
Abstract
Infections with Rothia mucilaginosa are rare. We present an unusual case of Rothia mucilaginosa in an immunocompromised host, which is usually considered a low virulence pathogen. The objective of this report is to highlight spectrum of clinical presentations in an immunocompromised individual and discuss various antimicrobial treatment options in the light of lack of definitive treatment guidelines for this organism.
Introduction
Rothia mucilaginosa resides in oral cavity and upper respiratory tract. 1 Although viewed as an organism of low virulence in immunocompetent host, it can cause various types of infections in immunocompromised host. 2 Rothia mucilaginosa has the potential to cause sepsis, pneumonia, meningitis, endocarditis, peritonitis, dermatitis. 3 – 5 Reports in literature involve the use of various antibiotics including penicillin, cephalosporins, carbapenems, and vancomycin for the treatment of this infection.6,7 We describe the case of a 17-year-old acute myeloid leukemia (AML) patient who developed Rothia mucilaginosa bacteremia followed by dissemination to lungs (nodules) and brain (meningitis/ventriculitis, brain abscess), complicated by hydrocephalus, eventually needing ventriculoperitoneal shunt. He could not be a candidate for bone marrow transplant due to his debilitated condition. He later succumbed to complications related to his AML despite palliative chemotherapy. We discuss dilemmas in the management and propose potential antimicrobial options due to lack of evidence-based guidelines.
Case report
A 17-year-old patient with high-risk acute myeloid leukemia (AML), HIV negative, non-diabetic, weighing 64 kg, with recent intensification phase 1 chemotherapy with intrathecal cytarabine (70 mg), systemic cytarabine (1000 mg/m2/day for 5 days—total 5 g/m2) and etoposide (150 mg/m2/day for 5 days—total 750 mg/m2) and on prophylaxis with trimethoprim 160 mg/sulfamethoxazole 800 mg (Bactrim DS tablet twice every Saturday, Sunday), levofloxacin 500 mg daily, and posaconazole (300 mg daily) was admitted (8 days after completion of 5 days of chemotherapy) with 1 day history of fever, headache, fatigue, and sore throat. His admission vitals included temperature of 38.3o C, heart rate 115, respiratory rate 18, blood pressure 118/68, saturation 100% on room air. His white blood cell count was 0.4 (normal range: 4.5–11 K/mm3), absolute neutrophil count of 0, hemoglobin 6.4 (normal range: 11.5–15.5 g/dL), platelet count 7 (130–400 K/mm3). He was started on empiric cefepime (2 g IV every 8 h) and vancomycin (1 g every 6 h followed by change to continuous infusion at 2400 mg/day). Vancomycin trough levels ranged between 7 and 21.7 µg/mL. Standard blood culture from admission returned positive for Rothia mucilaginosa in one lumen of double lumen broviac. He completed 10 days of IV vancomycin (1 g every 6 h) and received 5 days of ethanol locks to both lumens of central line with rapid clearance of his bacteremia. All his symptoms seemed to improve except that he continued to be febrile up to 40o C daily, prompting further infectious work-up including Aspergillus galactomannan, Epstein–Barr virus polymerase chain reaction (EBV PCR), Coccidioides titers, cytomegalovirus (CMV) PCR, Quantiferon Gold, respiratory viral panel (RVP) with negative results.
Given 1 week of daily fever despite antimicrobial therapy, he underwent computed tomography (CT) of chest (hospital day 8), which revealed multiple lung nodules with a possible cavitary lesion. Amphotericin B (5 mg/kg/dose daily) was started with improvement in his fever curve initially but became febrile shortly thereafter, prompting video-assisted thoracoscopic surgery (VATS) and lung nodule biopsy with placement of chest tube (hospital day 11). Echocardiogram (ECHO) was normal. He remained on cefepime during the entire course at this time per hospital febrile neutropenia guidelines, being at risk for serious gram-negative infections due to continued fever, without any evidence of count recovery and without another explanation for fever at that time. Pathology reported poorly formed epithelioid granulomas in lung parenchyma and mild chronic inflammation. Lung nodule biopsy cultures for bacteria, legionella, fungal, acid-fast bacilli (AFB) and broad range PCR for bacterial, fungal, AFB, aspergillus, and mucor returned negative.
