered electrostatic quality and reduced colistin binding affinity.8,17
In our case, the initial CR-KP isolate was susceptible to colistin. However, repeat cultures after 48 h grew CR-KP resistant to colistin even though an adequate dose of colistin was administered. It has previously been reported that suboptimal dosing of colistin may result in in vitro and in vivo acquired colistin resistance through pmrHFIJKLM upregulation.15,18 In our case, we speculate that the necrotic lesion with compromised blood supply and antibiotic penetration served as a sanctuary nidus for CR-KP growth and colistin resistance.
Another important aspect of this patient’s future management, during further chemotherapeutic cycles, would be extremely high risk of recurrent multidrug resistant (MDR) infections. Patients who either become colonized or have history of previous MDR infections are considered high risk for MDR recurrence. These patients should ideally be offered de-colonization with either oral non-absorbable antibiotics or fecal microbiota transplantation. However, in CRE, decontamination is not recommended due to the theoretical risk of further antibiotic pressure and selection of resistant strains. 19 Antibiotic de-escalation strategy is considered optimal, safe, and feasible for this high-risk patient population, that is, upfront empirical institution of antibiotics covering for MDR and early de-escalation/discontinuation at 72–96 h after either no growth or growth of susceptible pathogen in baseline cultures.20,21 This strategy not only substantially lowers the mortality associated with gram-negative MDR organisms but also prevents emergence of resistant strains due to early de-escalation/discontinuation after availability of baseline cultures.
Conclusion
CR-KP is emerging as a major threat for immunocompromised patients because of very high virulence and a peculiarity to acquire antimicrobial resistance while on antibacterial treatment. Through this article, we want to highlight the importance of early surgical debridement along with accurate antibiotics selection and dosing to manage this life/limb-threatening condition.
Footnotes
Author contributions
A.J. contributed to the manuscript writing and critical review of the article. A.S. collected and formulated all the clinical data and manuscript writing. F.R. contributed to the manuscript writing. A.S. contributed to the manuscript writing and submission of manuscript. T.S. contributed to the critical review of the article.
Availability of data and materials
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This case report was approved by the hospital ethics committee (NIBD Ethics Committee) with protocol approval no. NIBD/RD-233/14-2020.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.