
Abstract
Carcinoma en cuirasse is a rare form of cutaneous metastasis characterized by the spread of a primary malignant tumor to the skin, most commonly associated with breast cancer in women. It may present as papulonodular lesions, erysipeloid, sclerodermiform infiltration, or en cuirassed, typically appearing months or years after the initial diagnosis of the primary malignancy. Diagnosis of carcinoma en cuirasse can be challenging, but histology can help distinguish it from other skin conditions. Treatment options for carcinoma en cuirasse are not well-defined due to the limited number of reported cases. Here, we report a case of a 30-year-old female, who presented with invasive ductal carcinoma which presented as carcinoma en cuirasse with a spoke-wheel pattern over the course of 6 months.
Introduction
Carcinoma en cuirasse (CeC) is an infrequent manifestation of skin metastasis, often originating from breast cancer and, less commonly, from primary lung, gastrointestinal, or genitourinary cancers. 1 Although the incidence of CeC in breast cancer patients is only about 6%, it is a condition that warrants prompt recognition and management. 2 CeC is caused by the invasion of cutaneous lymphatics, which initially appear as skin nodules that coalesce and subsequently diffuse to indurate the skin through thickening, edema, and fibrosis of the dermis and subcutis of the chest wall and abdomen. 3
CeC usually emerges after the initial treatment of the primary tumor, although in other cases, it may be the first manifestation of a rapidly evolving internal malignancy, underscoring the need for early identification and diagnosis. 4 We present a case of a patient who developed CeC following a 5-month history of bilateral breast pain, redness, and induration, and we discuss the diagnostic and therapeutic approaches that were undertaken. This report is intended to raise awareness among clinicians of the clinical features, diagnostic considerations, and potential management options for CeC, a rare but significant dermatologic complication of malignancy.
Case presentation
A 30-year-old South-Asian woman, multiparous and resident of India, presented to the surgical outpatient department with a complaint of pain in her left and right breast for the past 5 months, with redness and hardness on both breasts for the past 2 months. The patient reported the spread of these symptoms to the cervical, axillary, and left forearm regions. The patient had a history of using over-the-counter skin preparations, including steroids, ayurvedic creams, topical herbal medication use, and antihistamines, for early dermatological presentation, until the disease reached the presenting proportions. On local examination, the bilateral breast showed diffuse enlargement with erythema and pigmentary changes resembling a spoke-wheel pattern (Figure 1). The patient reported using herbal topical treatments for approximately 2 weeks to alleviate inflammation and erythema. However, instead of subsiding, the inflammation persisted and the skin lesions developed into a prominent hyperpigmented spoke-wheel pattern. The examination revealed tender, firm hard nodularity over both breasts and lymphedema of the left arm. Bilateral palpable axillary lymph nodes were also present. Ultrasound revealed inflammatory breast carcinoma of the bilateral breasts. A fine needle aspiration cytology was performed on the axillary lymph nodes, and a Trucut biopsy was utilized to obtain specimens from the elevated “spoke-wheel” area of the breast tissue. Morphological findings included the raised hyperpigmented “spoke-wheel” and erythema present in areas of the upper trunk including the bilateral upper arms, and cervical, and axillary regions. Histopathology examination revealed dense pleomorphism and anisonucleosis. The cells had scanty cytoplasm and large hyperchromatic nuclei with prominent nucleoli (Figure 2), and dense fibrous-collagenous bundles showing round to polygonal cells with no significant tubule formation (Figure 3), signifying malignant cells with few clear cytoplasm from aspirate sites. Based on the cytological findings, with cutaneous metastasis, a cytodiagnosis of stage 4 invasive ductal carcinoma of the breast with CeC was made. The patient was referred to an oncology center and was receiving palliative treatment with doxorubicin and paclitaxel, with three cycles completed at the last follow-up.

Diffuse enlargement of the bilateral breast with erythema and pigmentary changes resembling spoke-wheel pattern and associated nodularity.