He remained febrile, neutropenic, and was started on granulocyte macrophage colony-stimulating factor (GM-CSF). His white count remained 0.4 with absolute neutrophil count (ANC) of 200 and C-reactive protein of 12.4 mg/dL (0.1–0.8 mg/dL). Persistent fever considering above negative infectious lab results triggered further work-up including repeat CT chest (hospital day 19) which was notable for increase in size and cavitation of pre-existing lung lesion. Voriconazole (300 mg every 12 h) was added empirically with the thought of rare possibility of amphotericin-resistant fungal organism (discontinued later). He also developed new headache, meningismus with episodes of behavioral change around the same time. CT of head/magnetic resonance imaging (MRI) of brain (hospital day 19) revealed ring-enhancing nodules in multiple lobes with surrounding vasogenic ventriculitis and diffuse cerebritis (Figure 1).

MRI brain imaging.
Lumbar puncture (LP; hospital day 20) revealed intracellular and extracellular structures resembling bacteria and was concerning for meningitis (Table 1).
Lumbar puncture results.

CSF: cerebrospinal fluid; LP: lumbar puncture; WBC: white blood cell; RBC: red blood cell.
The timeline of events from chemotherapy to diagnosis of meningitis is depicted in Figure 2.
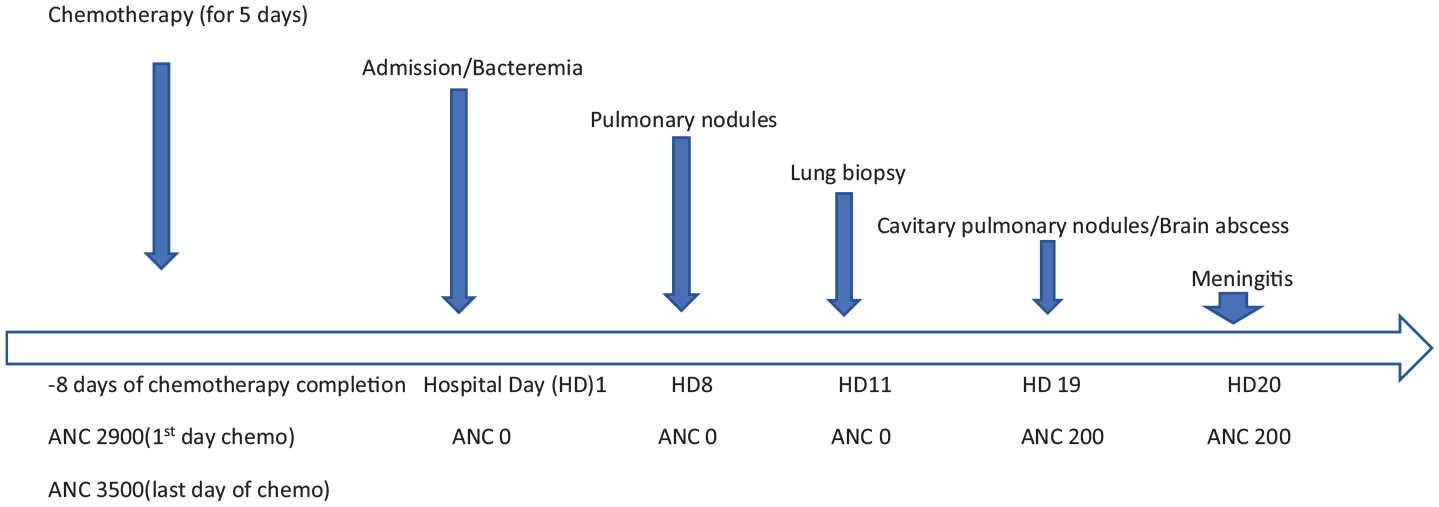
Timeline.
Vancomycin was added while continuing cefepime pending further identification. Standard cerebrospinal fluid (CSF) culture grew Rothia mucilaginosa. Based on previous Rothia blood isolate minimum inhibitory concentration (MIC) and pending MIC on CSF isolate, therapy was changed to high-dose penicillin G (5 million units every 6 h; hospital day 22) and rifampin (600 mg once daily) was added 2 days (hospital day 24) later upon worsening of his mental status along with bilateral upward gaze. Repeat MRI brain (hospital day 24) revealed moderate communicating hydrocephalus and underwent placement of bilateral ventricular external ventricular drains (EVDs). His fever curve improved, along with decreasing CRP. Multiple repeat follow-up CSF cultures were negative. CSF isolate resulted susceptible to penicillin, vancomycin, ceftriaxone, and rifampin (Table 2).
Rothia mucilaginosa MICs.
