
Abstract
Emergency total gastrectomy for patients with gastric cancer who are in shock carries a high risk of esophagojejunal anastomosis leakage. No alternatives have been reported to reduce this risk. This study reports two patients with gastric cancer who were in shock and underwent emergency gastrectomy and two-stage esophagojejunal anastomosis with good results. In the first stage, immediately after gastrectomy, the esophagus was attached to a Roux-en-Y jejunal loop that prevented retraction of the esophagus into the mediastinum. In the second stage, in a second surgery, the esophagojejunal anastomosis was completed under better clinical conditions.
Introduction
Esophagojejunal anastomosis (EJA) leakage is one of the most common surgical complications after gastrectomy for gastric cancer (GC), with reports ranging from 2% to 20%.1–12 EJA leakage impacts the length of hospital stay, increases costs, and has a mortality rate that can reach 50%.2–5,7,10,13 Risk factors for EJA leakage in emergency gastrectomy have been described as lack of tissue irrigation and oxygenation due to shock or sepsis, patient nutritional status, and the surgeon’s experience.3,6,8
To date, no reconstruction alternatives have been reported in cases of emergency total gastrectomy for GC to reduce the risk of EJA leakage.
In a case report of one patient who required emergency total gastrectomy due to gastric necrosis after ingestion of a caustic substance, gastrectomy was performed in the first surgery and Roux-en-Y reconstruction in the second, with good postoperative results. 14
Our group has performed terminolateral two-layer manual EJA in elective laparoscopic total gastrectomy for patients with GC, in which the sectioned esophagus is first sutured to a Roux-en-Y jejunal loop using a linear stapler, and the remaining layers are closed with manual suturing 15 (Figure 1).

First stage EJA (Steps a and b); Second stage EJA (Steps c-g). Steps of terminolateral manual EJA. (a and b) The esophagus is sectioned with a cutting linear stapler and then hand-sutured to a Roux-en-Y jejunal loop with 3-0 polyglycolic acid thread. (c and d) The esophageal lumen and the jejunal lumen are opened using harmonic forceps or a hook, and the second layer is closed by manual suturing with the same material. € The first anterior layer is sutured with 3-0 polyglycolic acid thread. f and g: A 38-French calibration bougie is passed, and the second layer is closed with 3-0 polyglycolic acid thread. The bougie is removed.
After emergency gastric resection, attaching the esophagus to a Roux-en-Y jejunal loop may be a fast and safe alternative to prevent retraction of the esophagus into the mediastinum and to prevent the need for tube drainage of the distal esophagus in patients in shock who require vasoactive drugs (VAD) and are malnourished. This procedure allows the performance of a safe anastomosis within the abdomen with a healthy esophagus.
This study presents two clinical cases in which emergency gastrectomy was performed in patients with GC by performing two-stage EJA.
Case report
The first case is a 56-year-old male patient with GC who underwent laparoscopic D2 subtotal gastrectomy with curative intent by Roux-en-Y reconstruction 1 month after a noncurative submucosal dissection. The definitive biopsy of the endoscopic submucosal surgical specimen dissection showed a moderately differentiated tubular adenocarcinoma with 1 mm-deep submucosal invasion and lymphatic and venous invasion. After 48 h, the patient developed septic shock with signs of peritoneal irritation, need for VAD, and drainage of saliva through the tubes; therefore, an exploratory laparotomy was performed, and 50% dehiscence of the gastrojejunal anastomosis, necrosis of the residual stomach, diffuse peritonitis, and rotation of the alimentary loop were found. We performed a total gastrectomy, resected the gastrojejunal anastomosis, sectioned the abdominal esophagus with a cutting linear stapler, and attached it to a Roux-en-Y jejunal loop with 3-0 polyglycolic acid suture without anastomosis (Figure 1(a) and (b)).
In a second stage performed 3 days later, when the patient was stable, EJA was completed manually (Figure 1(c)—(g)). The patient progressed without complications and was discharged after 15 days. The definitive biopsy showed no cancer or lymph node involvement. The final staging was T1bN0M0.
The second case was a 72-year-old male patient with severe sarcopenia and a history of high blood pressure. He visited the emergency department with a history of dyspnea, an 11 kg weight loss, impaired quantitative consciousness, and upper gastrointestinal bleeding, with hypotension and no need for VAD. An emergency upper digestive endoscopy was performed and identified cancer of the gastroesophageal junction (Siewert III) with active bleeding; thus, injection therapy with adrenaline and thermocoagulation was performed (Figure 2).

Endoscopic images showing cancer of the gastroesophageal junction (Siewert III, Borrmann 1).
A day later, the patient had a new episode of gastrointestinal bleeding that required VAD. Because endoscopic hemostasis was not achieved, an emergency total gastrectomy was performed (Figures 3–5) by sectioning the abdominal esophagus with a cutting linear stapler and suturing it to the Roux-en-Y jejunal loop without completing the anastomosis, followed by duodenostomy with a Pezzer catheter.