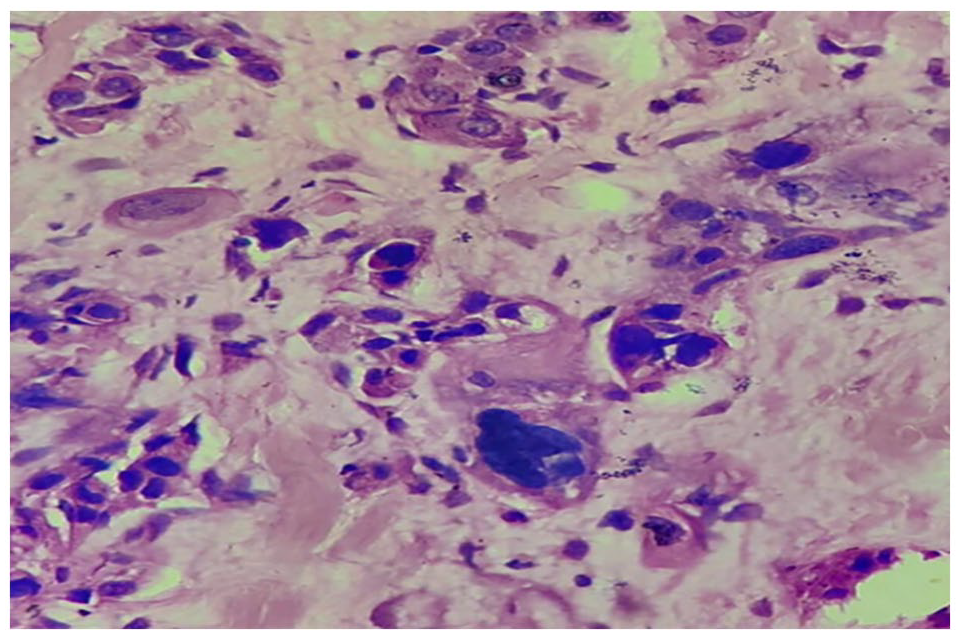
Histopathological finding—oval and spindled tumor cells (white arrow) with pleomorphic, hyperchromatic, and inconspicuous nuclei with scant-to-moderate amounts of indistinct basophilic cytoplasm.

Histopathological finding—large tumor cells with pleomorphic and hyperchromatic nuclei and scanty cytoplasm.
Discussion
Cutaneous metastasis occurs in about 10% of all cancer patients, taking various forms depending on the primary malignancy. 5 It can also be the initial presentation of malignancy in 37% of men and 6% of women. 4 The most common malignancy to metastasize to the skin in women is breast cancer, manifesting in the form of papulonodular lesions, alopecia neoplastica, erysipeloid inflammatory plaques, or carcinoma en cuirasse. 3 CeC is a rare type of skin metastasis mostly seen in breast cancer and, less frequently, in primary lung, gastrointestinal, or genitourinary cancers.1,3 CeC has an incidence of about 6% in breast cancer patients 2 and was first described in 1838 by Dr. Alfred Velpeau, who called the condition “en cuirasse” since it resembled breastplate armor worn on the chest. 6 The exact pathogenesis of CeC is unknown, though researchers hypothesize it is due to the activation of stromal fibroblasts by an extracellular signaling molecule known as pleiotrophin. 7
The differential diagnosis for CeC includes morphea, chronic radiation dermatitis, keloids, and other cutaneous metastases. Thus, obtaining a biopsy and observing a lesion’s histology is crucial when differentiating these diseases from one another. In morphea, for instance, there are thickened hyalinized collagen bundles and loss of adventitial fat. Chronic radiation dermatitis appears similar to morphea under a microscope but with large stellate fibroblasts present amidst the collagen bundles. Keloids show whorls of collagen and fibroblasts, with thick hyalinized collagen that resembles “bubble gum.” CeC appears as a fibrotic stroma with single rows of tumor cells between the collagen bundles. The tumor cells appear very similar to fibroblasts, which can sometimes deceive pathologists into overlooking them.3,5
CeC usually holds a bad prognosis since it indicates a late stage of breast cancer. There’s no definitive treatment for CeC due to the scarcity of cases and the advanced stage of primary malignancy accompanying the disease. Furthermore, the extensive fibrosis in the lesion can prove a major obstacle for treatment modalities to reach the lesion uniformly, compromising the use of chemotherapy, radiotherapy, and hormonal antagonists, all of which had been tried and failed in previous case reports.6,8,9 In one report, physicians used a remedy called VRCTC-310, a combination of snake venom crotoxin and cardiotoxin, in a woman with CeC and reduced the tumor mass by more than 80% after just 6 weeks of treatment. 10 Since CeC indicates a late stage of breast cancer, the role of surgery and breast reconstruction is minimal. Although a higher stage of the disease isn’t a contraindication to breast reconstruction, patients and physicians may not regard such a procedure as a high priority compared to treatment. 1
Conclusion
The prognosis of cutaneous metastasis is dependent on the type and biological behavior of the primary tumor that underlies it. Although rare, cutaneous metastasis as the initial presentation of an undiagnosed internal malignancy can occur, as demonstrated in this case report. The discovery of a spoke-wheel-patterned nodular lesion on bilateral breasts is a unique dermatological finding that has not been previously reported in the literature. The association of breast carcinoma with skin metastasis typically indicates advanced cancer and poor prognosis. Therefore, early recognition and thorough investigation of cutaneous metastasis are crucial for optimal outcomes.
Footnotes
Acknowledgements
None.
Author contributions
S.B., C.H., T.S.H., and Y.V. were involved in the study concept, the collection of the data, drafting, literature review, data validation, supervision, and editing of the manuscript. H.M., H.S., A.N., and P.S. were responsible for the literature review and revising the manuscript for important intellectual content.
Data availability statement
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Clinical trial registration
None.