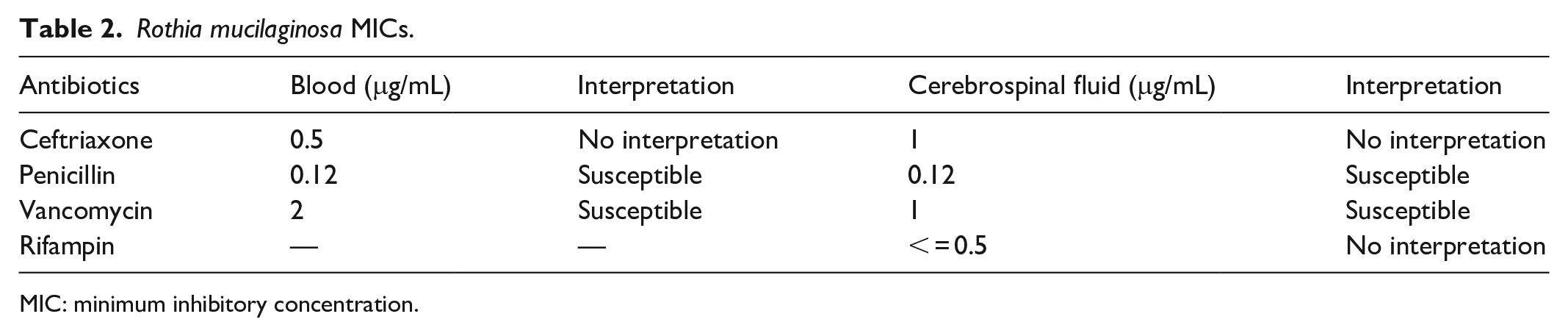
MIC: minimum inhibitory concentration.
He was also started on low-dose steroids (dexamethasone 2 mg every 12 h) by neurosurgery (hospital day 26). Follow-up MRI brain (hospital day 45) revealed significant reduction in lateral ventricular size but increase in the fourth ventricular size raising the possibility of trapped/partially obstructed fourth ventricle by adhesions/infection, but shunt placement was deferred at that point. His mental status seemed to have mildly improved initially but reached a plateau thereafter. After discussion among care team members, the decision was made to increase the dose of steroids (dexamethasone 4 mg every 6 h) after about 3 weeks into therapy. He finally underwent ventriculoperitoneal (VP) shunt placement at 5 weeks into therapy due to continued need for CSF diversion with resultant gradual improvement in his mental status, although he was left with neurological deficits. He completed 6 weeks of antimicrobial therapy.
He received intensive rehabilitation therapy with continued improving neurologic status along with modest ambulatory gains. Given his neurological status, he could no longer be a candidate for bone marrow transplant (BMT) and received palliative chemotherapy. Unfortunately, his AML relapsed and survived only for few months thereafter.
Discussion
Rothia mucilaginosa, (Stomatococcus mucilaginosa), is gram-positive coccus residing in the oral cavity and upper respiratory tract. 1 It forms mucoid, whitish colonies and strictly adhere to agar. The prevalence of this organism may be underestimated due to above characteristics, resulting in difficulty in manipulation and microbiological identification of this organism. It is thought to be of low virulence in immunocompetent population but can behave as an opportunistic pathogen in immune compromised persons including the one receiving chemotherapy. 2 Such patients have multiple predisposing risk factors—presence of central catheter, neutropenia (occasionally profound and prolonged), and mucositis. In addition, the potential risk of selection pressure on body’s microbial flora following the prolonged use of broad-spectrum antibiotics cannot be underestimated as well. Rothia mucilaginosa has the potential to cause sepsis, pneumonia, meningitis, endocarditis, peritonitis, and dermatitis.3–5 Literature review reports treatment with vancomycin, penicillin, ampicillin, second-, or third-generation cephalosporins, imipenem with very few reports on use of rifampin and intrathecal vancomycin in meningitis.6,7 Penicillin resistance has been seen in some cases as well. 8 Other antibiotic options including aminoglycosides, fluoroquinolones, clindamycin, co-trimoxazole have been noted to have higher MICs and should not be considered as empiric choices. 9
His initial clinical course was notable for persistent fever despite rapid clearance of bacteremia. Potential explanations of persistent fever considered at that time included prolonged neutropenia with mucositis resulting in endotoxin release from gram-negative organisms, new bacterial infection but blood cultures remained negative, invasive fungal infection with finding of lung nodule as he seemed to defervesce for few days while on empiric broad antifungal therapy. However, the later course with findings of additional parenchymal brain lesions including meningitis suggested the high likelihood of initial seeding of his lungs and brain with Rothia mucilaginosa. Pulmonary lesions could have been septic emboli from initial Rothia bacteremia, which could have been misinterpreted as fungal pulmonary infection initially.
