
Abstract
Mycobacterium chelonae is a species of mycobacteria that can be found ubiquitously in the environment. It can be found in soil, water, and in aquatic animals. Infections with this pathogen usually involve the soft tissues, eyes, bones, and skin. We present the case of a recurrence of a sporotrichoid cutaneous infection by M. chelonae in an immunocompromised 31-year-old woman with systemic lupus erythematosus. The patient originally developed a swelling of her right foot followed by a sporotrichoid pattern of infection on her right lower leg. A susceptibility profile was established, and treatment with linezolid and clarithromycin was administered for 8 months, in accordance with guidelines from the American Thoracic Society. The patient was clear of new lesions for approximately 1 month before noting a re-emergence. Treatment with linezolid and clarithromycin was re-initiated with subsequent improvement. This case underlines the need for prolonged treatment of this infection in patients with an immunocompromised status.
Introduction
Mycobacterium chelonae, a non-tuberculous mycobacteria (NTM), is a ubiquitous species of mycobacteria that is found in the environment. It can be found in soil, dust, water and aquatic animals.1,2 Infections with this pathogen usually involve the soft tissues, eyes, bones, and skin. 3
We describe a case of cutaneous infection by M. chelonae presenting with a sporotrichoid pattern of lesions in an immunosuppressed patient. Our case underscores the importance of treating these cases with an extended course of appropriate antibiotics.
Case report
In July 2016, the patient, a 31-year-old female with a history of systemic lupus erythematosus diagnosed at 9 years of age, developed a swelling of her right foot. This was followed by a pattern of sub-cutaneous nodules spreading up her right lower leg.
At the time, she was taking methylprednisolone (12–16 mg DIE), hydroxychloroquine, cinacalcet, darbepoetin alfa, iron, and vitamin D. She had also been undergoing dialysis treatments for the past 10 years.
Despite many hospital visits, her cutaneous condition was not recognized multiple times over a 6-month period until a skin biopsy in February 2017 was performed. The biopsy revealed multiple areas of necrosis and suppurative granulomatous inflammation implicating the dermis. A modified Ziehl–Neelsen stain revealed rod-shaped microorganisms, around 2–5 mm in length, compatible with atypical mycobacteria. The mycobacteria were grown in culture and M. chelonae was then identified by the Laboratoire de Santé Publique du Québec using analysis of genomic deletions and by sequencing of the 16S rRNA gene. The patient presents multiple risk factors for acquiring this pathogen such as gardening and home pedicures. It is therefore difficult to determine an exact origin of infection.
Once M. chelonae was identified, a susceptibility profile was established showing susceptibility to amikacin, clarithromycin, linezolid, and tobramycin, and resistance to cefoxitin, ciprofloxacin, doxycycline, moxifloxacin, and trimethoprim/sulfamethoxazole. The patient was treated with a combination of linezolid and clarithromycin for 8 months: the lesions receded and antibiotics were discontinued in October 2017. The patient was clear of new lesions for approximately 1 month before noting a re-emergence of erythematous lesions on her right lower leg. A second skin biopsy was performed in December 2017 (Figure 1). This biopsy showed suppurative and necrotizing granulomatous inflammation in the dermis and hypodermis.
