
Abstract
Patients affected with COVID-19 are at risk of developing serious and life-threatening conditions. The clinical manifestations of COVID-19 were detected in asymptomatic cases to severe clinical symptoms with a major impact on the respiratory system. A few cases of cutaneous as well as an oral lesion of herpes zoster in patients with COVID-19 were reported in the literature. We present a case of the rapid appearance of the oral lesion as a manifestation of herpes zoster associated with COVID-19 infection. Our case highlights the importance of oral examination as well as oral care in patients with COVID-19 infection.
Introduction
Recent data of patients infected with COVID-19 showed various clinical signs and symptoms such as sore throat, headache, hypogeusia, diarrhea, bone ache, and in severe cases pneumonia. 1 Reactivation of herpes zoster (HZ) during the acute or subacute phase of COVID-19 was related to the decline in the varicella zoster virus–specific cell-mediated immunity. 2
COVID-19 showed a direct impact on T-lymphocytes immune dysfunction resulting in lymphopenia which causes decreased body resistance to infection, and it may increase the reactivation of the HZ virus.3,4 We present a unique case of clinically diagnosed oral lesion of HZ infection 10 days after COVID-19 clinical signs and symptoms were detected. Our case highlights the importance of increasing the awareness among researchers and dental practitioners about the possible association between HZ and COVID-19.
Case presentation
A 49-year-old female was referred to the Oral Medicine and Periodontology clinic, Faculty of Dentistry, Mansoura University, for further evaluation of a painful lesion on the hard palate that appeared 10 days after the clinical signs and symptoms of COVID-19 infection such as sore throat, fever, fatigue, bone pain, headache, and dry cough.
Intraoral examination revealed unilateral vesicles filled with clear fluid as well as painful erythematous areas involving one side of the hard palate which was preceded by initial stabbing pain. The pain was continuous, severe, and sharp. The vesicles were small and few in numbers. Later, they increased in number with watery discharge. The palatal mucosa surrounding the vesicles was tender to touch (Figure 1). During detection of the oral lesion, the patient was still complaining of mild symptoms of COVID-19 infection as bone pain and headache.

Clinical photograph showing unilateral vesicles and erythematous areas of the hard palate.
Extraoral examination showed unilateral palpable submandibular and cervical lymph nodes. No swelling of the neck, no temporomandibular joint (TMJ) clicking, or tenderness of muscles of mastication. The medical history showed hypertension, osteoarthritis, and maxillary sinusitis. The patient denied any history of shingles or vaccination for HZ.
Laboratory investigations revealed lymphopenia, neutrophilia, elevated levels of serum alanine aminotransferase and aspartate aminotransferase, elevated lactate dehydrogenase, and high C-reactive protein. Chest X-ray and computed tomography (CT) were consistent with COVID-19 infection (Figure 2(a) and (b)).
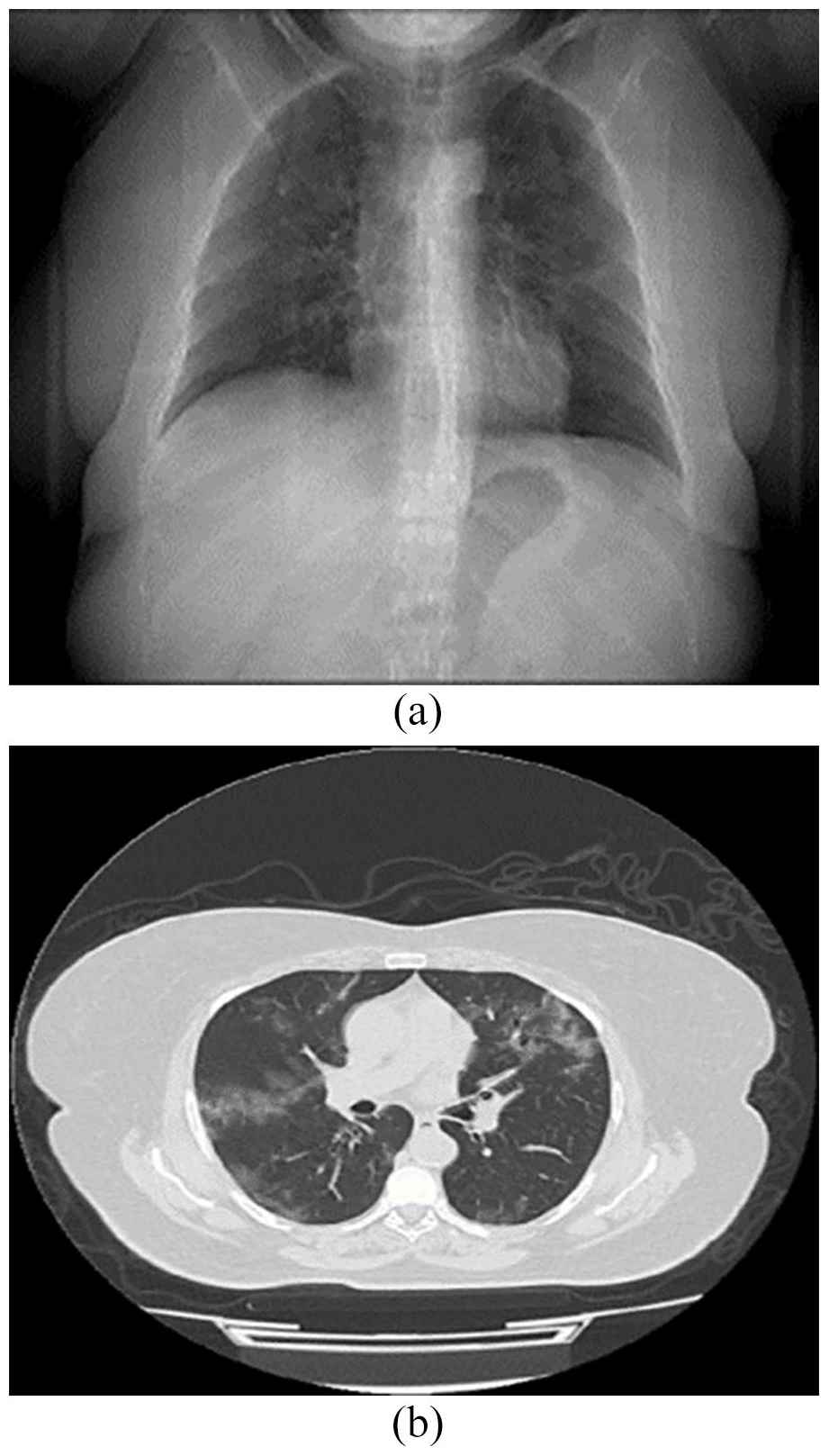
(a) Chest X-ray posteroanterior view shows ill-defined bilateral irregular patches scattered all over the lung especially in the right lung middle zone. (b) Non-contrast CT scan of the chest: Thin axial cuts were taken through the chest with lung and mediastinal windows, reveals bilateral pulmonary pan-lobar scattered peripheral patchy zones of ground-glass opacification with fine inter-lobular septal thickening, likely of pneumonic nature.
