
Abstract
We present a 59-year-old female Jehovah’s Witness patient transferred from another facility to our tertiary center as an emergency case owing to anemia due to gastrointestinal bleeding. A computed tomography scan and gastroscopy confirmed an invasion of the duodenum by a malignant process. The patient underwent a Whipple procedure and a right hemicolectomy refusing blood transfusion. On the 17th postoperative day, the patient was discharged following a successful surgery. This article’s objectives are to first highlight the moral and ethical quandary and then share our surgical experiences with this particular patient population. In conclusion, Jehovah’s Witnesses’ management of major abdominal surgery poses considerable clinical, moral, and legal difficulties. Despite them, doctors must put the patients’ needs first while also honoring their religious convictions. However, urgent situations continue to arise, forcing medical professionals to weigh their religious convictions against the need to save a patient’s life.
Introduction
Jehovah’s Witnesses is a religious group that stands out for its distinctive ideals and practices, particularly its opposition to blood and blood-related products’ transfusions. In low- and middle-income countries, providing medical care for Jehovah’s Witness patients who require major urgent abdominal surgeries can be even more challenging due to limited resources, inadequate healthcare infrastructure, and cultural and religious factors that can influence healthcare decisions. 1 Furthermore, if the patient presents with severe anemia, this can further complicate the situation, as surgery may be necessary to address the underlying condition causing the anemia, but this can also increase the risk of significant blood loss during the procedure.1,2
In these challenging circumstances, healthcare providers must navigate the tension between respecting the patient’s religious beliefs and ensuring the highest standard of medical care. This requires a multidisciplinary approach involving the patient, their family, and the healthcare team to arrive at a shared decision-making process that considers the patient’s health, religious beliefs, and cultural background. 3 In this essay, we will explore the challenges and opportunities presented by caring for Jehovah’s Witness patients undergoing major urgent abdominal surgeries with life- threatening anemia in middle-income countries.
Case description
A female patient, 59-year-old and a Jehovah’s Witness, was admitted to the secondary hospital in a small city due to abdominal pain. Primary laboratory investigations reveal a hemoglobin level of 64 g/L. Immediately, she was transferred to the main tertiary university clinical center “Mother Theresa” in the capital city of Skopje as an emergency case with suspected gastrointestinal tract issues. She underwent diagnostic procedures. Gastroscopy revealed gastrointestinal tract bleeding from suprapapillary formation with a central ulceration on the back-lateral wall of the duodenum, and a computed tomography (CT) scan confirmed a neoplastic infiltrative process of the colonic hepatic flexure carcinoma into the descending part of the duodenum (Figure 1). It was obvious she needed urgent life-saving surgery. High-risk consent as well as transfusion of blood and blood-related products’, including cryoprecipitate, refusing consent was obtained due to her severe condition because of her
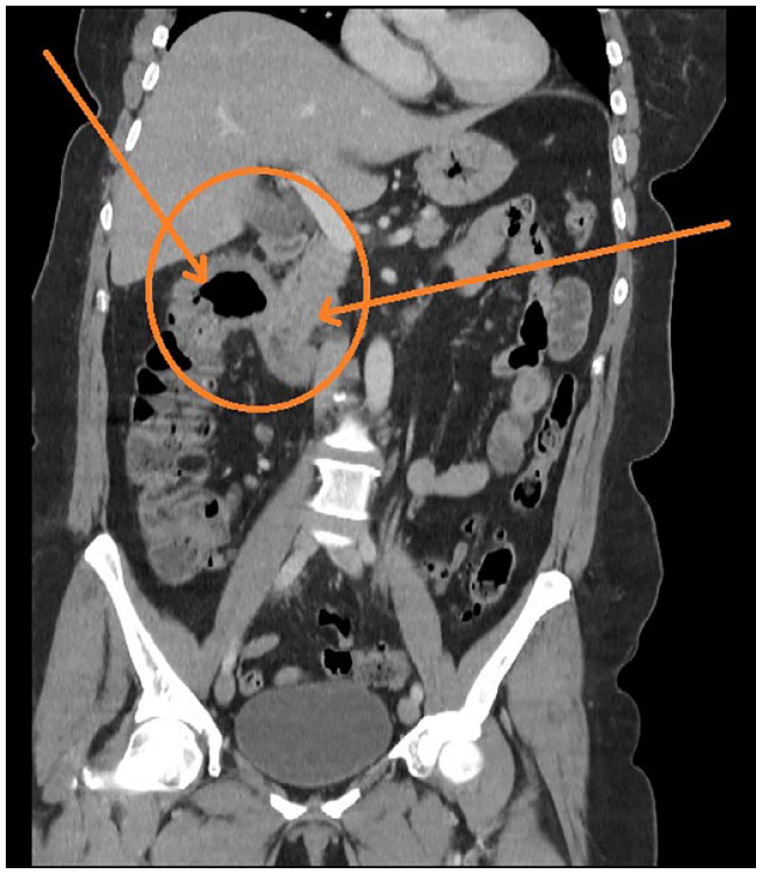
CT scan of the abdominal tumor before surgery showing tumor infiltration of the colonic hepatic flexure carcinoma into the descending part of the duodenum.
