
Abstract
Tuberculosis presenting as monoarticular involvement in immunocompetent patients is rare. Here, we report a Sri Lankan patient presenting with ankle swelling due to tuberculosis with no other extrapulmonary or pulmonary involvement. Magnetic resonance imaging showed destruction of articular cartilage of the ankle joint with chronic inflammation of the subtalar joint. The diagnosis was confirmed by synovial tissue culture which was positive for Mycobacterium tuberculosis. The patient recovered uneventfully with anti-tuberculosis treatment. Therefore, a high degree of suspicion is necessary to diagnose extrapulmonary tuberculosis when patients are presenting with atypical monoarthritis.
Introduction
Despite dramatic decline of global mortality due to tuberculosis since 20th century, it continues to be a devastating public health concern in South East Asian and African countries, making tuberculosis a leading cause for ill-health in these regions. 1 Skeletal tuberculosis is a less common extrapulmonary manifestation of the disease which can cause monoarticular involvement. 2 Isolated involvement of joints encompasses a spectrum of differential diagnoses such as infectious, inflammatory or neoplastic processes, where a high degree of suspicion is necessary for the diagnosis of tuberculous involvement.2,3 Here, we report a rare presentation of ankle joint monoarthritis due to tuberculosis without pulmonary involvement.
Case
A 44-year-old otherwise healthy Sri Lankan male presented with left ankle joint swelling of 6 months duration. He had progressive ankle swelling with restricted movement and pain while weight-bearing. He denied any respiratory symptoms, pyrexia and constitutional symptoms. Patient did not have a history of previous trauma or surgery. On examination, his left ankle joint was swollen without tenderness or warmth (Figure 1). There was global restriction of movements at the ankle joint. Apart from this, the general physical examination was unremarkable. His basic haematological tests were normal; however, his erythrocyte sedimentation rate (ESR) was 35 mm in the first hour. A Mantoux test was performed and it was positive with an induration of 18 mm. However, Ziehl–Neelsen stain for acid-fast bacilli was negative and the chest X-ray was unremarkable. Arthritis workup with rheumatoid factor (RF), anti-cyclic citrullinated peptide antibody (anti-CCP), and antinuclear antibody (ANA) was negative. His fasting blood sugar level was normal and retroviral screening was negative. X-ray of the ankle region showed irregular outline at ankle mortise and loss of joint space with an irregular articular outline at subtalar joint (Figure 2). The magnetic resonance imaging (MRI) showed a marked loss of articular cartilage with associated bone marrow oedema in the subarticular region of distal tibia extending to distal metaphyseal region (Figure 3). The subtalar joint also showed evidence of chronic inflammation. Aspiration was not possible due to minimal effusion. Since initial workup, including MRI, was inconclusive, the patient underwent open synovial biopsy which showed granulomatous type of inflammation without any Langhans type of giant cells or associated caseating granulomas. Xpert MTB/RIF test was negative; however, culture for mycobacteria was positive for Mycobacterium tuberculosis. The ankle was splinted with a back slab and was kept non-weight-bearing for the initial 2 months, followed by gradual mobilisation. Anti-tuberculosis treatment was initiated immediately after the synovial biopsy result, that is, 7 weeks after the initial presentation. Patient was treated for 2 months with isoniazid 300 mg, rifampicin 600 mg, pyrazinamide 1500 mg, and ethambutol 800 mg once daily (intensive phase), followed by 7 more months with isoniazid 300 mg and rifampicin 600 mg once daily (continuation phase). With anti-tuberculosis treatment and physiotherapy, his pain and swelling improved dramatically and he was able to bear weight by 3 months of treatment. Patient completed anti-tuberculosis treatment at 9 months and remains asymptomatic after 1-year follow-up. A repeat MRI was not performed since patient clinically improved.

Anterior view of the left ankle joint with swelling.

Anteroposterior and lateral views of left ankle joint showing narrowed joint space and subtalar joint involvement.

MR image of the ankle joint showing marked loss of articular cartilage with associated bone marrow oedema in the subarticular region of the distal tibia.
