
Abstract
Placenta accreta spectrum encompasses a group of conditions of abnormal placental infiltration of the uterine wall and surrounding tissues. It is associated with significant blood loss, perioperative morbidity, and risk of death. A coordinated interdisciplinary approach to these complex cases and early resuscitation with blood products are critical factors in the successful management of patients affected by this disease. We describe the successful management of a patient with placenta percreta who required supra-massive transfusion of blood products and interventions by different specialized teams in a tertiary care center.
Introduction
Maternal hemorrhage due to placenta accreta spectrum (PAS) is associated with significant morbidity and mortality and represents a challenge to obstetricians and anesthesiologists. 1 In some instances, planned cesarean hysterectomy is the treatment of choice when this complication is anticipated. Despite careful planning, in some cases, exhaustive resuscitation and transfusion of blood products are necessary in order to maintain hemodynamic stability and organ perfusion. Successful resuscitative efforts in these situations are the result of a combination of surgical control of bleeding, administration of fluids and blood products, use of vasoactive medications, and intervention on hemostatic pathways in the context of a coordinated interdisciplinary effort during the perioperative period. 2 Here we present a patient with PAS who underwent cesarean hysterectomy with massive bleeding and supra-massive blood product transfusion. Timely and decisive obstetric and anesthetic actions led to maternal survival and discharge from the hospital.
Case presentation
We present a 37-year-old patient with 36 weeks gestation in her sixth pregnancy. We obtained written consent from the patient for publication of her case. The patient had history of four prior cesarean deliveries. During her current pregnancy, she was diagnosed with possible placenta accreta in the third trimester. Placental ultrasound revealed complete anterior placenta previa and focal areas near the endocervix suggestive of accretism. Magnetic resonance imaging exhibited focal obscuration of normal placental-myometrial aspects anteriorly, which were concerning for placental invasion. The patient was scheduled for cesarean hysterectomy at 36 weeks (Image 1). Pre-anesthetic evaluation revealed controlled hyperthyroidism and right hydronephrosis with normal renal function. The patient was prepared for surgery with three peripheral intravenous catheters and a large-caliber central line. Hypogastric artery balloons were placed prophylactically in the interventional radiology suite. Immediate preoperative ultrasound showed placenta previa with the anterior portion of the placenta extending to the level of the umbilicus. Intraoperative cystoscopy showed vesical distortion and placental infiltration which made ureteral stent placement impossible. Transfundal cesarean section was performed with neonatal Apgar scores of 3, 6, and 8. Immediately thereafter, severely adherent placenta with infiltration of posterior bladder wall was evidenced, such that some placenta had to be left on bladder serosa and muscularis (Image 2). Excessive hemorrhage from adherent placenta occurred. Cystostomy was attempted but was nonfunctional due to multiple clots. The resulting bilateral hydroureter and hydronephrosis caused compression of the right ovarian vein and subsequent high-pressure dilation and rupture of the vein. A suprapubic catheter was placed. Excessive collateral vessels feeding the placenta, arising from the bladder, pelvic sidewalls, vagina, and along the uterus and cervix, caused massive hemorrhage from all sites. Friable tissue with coagulopathy resulted in tears of the left external and common iliac veins. In order to repair the massive bleeding, the left common iliac artery and vein were ligated. The abdomen was packed and the patient taken to the interventional radiology suite for embolization of hypogastric arteries with gelfoam as embolization material. The patient was transferred intubated to the intensive care unit for resuscitation. During the surgical intervention, the blood loss was estimated to be 70 L. The patient received 118 units of red blood cells, 91 units of fresh frozen plasma, 30 units of cryoprecipitate, 90 units of platelets, 3 L of crystalloids, and 42 L of albumin, in addition to 3 L of cell saver. The patient returned to the operating room 24 h later due to abdominal compartment syndrome. Hemostasis was achieved at that point. Her clinical course in the intensive care unit was marked by the evidence of acute lung injury and elevation of bilirubin without liver dysfunction. Of note, the patient arrived to the intensive care unit with normal acid–base status, kidney function, and body temperature. Two days later, the iliac artery catheters were removed. The left common and external iliac arteries were repaired. The patient progressed satisfactorily and was extubated. Vascular surgery found weak Doppler signals on left lower extremities, with normal temperature, capillary refill and neurologic exam. Four months after surgery, the patient complained of mild left thigh pain after walking for a mile. On the same visit, she exhibited strong multiphasic Doppler signals in the posterior tibialis and anterior tibialis arteries, with a weaker multiphasic Doppler signal in the dorsalis pedis artery.