The patient was hemodynamically stable for the whole procedure. Blood gas analysis after finishing the anastomosis revealed Hb of 59 g/L. Despite the complexity of the case involving medical and ethical concerns as well, the surgery was performed successfully by the on duty surgical and anesthesia teams no needing extra personal and lasted 4 h with an estimated blood loss of 450 ml at the end of the surgery. The patient was sent to a tertiary medical center as an emergent case because of acute severe gastrointestinal bleeding where no time for preoperative measures for optimizing the patient could be met as seen in other patients needing elective surgery. Because of the emergent nature of the case as well as the verified malignant process, the intraoperative use of a cell salvage technique and extracorporeal membrane oxygenation (ECMO) were not possible neither available. During her hospital stay, she was continuously treated with iron, sucrose, erythropoietin, and vitamins. On the 12th postoperative day, thoracocentesis with evacuation of 800 ml of transudate was performed. Because of the patient’s beliefs as well as the beliefs of the patient’s family which has refused transfusion of blood and any type of blood products during the treatment despite the seriousness of the condition and possible complications, we have treated the patient respecting her decision, so neither blood nor blood products were not given during the whole in-hospital stay. The patient was discharged from the hospital on the 17th postoperative day with Hb levels of 86 g/l. During the in-hospital stay, she received the total amount of 12,000 of erythropoietin applied subcutaneously as well as the total amount of 1700 mg of iron for parenteral application.
Discussion
A number of studies have been conducted concerning the medical and legal difficulties that doctors who treat Jehovah’s Witnesses face,4,5 and there have been stories of successful blood-saving procedures used during abdominal surgery.6–8 However, to our knowledge, this is the first emergency case of the Whipple procedure in a Jehovah’s Witness with grade 4 (life-threatening anemia) and a hemoglobin value of 65 g/L.
When Jehovah’s Witnesses reject blood transfusions, a variety of intricate ethical dilemmas involving the four fundamental principles of ethics, such as beneficence, non-maleficence, autonomy, and justice, are at hand. Even if the clinician believes that the patient made an irrational decision or that the decision may inevitably result in the patient’s death, which can be very difficult for a doctor to accept, the principle of autonomy should be respected in patients who can provide informed consent and do not wish to receive blood products.9,10
However, the act of withholding blood products (even though it is an act of omission in this case) can lead to internal conflict for doctors because the principle of non-maleficence requires that they prevent injury for their patients. The principle of beneficence supports the doctor in providing the patient with the best care possible, which in some situations may involve the transfusion of blood products. When managing this kind of patient, effective communication with the patient and their family is also crucial in these situations to ensure that the patient’s religious beliefs and cultural values are respected while providing appropriate medical care.11,12 Regarding this fact listed before, we as a medical team did a detailed briefing with the patient and the closest family members explaining them the deep seriousness of the condition of the treatment options and a live-saving need of a surgery as well as the complications that may arise without receiving blood and any blood products during the perioperative period. The fourth and final principle of justice advocates for respecting a competent patient’s wishes. Therefore, in this situation, withholding blood products is acceptable, 13 which was done in our case. To ensure a thorough grasp of the diagnosis, prognosis, surgical challenges, and potential issues, we conducted extensive preoperative discussions with the responsible anesthetist, surgeon, medical staff, and all of our patient relatives and patients themselves. After confirming that our patient is completely aware of the possible complications arising from the procedure as well as her beliefs for not receiving any blood products after signing the high-risk consent and transfusion refusing consent, we have proceeded to the surgical treatment not hurting her autonomy or justice, which were discussed before. It is very true that in this kind of situations when following the patients’ beliefs, there is a high possibility of hurting the second and third principles of ethics because of practicing medicine in emergent cases against all well-known principles for maintaining homeostasis in order to keep the patient wish a priority.