Discussion
Epidemiology and risk factors
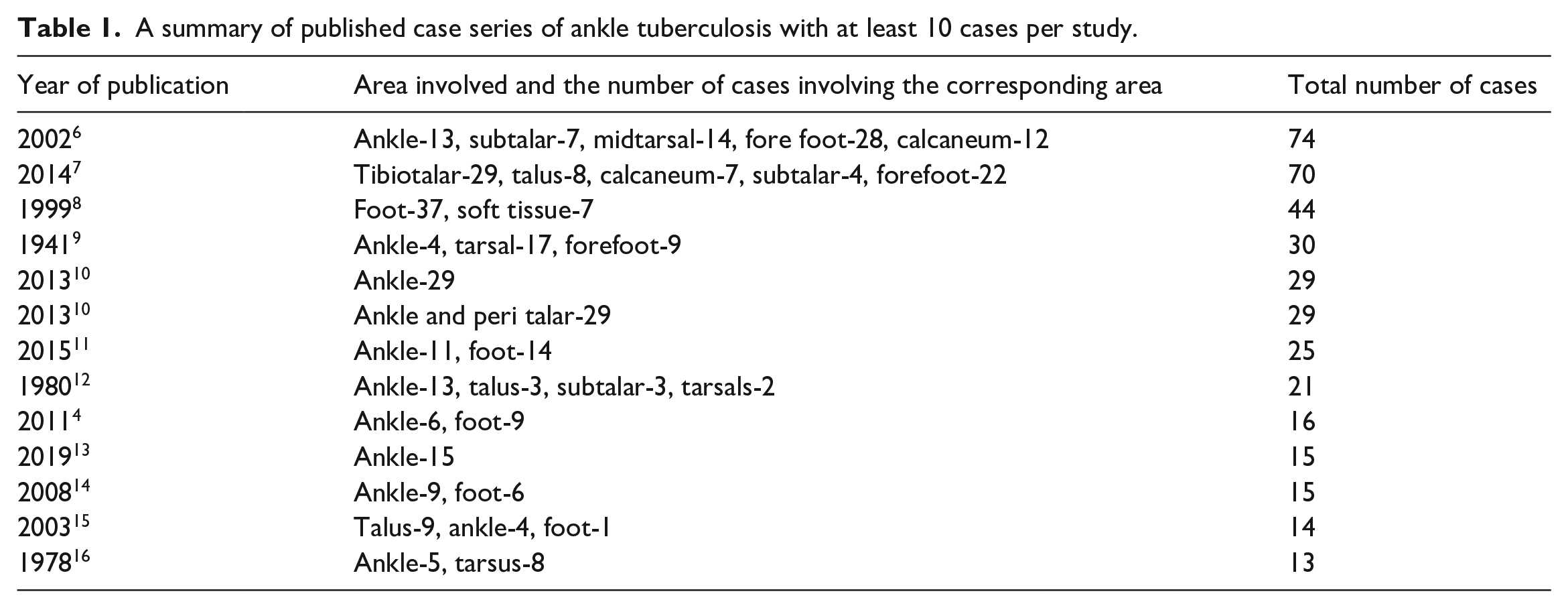
The incidence of the skeletal involvement is reported to be up to 11.3% of the cases with tuberculosis infection, 1 with half of the cases affecting the vertebral column.4,5 Osteomyelitis of the bones of the involved joints is seen in approximately 98% of the times. 1 Weight-bearing joints such as hip and knee are affected frequently in monoarticular tuberculosis, 1 while ankle joint is rarely involved.4,5 Published case series of tuberculosis involving the ankle joint are summarised in the Table 1. Immunocompromised status secondary to HIV infection, malnutrition, smoking and long-term immunosuppressive therapy for autoimmune diseases, malignancies, renal failure, extreme ages and organ transplant as well as emerging resistance of the M. tuberculosis complex for the anti-tuberculosis treatment have contributed significantly for the involvement of the skeletal systems.5,17
A summary of published case series of ankle tuberculosis with at least 10 cases per study.
Pathogenesis
M. tuberculosis bacilli disseminate haematogenously and seed the joints, with a special predilection to the joints with a history of recent trauma and/or inflammation, possibly due to the high vascularity. 6 Moreover, prosthetic joints are also predisposed to tuberculous monoarthritis. 18 Of foot and ankle involvement with M. tuberculosis, the calcaneum has the highest reported incidence, probably because it is the most vascular bone of the foot, while it is continuously subjected to the stresses as it contacts the ground. 19 Once the bone or the synovium is seeded, the bacilli may progressively infect the tissues or remain dormant to be reactivated when the patient’s immunity is suppressed. 20 If the synovium is seeded first, the lesion gradually evolves to become a pannus and spreads through the articular cartilage to reach the subchondral region. 4 Alternatively, if only the bone is seeded, the granulation tissue will directly spread through the bone to the subchondral region. 21 Once the subchondral region is invaded by the granulation tissue, the articular cartilage may detach from the adjoining bone, 5 leading to joint collapse and secondary degenerative changes. 22 However, the cartilage may remain viable for a long duration without undergoing proteolysis.4,5
Pathological classification of articular tuberculosis
Martini and Ouahes proposed four stages of articular tuberculosis which was later modified by Chen et al. 10 In the first stage, infection is confined mostly to the synovial lining with no substantial bony erosion or localised osteoporosis. The second stage is characterised by noticeable erosions or areas of tuberculous osteomyelitis, with no reduction of joint space. The third stage has further synovial and bony involvement with collapse of joint space. The fourth stage is characterised by involvement of adjacent joint surfaces or concomitant pyogenic arthritis with significant disorganisation of bony architecture.10,22
Clinical features
The resultant chronic inflammation gives rise to the characteristic myriad of clinical symptoms and signs: pain, swelling, redness and restriction of the range of motion of the affected joint. Inguinal lymphadenopathy could be seen in some. 22 Discharging sinuses and ankylosis are found in advanced cases. 22 Systemic symptoms such as fever, night sweats, malaise, loss of weight and loss of appetite may accompany local inflammatory signs and symptoms suggestive of tuberculosis. Traumatic arthritis, chronic pyogenic arthritis, rheumatoid arthritis, Charcot arthropathy, psoriatic arthropathy, pigmented villonodular synovitis, amyloidosis, sarcoidosis and neoplasms (benign and malignant) are some of the differential diagnoses for ankle tuberculosis.4,10,14,22,23 Atypical presentations of ankle tuberculosis frequently cause diagnostic challenges. Therefore, a high degree of suspicion is necessary in atypical presentations of monoarthritis. Isolated joint involvement by tuberculosis in immunocompetent subjects are rare. 24 In our patient, there was no history suggestive of pulmonary tuberculosis or an immunocompromised status which could alert the diagnosis of tuberculosis, except that he was a citizen of a tuberculosis endemic country. As reflected in our case, the prompt diagnosis and timely initiation of anti-tuberculosis treatment are extremely important to achieve a good outcome.