Reconstruction after emergency gastrectomy. The jejunal loop is pulled up in accordance with the Roux-en-Y procedure and attached to the abdominal esophagus without anastomosis, a nasoesophageal decompressive tube is placed, and duodenostomy with a Pezzer catheter is performed.

Surgical specimen after emergency total gastrectomy showing a 5 cm tumor. (Siewert III, Borrmann 1).
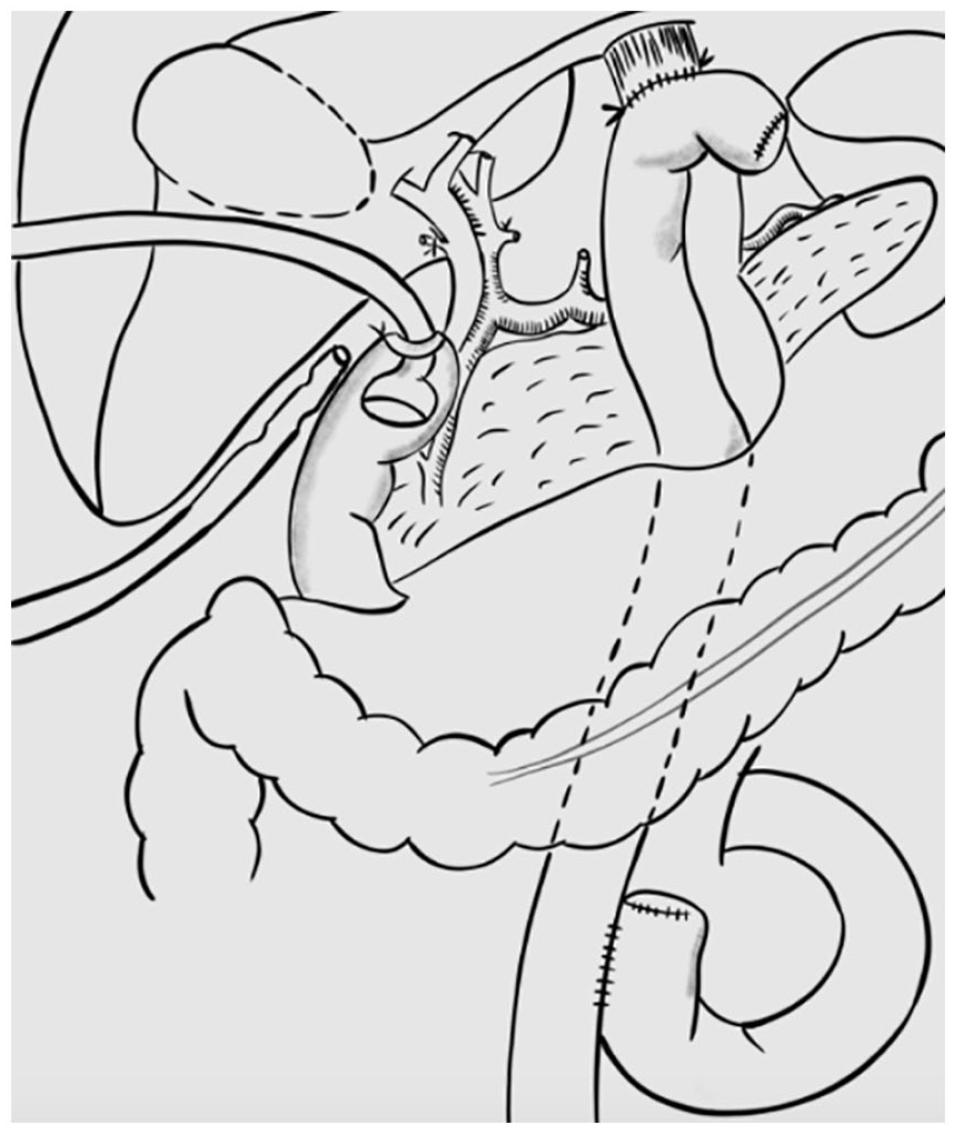
Diagram of reconstruction after emergency gastrectomy, in which the jejunal loop is pulled up according to the Roux-en-Y procedure, attached to the esophagus without anastomosis, and followed by duodenostomy with a Pezzer catheter.
Due to the severe sarcopenia and positive PCR test for SARS-CoV-2 in the immediate postoperative period, the patient underwent prehabilitation for 30 days. In a second stage, the EJA was completed without incident (Figure 6).