Magnetic resonance imaging (MRI) showing complete placenta previa with focal obscuration of placental-myometrial interface at midline. Placental tissue in contact with the dome of the bladder.
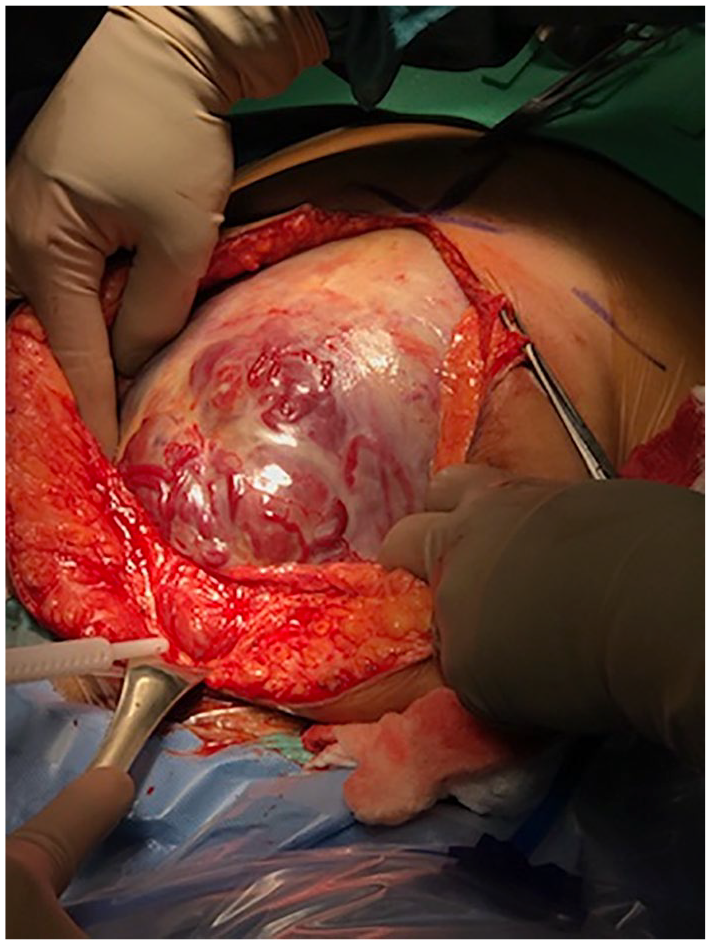
Uterine wall infiltration by morbidly adherent placenta before hysterotomy. No bleeding observed at that time of the operation.
Discussion
PAS can lead to an array of potential circumstances that could result in catastrophe if they coincide. This case highlights the importance of a multidisciplinary approach and extensive preoperative planning in the successful management of PAS. The abnormal invasion of the chorionic villi into and/or beyond the myometrial wall exponentially increases the difficulty of placental detachment after fetal delivery. At the same time, the morbid placental invasion interferes with the myometrial contraction necessary to both control blood flow and facilitate placental detachment. Therefore, failure in physiological hemostatic mechanisms combined with deep and multiple organ involvement results in a challenging scenario requiring multidisciplinary organized intervention with rigorous preoperative planning.
The health care team caring for a patient with abnormally adherent placenta should include patient care coordinators, nursing and blood bank staff, obstetric anesthesiologists, obstetricians, vascular surgeons, urologists, neonatologists, and interventional radiologists. It cannot be overemphasized that prenatal diagnosis is an important factor in reducing maternal morbidity and mortality. Planning for delivery in a tertiary care center with experience in management of PAS based on an interdisciplinary approach is of utmost importance in this complex patient population. In our institution, as soon as the diagnosis is made, the team is activated, and preoperative planning begins and preterm cesarean hysterectomy is scheduled. 3 The blood bank is notified, ABO, Rh antibody status are analyzed, orders are placed, and supplies checked. The physicians communicate to ensure all pertinent tests and procedures are performed to optimize the patient before surgery. Special attention is given to underlying coagulopathy and anemia. Statistically significant reductions in blood loss have been reported when a multidisciplinary approach is implemented.4–7 On the contrary, it is recommended that PAS patients be managed in tertiary care centers, underscoring the importance of resource availability and coordinated multispecialty care. 8 Surgical management of PAS entails multiple interventions aimed at limiting bleeding. The use of prophylactic hypogastric balloons is controversial, as it does not account for all the proximal uterine blood supply; and some authors have shown their inefficacy in cases of placenta percreta. 9 Other strategies such as compression of the abdominal aorta may be indicated in a severe case like the one presented here. 10 Although surgical management in this case may have included or omitted different strategies with controversial or demonstrated efficacy, we focused our case on resuscitation of a patient with massive bleeding in the context of PAS.