Investigations
Radiographic changes usually require 2–5 months from the onset of disease.14,25 One of the earliest features seen on a plain radiograph is joint effusions.14,25 Plain radiographs may show articular erosions in advanced disease as in our patient. 15 Nonetheless, the majority of the features detected on a plain X-ray are non-specific. 4 MRI is the preferred modality of imaging in skeletal tuberculosis which has a better diagnostic accuracy than plain radiographs or computed tomography (CT). 2 Joint oedema, effusions, periarticular osteopenia, capsular and synovial thickening, paraosseous masses and subchondral lytic lesions are seen on magnetic resonance (MR) images in tuberculous arthritis.10,15 Joint space narrowing is characteristically seen in advanced cases secondary to collapsing of the articular cartilage. 10 In addition to the ankle joint, there was MR evidence of the involvement of subtalar joint in our patient. According to the previous reports, tuberculosis can affect multiple joints in the foot apart from these two joints. 26 In addition to the diagnosis and the assessment of the extent of the tuberculosis of the ankle joint, MRI is also useful to determine the response to treatment. 15
Acid-fast bacilli culture is usually negative in cases with tuberculous monoarthritis involving the ankle joint.4,6 Therefore, the diagnosis is confirmed by the presence of caseating granulomas with characteristic Langhans type giant cells on biopsy.4,6 In a case series, only 50% of the patients with ankle joint tuberculosis were culture positive while all demonstrated caseating necrosis histopathologically. 4 Intriguingly, however, we observed neither caseating necrosis nor Langhans giant cells in the synovial biopsy. Nevertheless, the tissue culture was positive for M. tuberculosis. However, it may take several weeks for the acid-fast culture of the harvested tissues to become positive for the organism. 27 In contrast, the Xpert MTB/RIF test enables rapid detection of amplified nucleic acid sequences specific for M. tuberculosis and related Mycobacterial complexes within a matter of few hours. 28 Nonetheless, the efficacy of these nucleic acid amplification assays is not very well established in samples other than sputum. 29 Likewise, we did not detect the presence of the organism in our patient using this technique. Due to delays in obtaining microbiological or histological diagnosis, suggestive clinicoradiological features often warrant initiation of treatment.8,30
Management
Atypical presentation of ankle tuberculosis may often cause a diagnostic dilemma leading to delayed initiation of treatment. 14 The reported average delay in the diagnosis of ankle joint tuberculosis varies from 12 to 24 months in several case series.4,10,14,22 The treatment of tuberculous monoarthritis is mainly conservative. The anti-tuberculous treatment should be decided on the regional antimicrobial sensitivity patterns and the previous history of treatment, if any.5,6 The duration of anti-tuberculous treatment for ankle tuberculosis in the previous reports are highly variable ranging from 6 to 18 months.19,31 Prolonged chemotherapy is often justified since osteoarticular tuberculosis, predominantly being paucibacillary with dormant bacilli, hence resistant to anti-tuberculous treatment.19,32 Early diagnosis is a major prognostic determinant of ankle tuberculosis.33,34 The combination of physiotherapy and occupational therapy with the pharmacological management may improve clinical outcomes. Noticeably, radiological resolution often lags behind clinical healing process. 6 The surgical interventions are necessary in cases complicated with joint abscesses, tenosynovitis and loss of bone and joint architecture. 10 Early debridement reduces the bacterial load, helps penetration of anti-tuberculous treatment and improves prognosis. 35 Arthroscopy is increasingly being utilised compared with open surgery since it is associated with less morbidity, less postoperative pain and fast rehabilitation.35,36 A follow-up of 29 cases who underwent surgical interventions for ankle tuberculosis resulted in good long-term surgical outcomes, with less than 6 patients being complicated by either hind foot malalignment or talar bone collapse postoperatively. 10 Arthrodesis of ankle and other foot joints can be considered in advanced cases where bony stability is severely compromised for weight-bearing. 6
Conclusion
Tuberculosis is a rare cause of chronic inflammatory monoarthritis; nevertheless, a high degree of suspicion is necessary in Asian and African countries where the disease is endemic. Timely diagnosis and treatment may result in rapid clinical improvement of this disease entity.
Footnotes
Data availability
All data provided in this manuscript will be available upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for his anonymized information to be published in this article.