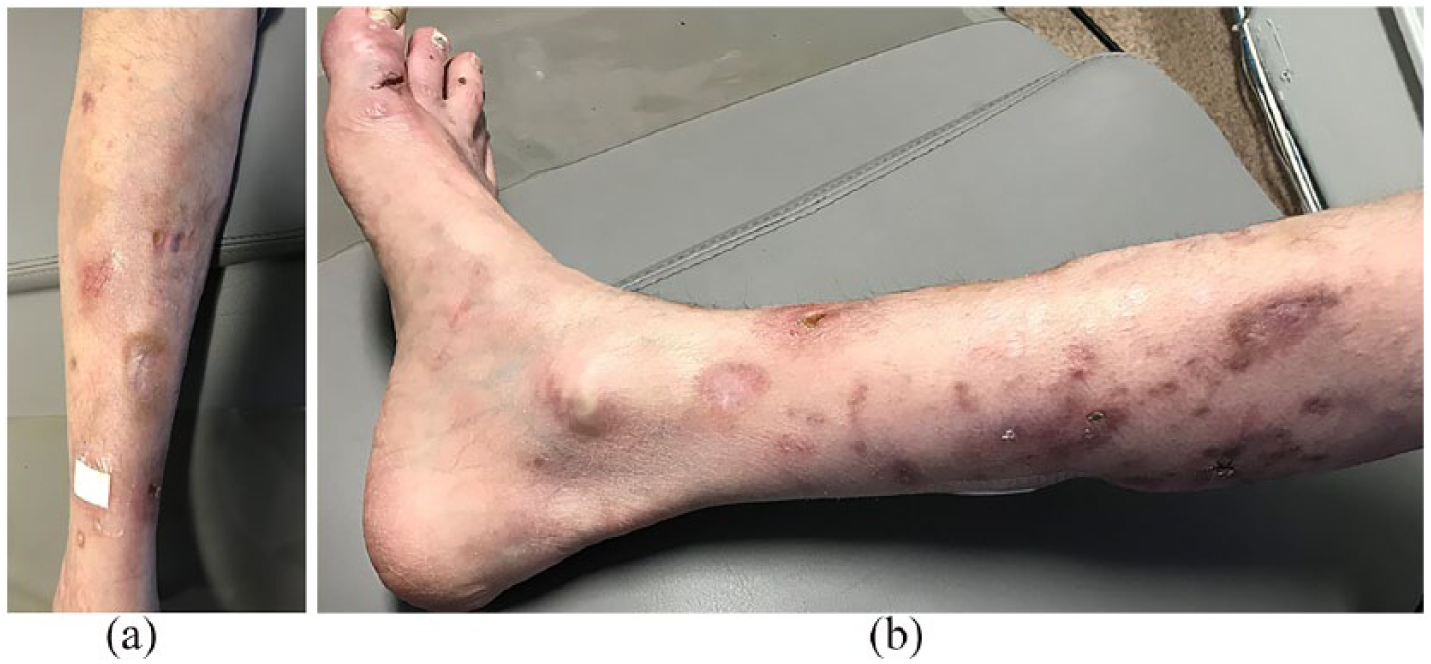
21 December 2017: unilateral sporotrichoid pattern of non-tender infiltrated plaques of the right foot and lower leg, on a background of chronic atrophic and hyperpigmented scarring—(a) frontal view and (b) medial view.
Modified Ziehl–Neelsen staining was once again performed, and this revealed the presence of rod-shaped microorganisms compatible with atypical mycobacteria (Figure 2). Treatment with linezolid and clarithromycin re-initiated with subsequent improvement was still underway as of March 2018.
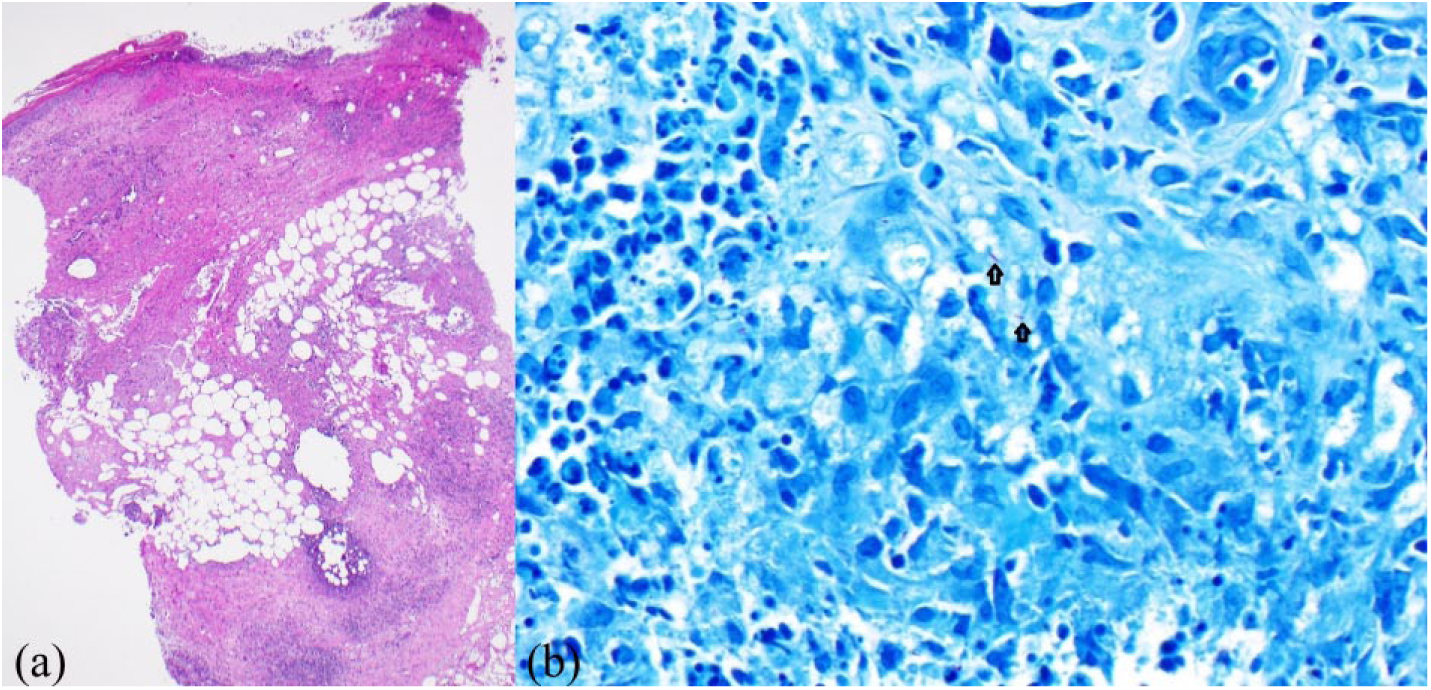
Biopsy of a nodule on the right lower limb. (a) Hematoxylin–eosin stain (40× magnification) demonstrated skin ulceration, extensive necrosis, and a suppurative granulomatous inflammatory process involving the dermis and the hypodermis, associated with fibrous reorganization. (b) Modified Ziehl–Neelsen stain (600× magnification) revealed rare rod-shaped organisms (black arrows) dispersed among areas of suppurative granulomatous inflammation.
Discussion
Skin, bone, and soft tissue disease are the most frequent clinical manifestations of M. chelonae infection. 3 The manifestations of cutaneous infection by M. chelonae vary mainly according to the patient’s immune status: localized infections such as cellulitis and abscesses are common in immunocompetent patients, whereas skin disease in the form of a sporotrichoid pattern of spread occurs most frequently in immunocompromised patients and is a rare form of presentation.1,4
The treatment parameters for this type of infection have not yet been standardized. Guidelines published by the American Thoracic Society on non-tuberculous mycobacterial diseases in 2007 recommend a minimum of 4 to 6 months of treatment with combination antibiotic therapy for cutaneous infection by M. chelonae but do not differentiate between treatment for immunocompetent and immunocompromised patients. 5
