
Abstract
Linear cutaneous lupus erythematosus is an unusual presentation of cutaneous lupus following Blaschko’s lines. It is described mostly in children and young adults and is usually not associated with systemic involvement. We report two cases of linear cutaneous lupus erythematosus in children who significantly improved after treatment with hydroxychloroquine in combination with topical corticosteroids and tacrolimus. These rare cases underline the importance of including linear cutaneous lupus erythematosus in the differential diagnosis of blaschkoid inflammatory lesions.
Introduction
In pediatrics, classification of cutaneous lupus erythematosus (CLE) is similar to adults, including acute CLE (ACLE), subacute CLE (SCLE), and chronic CLE (CCLE).1,2 Childhood-onset CLE may, however, differ in demographics and disease progression. Median age at diagnosis varies between 11.7 and 14 years, with a female predominance of about 2F:1M,1,2 except in pre-pubertal onset 1 and CCLE 2 where an equal sex distribution is observed. CCLE is most commonly reported (45%–60%), followed by ACLE (34%–35%).1,2
Less commonly known, linear CLE (LCLE) is a rare presentation of CLE following Blaschko’s lines. 3 This distinct subtype is described mostly in children and young adults. Herein, we report two rare cases of LCLE occurring during childhood.
Case report
Case 1
A 12-year-old girl presented to the Pediatric Dermatology Clinic for a 6-year history of asymptomatic linear plaques on her knee. She was not known for any diseases and didn’t take any medication. The patient had no systemic symptoms such as fever, weight loss, arthralgias, oral ulcers, photosensitivity, or cardiopulmonary symptoms. Atrophic, squamous, and erythemato-violaceous plaques following Blaschko’s lines were noted on her left knee (Figure 1). Antinuclear antibodies (ANA), extractable nuclear antigen (ENA) antibodies (full panel including anti-SSA, anti-SSB, anti-Sm, anti-RNP, anti-Scl-70, anti-Jo-1 and anti-CENP-B), and anti-double stranded DNA (anti-dsDNA) antibodies were negative. Laboratory tests such as complete blood count, creatinine, urinalysis, liver tests, and C-reactive protein were normal.

Linear cutaneous lupus erythematosus with erythemato-violaceous and squamous papules and plaques with some atrophy along medial left knee.
Skin biopsy revealed vacuolar interface dermatitis with superficial and deep lymphohistiocytic perivascular and periadnexal infiltrates, lymphocytic vasculitis and increased dermal mucin deposition (Figure 2). Direct immunofluorescence (DIF) was not done. Little response was noted under betamethasone dipropionate 0.05% cream. Hydroxychloroquine (5 mg/kg/day) combined with tacrolimus 0.1% ointment led to a significant improvement within 6 months.
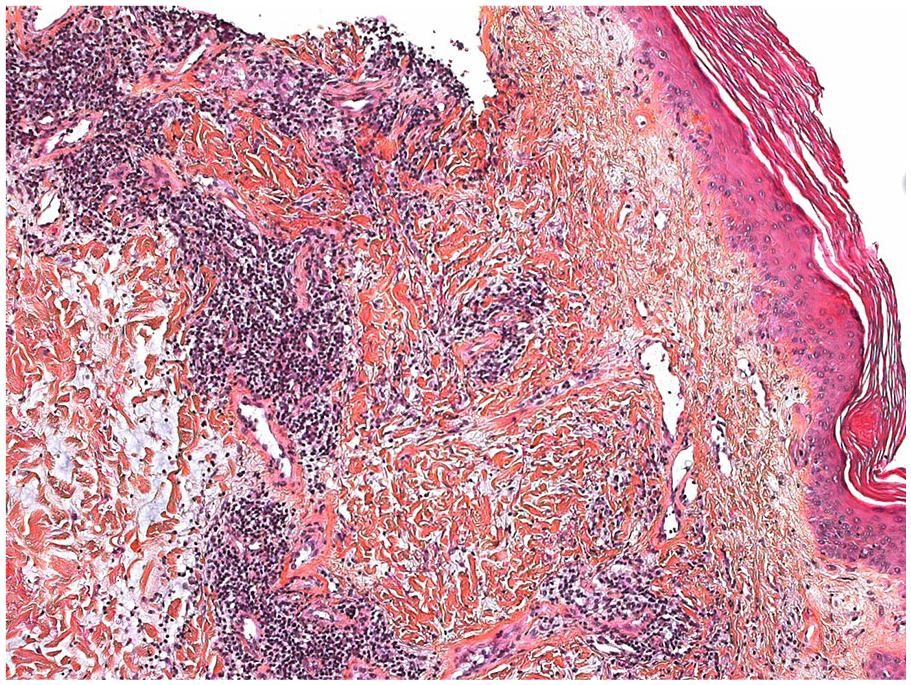
A hematoxylin eosin saffron–stained section at 100× magnification shows vacuolar interface dermatitis, lymphohistiocytic perivascular and periadnexal infiltrates and lymphocytic vasculitis. Collagen bundles are separated by a clear substance within deep dermis.
Case 2
A healthy 15-year-old boy presented a 3-year history of slightly pruriginous linear lesions on his thigh. There were no systemic symptoms, and a review of systems was negative. Blaschkoid squamous and erythemato-violaceous papules with follicular plugging were observed on his left anterior and medial thigh (Figure 3). ANA, ENA full panel and anti-dsDNA were negative, and the remaining laboratory investigations were normal. Skin biopsy showed findings similar to the first patient (Figure 4). DIF was not done. Complete resolution was noted within 5 months under hydroxychloroquine (5 mg/kg/day) with clobetasol propionate 0.05% cream (for 5 weeks), followed by tacrolimus 0.1% ointment.