Penicillin and cephalosporins have comparable CNS penetration, being poor without inflammation but improves with inflammation especially with increased doses of these medications. 10 Although cefepime (fourth-generation cephalosporin) has good pulmonary and CSF penetration and has gram-positive coverage but third-generation cephalosporin may perform better in gram-positive infections in general. It is likely that diagnosis of meningitis was delayed due to lack of significant neurological symptoms from lack of inflammation secondary to neutropenia. Even after the diagnosis of meningitis has been confirmed, lack of meningeal inflammation before neutrophils start to recover, can result in poor CSF antibiotic entry. Since initial blood isolate had vancomycin MIC of 2 μg/mL, we decided to start empirically high-dose penicillin (based on blood isolate MIC of 0.12 μg/mL) followed by the addition of rifampin. CSF penetration of rifampin is independent of inflammatory status of meninges due to its lipophilicity. 10 Although high-dose penicillin and vancomycin generally have comparable CNS penetration, but it is difficult to achieve therapeutic levels with vancomycin after intravenous administration due to its narrow therapeutic index. 11 However, effective CNS vancomycin levels can be achieved with high-dose continuous infusion (60 mg/kg/day). When combined with intraventricular therapy, CNS concentrations of vancomycin are much greater. 11
The question of additional benefit of intrathecal antibiotics was raised as well. However, we decided against its use due to improvement of CSF parameters, absence of bacteria on microscopic evaluation and bacterial cultures on subsequent cultures. The change to high-dose penicillin and rifampin also coincided with his count recovery, which may have aided in achieving therapeutic CNS antibiotic concentration.
Based on literature review, it may be reasonable to empirically treat Rothia mucilaginosa meningitis with vancomycin and or third-generation cephalosporin pending MIC results. However, if therapeutic vancomycin level cannot be achieved or if third-generation cephalosporin cannot be used, then empirical high-dose penicillin along with rifampin pending MIC results could be considered if previous MIC isolates (if available) reveal penicillin susceptibility. Intrathecal vancomycin could be reserved for those failing systemic therapy due to potential challenges in achieving therapeutic CSF levels with vancomycin along with reviewing risks outweighing the benefits of this route. It would be reasonable to consider the additional use of G-CSF for restoration of neutrophil function along with the optimization of antimicrobial therapy.
At some point, we also struggled with the decision whether steroids would be beneficial for his neurological condition. Steroids were not added initially due to theoretical concern of decreasing inflammation, thus decreasing CSF antibiotic penetration. However, they were added later to decrease inflammation-related effects, once CSF cultures were sterile, due to plateauing of his recovery. We believe that earlier CSF diversion would be beneficial in these situations.
We also propose that lumbar puncture and head imaging should be included in the work-up of persistently febrile neutropenic patient without obvious explanation due to delayed signs and symptoms. Every effort should be made to obtain biopsy of tissue for pathology, cultures, and PCR for definitive diagnosis as susceptibility information can guide targeted therapy if an organism is identified in culture. However, in certain circumstances when biopsy cannot be obtained, one could consider newer, sensitive molecular diagnostic tests involving next-generation sequencing (NGS) to assist with early diagnosis of infections although it would lack susceptibility data. We also wonder if broad-spectrum antibiotic prophylaxis will result in shift of host microbial flora and patients will potentially experience infections with new organisms.
Conclusion
This case highlights the importance of considering broad spectrum of clinical presentations by Rothia mucilaginosa in an immunocompromised host. Head imaging and lumbar puncture should be strongly considered during work-up of persistently febrile neutropenic patient even without obvious neurological symptoms especially if there is recent history of bacteremia to assist with early diagnosis of intracranial infection in this type of host. Every effort should be made to obtain tissue diagnosis in case of dissemination to assist with targeted therapy. Various treatment options for this bacterium include penicillin (if susceptible), vancomycin, third-generation cephalosporins and addition of rifampin (in cases of meningitis) could be considered on case-by-case basis.
Footnotes
Acknowledgements
We acknowledge the willingness of the patient’s family for letting us share his clinical course to enhance the existing knowledge on management of Rothia mucilaginosa infections.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical Committee approval not required at our institution due to nature of article submission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
A written informed consent for patient information and images to be published was provided by the patient(s) or a legally authorized representative.