When treating Jehovah’s Witnesses, alternative strategies to manage the patient’s anemia and prevent further complications may be necessary. This may involve the use of blood conservation techniques, such as preoperative optimization of the patient’s hemoglobin levels, intraoperative blood salvage and reinfusion, and the use of erythropoietin-stimulating agents to promote red blood cell production. 13 While some patients will consent to these methods, others will not. Despite the possible risk of retransfusing cancerous cells, the majority of patients were glad to take blood that had been saved from cancer cells. 14 However, recent research suggests that cell salvage does not raise the risk of cancer recurrence, which may persuade patients to adopt this blood management method after surgery.15,16 Lee and colleagues used transfusion-free pancreatectomies. Most of the transfusion-free pancreatectomy patients in their program got treatment based on three pillars. First, patients underwent preoperative blood augmentation, receiving IV iron, sucrose, and erythropoietin until their hemoglobin level exceeded 12.0 g/dl. Second, the majority of patients underwent autologous blood conservation. The anesthesiologist decided whether to do it, and the amount of autologous transfusion was determined based on the patient’s basic information (expected blood loss, preoperative hemoglobin concentration, and overall physiologic status as measured by heart rate, blood pressure, and central venous pressure), as well as their risk of bleeding and general health. Third, a transfusion-free approach designed to reduce postoperative blood loss. 17 However, this was an emergency case with life-threatening anemia, and unfortunately, perioperative methods in limited resource centers are restricted due to human or technical resources. We do not have technicians on call for intraoperative cell salvage. Due to the urgency of the case, we did not have any possibilities for preoperative blood conservation techniques as well.
On the other hand, the products that Jehovah’s Witnesses consider unacceptable vary, so it is important to determine whether a product is acceptable before taking any action. 4 Recombinant erythropoietin, recombinant factor VIIa, and synthetic blood substitutes are examples of products that are generally acceptable; however, platelet fractions, albumin, immunoglobulins, cryoprecipitate, interferons, and red cell fractions, including human hemoglobin, may also be acceptable. Artificial blood replacements, most frequently seen as hemoglobin-based oxygen carriers and perfluorocarbon-based oxygen carriers, imitate some of the biological functions of red blood cells, most notably those of oxygen and carbon dioxide. 18 But it is difficult to get these for clinical use. 13 As mentioned previously, we used recombinant erythropoietin in our case and albumin 20%–50 ml as well.
Guidelines that specify precautions to be taken to reduce risk among Jehovah’s Witnesses who undergo major surgery have also been published by the Royal College of Surgeons of England 18 and the Association of Anaesthetists of Great Britain and Ireland. 19 Anesthetic techniques include patient positioning (typically in the Trendelenburg position), temperature control to prevent hypothermia and subsequent coagulopathy in patients, and ventilation intended to reduce venous preload and, consequently, any potential increase in bleeding. All of those strategies, with protective ventilation and minimal positive end-expiratory pressure (PEEP), were used in our case. Controlled hypotension was used to minimize perioperative blood loss as well. Fernandes describes this strategy in their presented case of complex pancreatic resection with vascular involvement in Jehovah’s Witnesses. 20 Intraoperative surgical strategies include the use of electrosurgery and harmonic scalpel devices to help with meticulous hemostasis, direct compression to achieve hemostasis, the application of hemostatic agents like fibrin glues, gelatin-based sealants, and human fibrinogen packs, and the application of hemostatic agents. Electrosurgery and a harmonic scalpel were used for hemostasis in our presented case by our experienced surgical team.
The rationalization of postoperative phlebotomy, the use of pediatric tubes when possible, and rapid assessment by a senior clinician if acute blood loss is anticipated are strategies to reduce postoperative blood loss. Although there is conflicting evidence, several surgical specialties have postoperative wound drainage systems that enable the autotransfusion of drained blood, minimizing any loss.21,22 Hyperbaric and extracorporeal oxygen therapies are further treatments for patients who have suffered significant intraoperative blood loss, although these are not commonly used,23,24 and we did not use any in our presented case.
Before beginning the operation, we did a full briefing with the entire theater staff. The briefing covered the criteria for stopping the procedure in the event of intraoperative issues, as well as all operational tactics and any backup plans required for the safe conduct of the surgery. Postoperative tactics were clearly documented in the case notes, and a debriefing with the team was held at the conclusion of the operation. The patient’s wishes and the postoperative monitoring and treatment plan were made known to all individuals (including nursing and support staff) involved in the postoperative care of the patient.
Conclusion
The risks of catastrophic hemorrhage and eventual fatality are, nevertheless, a concern for the medical staff, despite the fact that Jehovah’s Witnesses can routinely endure major surgery without worry. This is made much more difficult in centers with inadequate resources in low- and middle-income nations. Adopting a comprehensive and collaborative multidisciplinary approach, involving surgeons, hematologists, anesthesiologists, transfusion specialists, as well as the active participation and support of the patient and their family, is crucial to effectively address the challenges of catastrophic hemorrhage and mortality in major surgeries among Jehovah’s Witnesses, emphasizing the importance of a coordinated effort within the medical community and a patient-centered approach.
Footnotes
Article’s note
This manuscript has not been published and is not under consideration for publication elsewhere.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from University Clinic for Anesthesia Reanimation and Intensive Care, Clinical Center Mother Theresa, Faculty of medicine, University “Ss. Cyril and Methodius” Skopje, R.N. Macedonia Approval number: 5.1. 2023/6.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Note
The patients in this study have signed formal releases granting permission for the publication of their case information.