Second stage of EJA. See steps c-g in Figure 1.
The patient progressed without complications. The biopsy reported a moderately differentiated 8.8 cm x 6 cm x 4 cm tubular-papillary adenocarcinoma with subserosal invasion, lymphatic and vascular invasion, negative edges, 11/53 positive ganglia, and a stage of T3N3aM0.
Both patients had good postoperative recovery, being discharged at 15 days. In the follow-up, they did not present EJA complications and were still alive for their cancer check-ups.
Discussion
Emergency gastrectomy for GC is performed in exceptional circumstances and has a mortality rate as high as 20%. 16 There are few related reports in the literature; 16 consequently, there are several controversial technical aspects of this procedure, 16 such as whether to perform lymphatic dissection, whether reconstruction should be immediate or deferred, and how to manage the duodenal stump.
In emergency surgery, the main objectives are to resuscitate the patient and control the site of bleeding or necrosis that caused shock as efficiently and safely as possible, avoiding additional steps that prolong surgical time or increase patient risk. In the case of emergency gastrectomy, the two most common sites of complication are leakage of the EJA and the duodenal stump, both of which have high morbidity and mortality (20%–50%).2–5,7,10,13 We consider Roux-en-Y jejunojejunal anastomosis safe, even in cases of emergency, and complications are the exception.
As a group, we propose the use of two-stage EJA as a novel alternative to emergency total gastrectomy for GC. In a first surgery, once the gastrectomy is completed, a Roux-en-Y jejunal loop is attached to the abdominal esophagus to prevent its retraction into the mediastinum (Figure 1(a) and (b)). Then, in a second surgery, when the patient is stable and under better nutritional conditions, EJA is electively completed by a team of experienced surgeons, using a laparoscopic approach if feasible (Figure 1(c),–(g)).
This technique could be useful not only for patients with GC but also for those in need of emergency gastrectomy with gastric necrosis secondary to the ingestion of caustics or gastric volvulus.14,17–19 A two-stage strategy not involving the esophagus has been used in the pediatric population. 20
The novelty of the EJA presented in this work is not because of the way it is performed but because of the time, as it was performed in two stages. There are several methods for performing an EJA: circular stapling, linear stapling and completely manually. When using stapler techniques in a second intervention, all procedures require significant release of a segment of the esophagus and removal of the suture that attaches the intestine to the esophagus, which already had scarring from the first intervention. In emergency cases, the gastroesophageal junction should be considered compromised by cancer invasion, as occurred in the second patient, or as having complete necrosis of the gastroesophageal junction in case of a volvulus, which is why the esophagus section is in the mediastinum and the length of the mesentery is difficult to reach without tension.
Historically, in total emergency gastrectomies, general surgeons use probes to direct saliva from the esophagus to the outside, but two problems arise: (1) retraction of the esophagus toward the mediastinum is required, since the esophagus easily contracts 15% when losing its natural attachment elements 21 and (2) there is a need to resect more esophageal tissue in the second surgery due to the scar left by the probe. These issues lead to anastomosis of the diaphragmatic pillars in the mediastinum, which is technically more difficult and is associated with a greater risk of leakage. 22
The staged technique allows the posterior portion of the anastomosis to attach and heal after the second surgery, reducing the risk of leakage on the posterior side. We consider duodenostomy a safe alternative in emergency gastrectomy. Our group has used it successfully, and the literature reports good results in patients at risk, since, in practice, it eliminates the possibility of leakage from the duodenal stump. 23 In addition, duodenostomy is useful as a potential access route for enteral nutrition therapy during the prehabilitation period before the second surgery, which could improve intestinal trophism, reduce the risk of infections, and improve nutritional status more efficiently.24–26
Duodenostomy is a technique with decreasing frequency, and we have indicated it without complications, except in four scenarios: (1) total esophagogastrectomy due to caustic ingestion, (2) complex duodenal injury, (3) patients with gastric cancer in which the duodenum cannot be closed safely due to peptic ulcer scars, and (4) emergency gastrectomy in malnourished patients.
The advantages of duodenostomy are that (1) it decreases the pressure on the duodenum, and (2) it allows a feeding route, providing a greater supply of nutrients directly to the intestine, as conducted in the second patient during his prehabilitation stage.
There are reports that duodenostomy has been used for nutritional access, which was used in the second patient while waiting for the second intervention. 27 This strategy was combined with parenteral nutrition and physical therapy to improve the patient’s functional and muscular state and to reach a prealbumin level greater than 15 mg/dL. With respect to COVID-19 infection, it is currently recommended to wait 7 weeks prior performing elective surgery; however, as the nutritional goals were achieved and to avoid laborious surgery due to adhesions, we made the decision to complete the anastomosis at 30 days.
This technique is beneficial since it prevents the problem of a less-experienced team performing a difficult anastomosis on a patient in shock, waiting for a time when conditions are ideal, so there is no doubt that disconnecting the esophagus is worrisome. Our initial plan was to complete the anastomosis at 7 days, but the COVID-19 diagnosis led us to defer this decision because we were unsure how it would evolve.
We believe that leaving the esophagus disconnected only slightly increases the risk of pneumonia if the precaution of actively aspirating saliva through a tube is taken. In our experience, several patients live with an obstructed or closed esophagus, and there is only a slight risk of pneumonia while waiting for their final surgery due to end-stage achalasia, peptic or caustic-related esophageal stricture or esophageal cancer during neoadjuvant chemoradiotherapy.
Conclusion
Two-stage EJA is a novel and safe technique to reduce the risk of leakage that can be used in patients with GC who are in shock and have an indication for emergency total gastrectomy since it prevents retraction of the esophagus into the mediastinum, thus allowing elective EJA to be performed under better hemodynamic and nutritional conditions by a team of experienced surgeons.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The ethics committee of our institution approved the publication of this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.