Our patient with PAS had a favorable outcome. Her survival depended on multiple factors related to medical and surgical management, in the context of the resources available at a tertiary care center and a coordinated interdisciplinary approach. To our knowledge, there is a scarcity of reports of massive transfusion in the order of 250 units of blood products in both general surgical patients and in the obstetric setting. Transfusion of blood products was initiated early in the case. Activation of multiple transfusion protocols is recommended early in peripartum hemorrhage, as it is associated with reduced mortality. 11 We employed a ratio of red blood cells to plasma to platelets of approximately 1:1:1. Although studies have not yet been conducted in obstetrics to demonstrate the superiority of the 1:1:1 ratio, this ratio has been recommended in studies of trauma patients, and those results have been extrapolated to postpartum hemorrhage. 12 Under our patient’s surgical circumstances, we had expected a major compromise of perfusion to the lower extremity that may have led to limb amputation. Studies in trauma patients have reported up to 47% amputation rate after common iliac artery ligation. 13 In our case, Doppler signals returned and the patient preserved limb function. Animal studies suggest that in young individuals, arteriogenesis and large-vessel neoformation occur after acute limb ischemia. 14 We may argue that these compensatory mechanisms in addition to collateral blood flow helped preserve long-term lower extremity function.
Although rupture of utero-ovarian vessels played a role in the significant blood loss of our patient, 15 our case underscores the importance of an effective resuscitation led by the anesthesiologist. Successful resuscitation in complex cases encompasses preoperative planning, intraoperative invasive and noninvasive monitoring, early detection of physiologic changes, and aggressive intervention by a team led by an anesthesiologist. Along this spectrum of clinical course, communication with the surgical and ancillary teams is critical. Regarding preoperative planning, the anesthesiologist is called to lead an interdisciplinary effort to anticipate intraoperative events and proactive courses of action. 16 Large bore vascular access, invasive monitoring, cell saver setup and rapid infusion systems must be planned and be in place before neuraxial blocks or induction of general anesthesia.17,18 The choice of anesthetic technique must be based on risk stratification, and should take into account the patient’s wishes, safety issues, and resuscitation plan. 19 Communication between obstetricians and anesthesiologists is necessary to determine the order and dose of uterotonic agents. The decision to activate multiple transfusion protocols should be made by the anesthesiologist based on estimated blood loss and hemodynamic, metabolic, and hematological variables. The activation of transfusion protocols must be announced to all personnel in the operating room. The use of tranexamic acid and point-of-care coagulation testing is recommended in these complex cases.20,21 Finally, postoperative destination to critical care and pain management should be planned by the anesthesiologist. 22
The glycocalix plays a critical role in vascular hemostasis and permeability as well as cell adhesion. 23 It has been postulated that hemorrhagic shock is associated with endothelial glycocalix shedding and degradation in animal models. 24 The amphoteric nature of endogenous albumin promotes binding of glycocalix and contributes to the preservation of normal capillary barrier function. 25 In addition to determine vascular oncotic pressure, albumin is a scavenger of reactive oxygen species and possesses anti-inflammatory and immunomodulatory properties.25,26 Colloids have been shown to increase plasma volume and cardiac index with smaller volume compared to crystalloids. This is important because excess volume leads to insterstitial edema and worsening of tissue oxygenation. 27 On the contrary, albumin is able to expand plasma volume without effect on vascular leak in patients undergoing major abdominal surgery. 28 In our case, we used colloid as the primary resuscitation fluid in addition to blood products. The acid–base status and creatinine levels were normal after the procedure despite the significant blood loss. We consider that being able to limit migration of fluid to the interstitial space via preservation of glycocalix may have contributed to the favorable outcome of our patient. Future research is necessary to determine the role of albumin as the primary fluid in management of severe obstetric hemorrhage.
Conclusion
We present a case of complex placenta accrete spectrum with severe intraoperative hemorrhage requiring complex interdisciplinary surgical management and massive transfusion of blood products with favorable outcome in terms of patient survival and lower extremity preservation. Our case demonstrates the importance of early mobilization of a multidisciplinary effort and resource availability for the management of patients affected by PAS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.