
Abstract
A 39-year-old G3P3 female presented with abrupt onset dyspnoea of one month duration. She was markedly symptomatic when lying supine and resorted to prone sleeping. Chest X-ray reported as cardiomegaly. Transthoracic echocardiography was unremarkable twice. Computed tomography chest showed a dilated pulmonary artery. Transesophageal echocardiography identified a 12-mm ostium secundum atrial septal defect with mild pulmonary hypertension. The defect was closed with a cocoon device and rendered her symptom free. This case highlights the importance of timely organization of transesophageal echocardiography when transthoracic echocardiography is negative. It also illustrates marked dyspnoea could be a presentation of undiagnosed atrial septal defect with mild pulmonary hypertension.
Introduction
Undiagnosed atrial septal defects (ASDs) are associated with a reduced life span. It is not unusual for an adult to have an ASD without being diagnosed, despite having had uneventful pregnancies. 1 Dyspnoea related to ASD is known to develop gradually after fourth decade.2,3 On contrary, patient may present abruptly with dyspnoea due to the development of pulmonary hypertension irrespective of the severity. 3 Potential complications of an undetected ASD are irreversible pulmonary hypertension, right ventricular failure, atrial arrhythmias, paradoxical embolization and cerebral abscess formation.2,3 Thus, timely diagnosis and closure of the defect is of paramount importance. 4
Case presentation
A 39-year-old G3P3 female presented with a history of relatively abrupt onset shortness of breath getting worse towards the end of the day for 1 month. She complained of marked orthopnoea in supine position relieved by sleeping prone. There were no respiratory symptoms and no chest tightness or palpitations. She had no other medical problems, and all three deliveries were uncomplicated and normal. There was no family history of young cardiac deaths or cardiovascular events. Her blood pressure was 110/70 mm Hg, pulse rate was 80 bpm, respiratory rate was 22/min and oxygen saturation was 100% on room air in supine, erect and prone positions. Single breath count was 7 indicating poor respiratory status. On examination, cardiovascular system was unremarkable except for an ejection murmur at pulmonary area and clear lungs. The basic metabolic panel including haemoglobin and renal functions was normal, and serum lactate dehydrogenase (LDH) was 289 U/L which was mildly raised. Her electrocardiograph (ECG) and chest X-ray (CXR) posteroanterior view are shown in Figures 1 and 2, respectively. Transthoracic echocardiography (TTE) was unremarkable twice with normal right and left heart functions and dimensions. The brain natriuretic peptide (BNP) levels were not done as the patient could not afford to pay for it. The patient could not complete pulmonary function tests because of marked dyspnoea. But she underwent imaging of chest which included high-resolution computed tomography (HRCT), CT chest with CT pulmonary angiogram (CTPA). HRCT and CT chest were normal but CTPA showed a dilated pulmonary artery of 31 mm where up to 29 mm was considered normal and the diameter of aorta was 23 mm. The possibility of chronic thromboembolism was also ruled out as there were no filling defects in the pulmonary vasculature when traced up to the terminal bifurcations. As none of the investigations failed to elucidate the reason behind her symptoms, the cardiologists expedited the transesophageal echocardiography (TOE). The TOE revealed an ASD 10 × 12 mm with a left-to-right shunt (Figure 3). Subsequently, she underwent right heart catheterization which reconfirmed the findings of TOE. Additional findings were mean pulmonary artery (MPA) pressure of 28 mm Hg (46/16 mm Hg) and right ventricular (RV) pressure of 49 mm Hg. This defect was successfully closed with a cocoon device and rendered her symptom free with a single breath count 35. Three months postprocedure, two-dimensional (2D) echocardiograph revealed a myxomatous mitral valve prolapse with mitral regurgitation but normal right ventricular function.

Normal ECG.