Blaschkoid cutaneous lupus erythematosus: confluent squamous erythemato-violaceous papules with follicular plugging on left thigh.

A hematoxylin eosin saffron–stained section at 100× magnification shows vacuolar interface dermatitis, lymphohistiocytic perivascular and periadnexal infiltrates, and lymphocytic vasculitis.
Discussion
LCLE represents a rare subtype of CLE mostly described among children and young adults. 3 The term “linear” refers to its peculiar clinical presentation in which lesions follow Blaschko’s lines. The latter illustrate pathways of ectodermal development during embryogenesis and are subject to mosaicism, resulting in apparent distinction between genetically abnormal and normal skin. 4 With keratinocyte apoptosis known as a key event for initiating CLE, it is hypothesized that genetically altered keratinocytes in LCLE may involve apoptotic pathways, hence predisposing them to apoptosis induced by ultraviolet irradiation for example. 5
In a literature review, 35 cases of childhood-onset LCLE were identified, including our 2 cases (1978–2020, conducted through PubMed).3,6–35 Median age of onset was 9 years old (1–17 years old), with a female predominance of 3F:1M. Different subtypes of CLE with a blaschkoid pattern have been described: discoid CLE (12 cases), lupus panniculitis (11), SCLE (1), bullous systemic lupus erythematosus (SLE) (1) and non-specified (10). The head and neck area were most frequently involved (57%), followed by extremities (46%) and trunk (14%), including 6 patients with multiple sites. LCLE lesions were usually erythematous and/or violaceous and may be atrophic (46%) and/or squamous (40%). Among patients with lupus panniculitis, 5 presented linear alopecia.8,22,27,28,30 Follicular plugging was noted in four cases (our case and previous studies),14,29,35 sclerosis in three13,19,35 and milia in one. 25 Patients were mostly asymptomatic but pruritis was occasionally noted.
The presence of SLE in LCLE is rare with only 2 patients reported.15,31 The first patient had linear bullous SLE and suffered from fever, palpebral edema, malar rash, oral ulcers and arthritis. 31 She had leucopenia and nephritis with positive ANA (1:1024), anti-dsDNA, anti-Ro and low complements (C3, C4). She responded well to systemic corticosteroids, hydroxychloroquine, and dapsone. The second patient had lupus panniculitis with fever, photosensitivity, oral ulcers, interstitial pneumonia, cytopenia and proteinuria. 15 She had positive ANA (1:320), anti-Ro and anticoagulant autoantibodies (anti-dsDNA not disclosed). Complete remission was noted within 5 months of systemic corticosteroids and azathioprine. Four patients had isolated photosensitivity.3,9,11,19
Among pediatric LCLE cases, the diagnosis was always confirmed by cutaneous biopsy. DIF positivity rate was 56% and showed linear and/or granular deposition of IgM +/- IgG, IgA and C3 deposition along dermoepidermal junction.3,6,8,18,20,23,31,33–35 ANA, anti-SSA/Ro and anti-dsDNA were positive in 33%3,6–8,11,15,17,18,26,27,31 (18% if ⩾1:160), 15%,15,16,31 and 6% 31 of cases, respectively. Full ENA panel was done in 8 cases (including our 2 patients), whereas other cases only disclosed about anti-SSA/Ro (mostly), anti-SSB/La, anti-Sm and/or anti-RNP. One patient had anti-histone autoantibodies without drug involvement. 13 The only patient with anti-dsDNA autoantibodies had bullous SLE. 31 Isolated leucopenia and isolated low complements were reported once.3,8
Multiple treatments have been described with pediatric LCLE (Table 1).3,6–17,19–35 Remission rates were of 25% and 73% with topical treatments and systemic treatments (in monotherapy or combination), respectively. Among the latter group, 6 patients initially failed to respond to topical treatments. Systemic treatments were often in combination and included corticosteroids, antimalarials and dapsone with remission rates of 100%, 63% and 100%. Time to remission was not often specified, but a period of 3 to 5 months was described in children under systemic treatments. It is difficult to draw conclusions about LCLE treatments due to various therapies and disease severity in reported cases, but topical treatments seem generally insufficient requiring systemic treatments.
Treatments reported in the 35 pediatric cases of linear cutaneous lupus erythematosus.

AZA: azathioprine; MMF: mycophenolate mofetil; MTX: methotrexate; TCI: topical calcineurin inhibitors; SLE: systemic lupus erythematosus.
Represents the same patient.
Represents the same patient.
Patient with SLE.
LCLE was diagnosed in our 2 patients considering blaschkoid distribution of lesions and cutaneous biopsy’s results. Both improved significantly with a combination of hydroxychloroquine and topical corticosteroids or tacrolimus. Interestingly, our first patient didn’t respond to topical potent corticosteroids in monotherapy, as reported in some cases in the literature. In conclusion, LCLE is a rare presentation of CLE with mostly good prognosis which should be considered in children with Blaschko-linear squamous erythemato-violaceous lesions and may require systemic treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patients provided written consent for publication of the case report.