The patient has been prescribed acyclovir 800 mg tablets five times per day for 10 days as well as topical antiseptics with chlorhexidine. In addition, paracetamol was prescribed for pain and fever. After 10 days, the patient showed full recovery of the oral lesions as well as COVID-19 infection. Regarding COVID-19 vaccination, our case did not receive a vaccine of COVID-19 till the time of appearance of oral HZ.
Discussion
The concern about the association between the COVID-19 infection and HZ was raised.2,3,5 The clinical manifestations of COVID-19 were detected in asymptomatic cases to severe clinical symptoms with a major impact on the respiratory system. 6 Furthermore, HZ may appear in completely asymptomatic COVID-19 patients. 7
Recently, a few reports of reactivation of HZ during COVID-19 infection were published. Elsaie et al. 3 reported a HZ lesion in two patients with COVID-19 with mild or no respiratory symptoms and no history of contact with known or suspected COVID-19 cases.
Desai et al. 2 reported unilateral vesicular painful rashes along the dermatomes T-11-12 in a patient with COVID-19 infection. The lesions were detected 6 weeks after the COVID-19 symptoms started. 2 However, we detected the HZ lesion 10 days after COVID-19 symptoms started.
We believe that a few reports of HZ in COVID-19 patients are due to many factors as a full evaluation of patients with COVID-19 in terms of oral mucosa is not commonly performed due to the severity of the diseases. In addition, it may be difficult for clinicians to detect those lesions in patients without painful symptoms.
Vaccine-related HZ cases have been reported worldwide. Recently, COVID-19 vaccination was reported as a triggering factor of HZ. 8 Iwanaga et al. 9 reported 399 cases of HZ after receiving the vaccine of COVID-19. There might be a link between COVID-19 vaccine and HZ emergence; however, the mechanism is still unknown.5,9,10 The possible risk factors for development of HZ after COVID-19 vaccine include the decrease in immune response associated with old age of the patient, HIV infection, physical trauma, iatrogenic immunocompromission, or comorbid conditions such as malignancy or chronic kidney or liver disease. 8
The period between HZ and COVID-19 differs between cases. In our case, we detect HZ 10 days after the symptoms of COVID-19 started. Other cases were reported in 2–3 weeks from the start of COVID symptoms. 11 Similarly, HZ was detected in cases of COVID vaccination within first week to the fourth week of vaccination with mean period between HZ and COVID-19 vaccination was 7.64 days. 8
Increased incidence of HZ during COVID-19 outbreak may be related to the intense stress during the infection and the altered immunity during the pandemic. 12 Biopsy was not performed on our patient; however, we recommend further research in the form of well-designed studies to be conducted to establish whether COVID-19 raises the risk of HZ.
Conclusion
Dentists, dermatologists, and otolaryngologists should be concerned about the probably rising incidence of HZ during the COVID-19 pandemic and consider appropriate therapeutic and protective measures against it.
Footnotes
Acknowledgements
The authors acknowledge the patient presented in this case report for her active contribution.
Author contributions
W.S. contributed to writing-original draft. F.A. contributed to editing-original draft. M.M.E. contributed to writing-review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Patient’s consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.