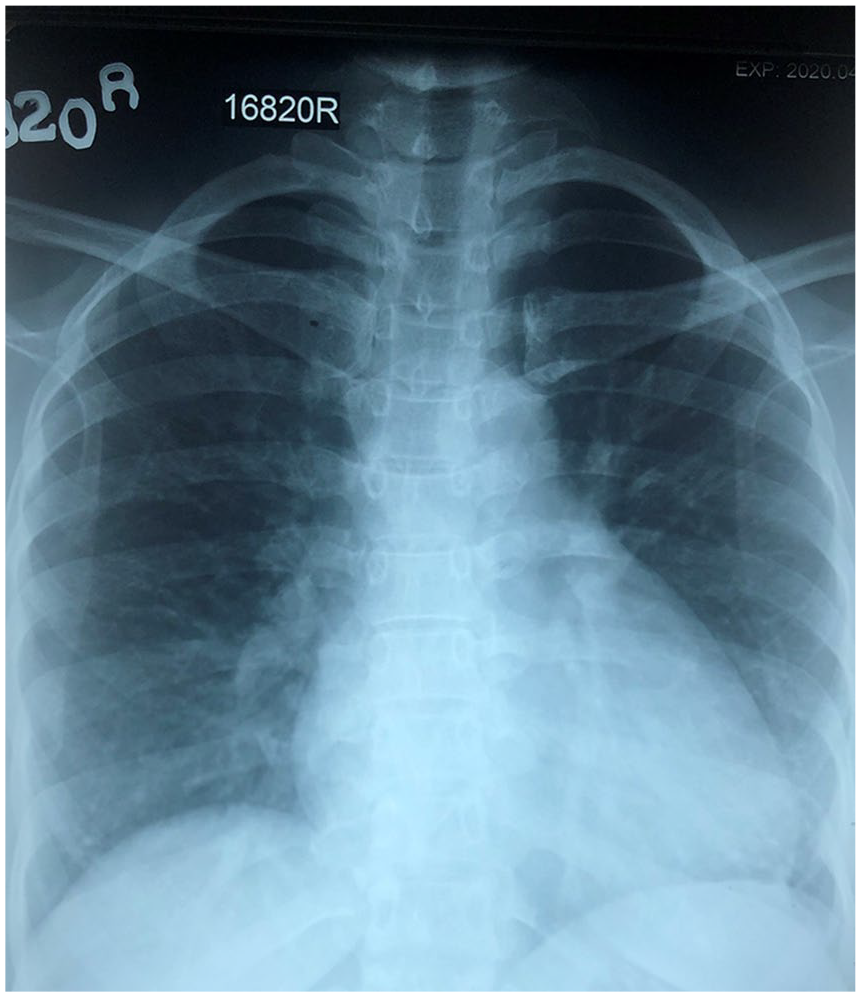
Chest X-ray A/P view showing mild cardiomegaly with obliteration of pulmonary artery bay.
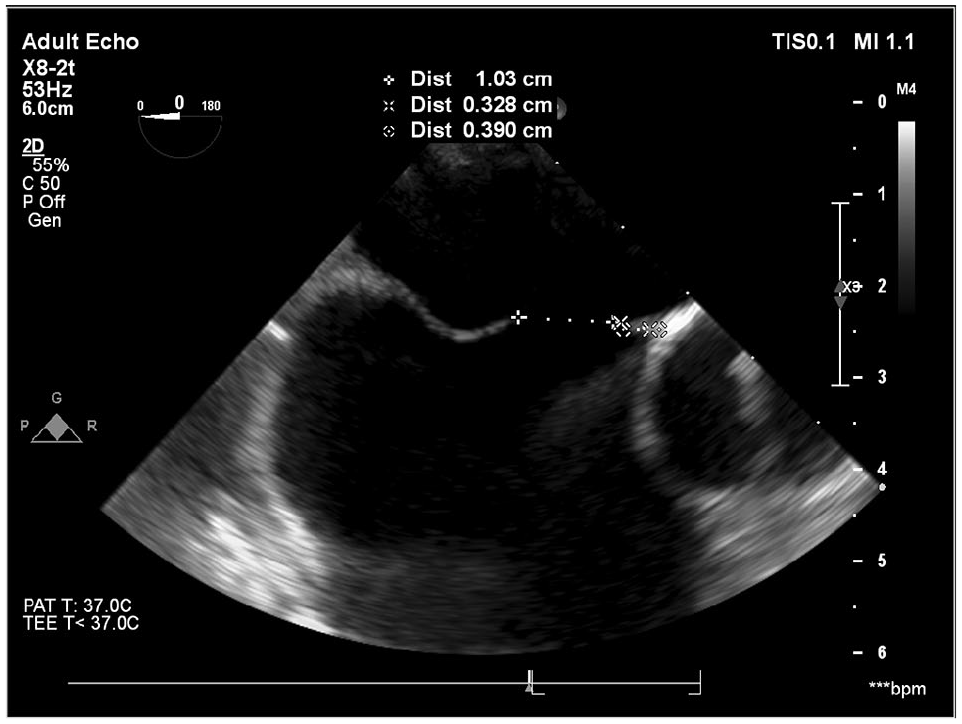
TOE showing the ostium secundum ASD.