The only clinical trial for M. chelonae skin disease that we documented studied the use of clarithromycin monotherapy in 14 patients (500-mg BID for 6 months). 6 During the trial, infections resolved in all but one case in which there was a relapse with an isolate manifesting resistance to clarithromycin. Also, this patient had stopped treatment early (after only 3.5 months). 6 Due to the possibility of the development of mutational resistance to clarithromycin, monotherapy alone is not recommended.6,7 Moreover, treatment should always include clarithromycin as initial isolates of M. chelonae has shown 100% sensitivity to this antibiotic.8,9
In a review of the literature (1987–2017, conducted through PubMed), we identified 142,3,10–22 cases of cutaneous M. chelonae infection presenting with a sporotrichoid pattern of spread. The vast majority of these cases (80%; 11/14) occurred in immunocompromised patients. Half of the cases were treated with oral antibiotics for at least 4 months (7/14) and 40% for more than 6 months (6/14). Only one recurrence of infection was clearly identified, and it occurred after surgical debridement after approximately two and a half months of antibiotic treatment (30 days IV and 6 weeks PO). 11 No recurrences were noted in the cases treated for over 6 months.
This case highlights the importance of following patients and treating these types of cases, M. chelonae infection, with an extended course of appropriate antibiotics, in particular, in immunocompromised individuals. Further, there is clearly a need for additional research to determine treatment guidelines for M. chelonae cutaneous infections.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent for patient information and images to be published was obtained.