Discussion
Chronic dyspnoea is defined as shortness of breath lasting more than 4 weeks. In a multiparous healthy female, the differential diagnosis can be broadly divided into cardiac, pulmonary, neuromuscular, metabolic and multifactorial causes. Diagnosis is always a challenge when the clinical assessment does not correlate with the findings of basic and specialized investigations as expected.
Not only comprehensive history but also critical analysis of symptoms is vital to any diagnosis. Cardiac pathology is high on the cards in the absence of respiratory symptoms, past history of wheezing or muscular weakness. Among cardiac related symptoms, presence of orthopnoea has a positive predictive value of 72% for heart failure. 5 Orthopnoea is described as shortness of breath on lying down due to an increase of blood volume drained from the heart and pooled in legs. Whether lying prone has an impact on orthopnoea in certain conditions is yet to be discovered. But it is well established that prone position improves gas exchange in adult respiratory distress syndrome (ARDS) due to increase in alveolar capillary units. 6 Similarly, in pulmonary hypertension, the prone position is thought to improve gas exchange as well. 7 Thus, for anyone, whose dyspnoea gets better when lying prone could be explained by recruitment of functioning alveolar units in the prone position. Mild pulmonary hypertension is hardly symptomatic making early diagnosis difficult unless suspected. But it too can present with New York Heart Association (NYHA) class 3–4 symptoms. 8 This is especially true as undiagnosed ASD can present abruptly in weeks or months with the development of pulmonary hypertension 2
Thorough clinical examination adds value to the history. Finding of cardiac murmurs is a highly sensitive sign for valvular heart disease (negative predictive value: 97%) but has a low specificity when present. 5 Similarly, absence of respiratory signs does not negate the possibility of respiratory disease as well.
There is an array of simple to complex investigations and different algorithms that help us to nail down a case of chronic dyspnoea. 5 Once basic investigations rule out anaemia and acid base disorders, the CXR and ECG play an important rule to narrow diagnosis. In suspected cardiac failure, CXR may indicate pulmonary oedema or increase cardiothoracic ratio but the findings of CXR P/A may not be always proportional to the symptoms. 5 Nevertheless, in resource-poor setting, the cardiothoracic ratio can be a very helpful tool to ascertain the cause of dyspnoea. 9 Although BNP is considered a first-line investigation to detect myocyte strain, it is not freely or readily available in Third World countries like us due to high cost.
Secondary investigations like TTE and CT imaging have to be performed, especially if the first-line basic investigations are normal. TTE assesses the structure and function of the heart. But the sensitivity and specificity of transthoracic echo in detecting ASD is 85% and 99%, respectively. 10 Several factors affect the sensitivity of detection of ASD by TTE, 10 namely, the echo machine, acoustic windows, ultra-sonographer, the characteristics of the shunt and so on. 10 Although the accuracy of diagnosis of ASD with the agitated saline method is 100%, it depends on the quality of manoeuvre. 11 Pulmonary hypertension in early stages is difficult to recognize on routine TTE.11,12 Therefore, right heart catheterization is the only modality to get an accurate reading on pulmonary hypertension when in doubt.11,12 On the other hand, CT chest and HRCT have high sensitivity in detecting a pulmonary condition. 13 CTPA is the investigation of choice to detect acute pulmonary embolism; however, CTPA can also be used in suspected chronic thromboembolic pulmonary hypertension (CTEPH). 5 These are especially important when one cannot obtain a proper lung function tests and lung scintigraphy studies.
Unfortunately, the place of TOE when investigating chronic dyspnoea is not well established. 5 The guidelines recommend TOE as a preprocedural assessment method of ASD rather than a diagnostic method. 14
The likely explanation to this patient who presented with NYHA class 3–4 dyspnoea and orthopnoea which improved in the prone position can be the development of pulmonary hypertension secondary to long-standing ASD. Cardiomegaly seen on the CXR P/A with obliteration of pulmonary artery bay indicated some volume overload to the main pulmonary trunk and implied her underlying issue correctly. CTPA confirmed a dilated pulmonary artery and was in agreement with CXR P/A findings. But TTE failed twice in identification of the defect. Last but not least, TOE captured the ASD which otherwise would have been missed and picked up at a later stage when nothing else could be done.
Conclusion
Timely organization of TOE is important in a middle-aged lady with dyspnoea possibly arising from heart without a clear explanation. This is especially important if TTE is normal as ASDs with minimal or early complications can be missed. Further mild pulmonary hypertension can present with NYHA class 3–4 symptoms which can be overlooked.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.