
Abstract
Entomophthoramycosis, a rare fungal infection, can mimic various clinical entities. We present a case of entomophthoramycosis affecting a 3-year-old male masquerading as liver tumour, diagnosed on stereotactic biopsy and later on resected specimen. He improved following partial hepatectomy and antifungal therapy. A high index of suspicion and heightened awareness regarding its unique morphological characteristics are required for appropriate management.
Introduction
Entomophthoramycosis includes mainly two genera basidiobolomycosis and conidiobolomycosis commonly affecting immunocompetent hosts. 1 They are ubiquitously found in tropical and subtropical regions like equatorial Africa, Central America and India. 2 It presents as loco-regional: subcutaneous and rhino-facial and/or systemic disease. Systemic dissemination is extremely uncommon; however, widespread fatal disease in visceral organs like brain, lung, spleen, stomach, kidney and pancreas was described. 3 Owing to its rarity, it is usually misdiagnosed as neoplasms like lymphoma, rhabdomyosarcoma, gastrointestinal stromal tumor or chronic granulomatous infections like tuberculosis, schistosomiasis and Crohn’s disease resulting in delay in management.1,4 Treatment includes rapid institution of appropriate antifungals with surgical resection when appropriate.
We herein report an unusual presentation of entomophthoramycosis as liver mass. It is an alert to clinicians to consider etiologies beyond the hepatic tumours and bacterial infections in children presenting with liver mass.
Case report
A 3-year-old male presented with persistent high-grade fever for 5–6 months, and upper abdominal distension with epigastric pain for 2 months. Physical examination revealed pallor and bilateral firm, mobile, upper cervical lymphadenopathy (1 cm × 1 cm). On systemic examination, there was a non-tender, firm hepatomegaly, with the left lobe of liver extending 10 cm below the xiphisternum. Ultrasonography (USG) revealed a lobulated necrotizing, echogenic mass (7.8 cm × 6.2 cm × 4.9 cm) in the left lobe along with a small echogenic lesion (7 mm) in segment IVa. A possibility of hepatoblastoma was entertained. On investigations, the haemoglobin was 7.0 g/dL; total leukocyte count was 29.2 × 109/L with 37% neutrophils, 30% eosinophils (absolute eosinophil count: 8760/mm3) and a platelet count of 900 × 109/L. The total serum protein was 9.2 g/dL with reversal of albumin/globulin ratio (albumin 4.2 g/dL and globulin 5.0 g/dL). The bilirubin, liver enzymes, alkaline phosphatase and renal functions were normal. Serum alpha-fetoprotein and beta-hCG levels were normal for age. The chest X-ray was normal. Contrast-enhanced computed tomography (CT) scan of the abdomen revealed a 7.3 cm × 5.8 cm × 4.7 cm lesion involving segments II, III and IVa with large central area of necrosis and contiguous extension into the greater omentum with evidence of mild ascites. No fat/calcifications/hypervascularity/centripetal enhancement was noted. Left portal vein was obliterated proximally and not visualized in the distal part with the left hepatic vein being obliterated also. The remaining hepatic and portal vessels were normal. No retroperitoneal lymphadenopathy was noted (Figure 1(a) and (b)). CT chest was normal.
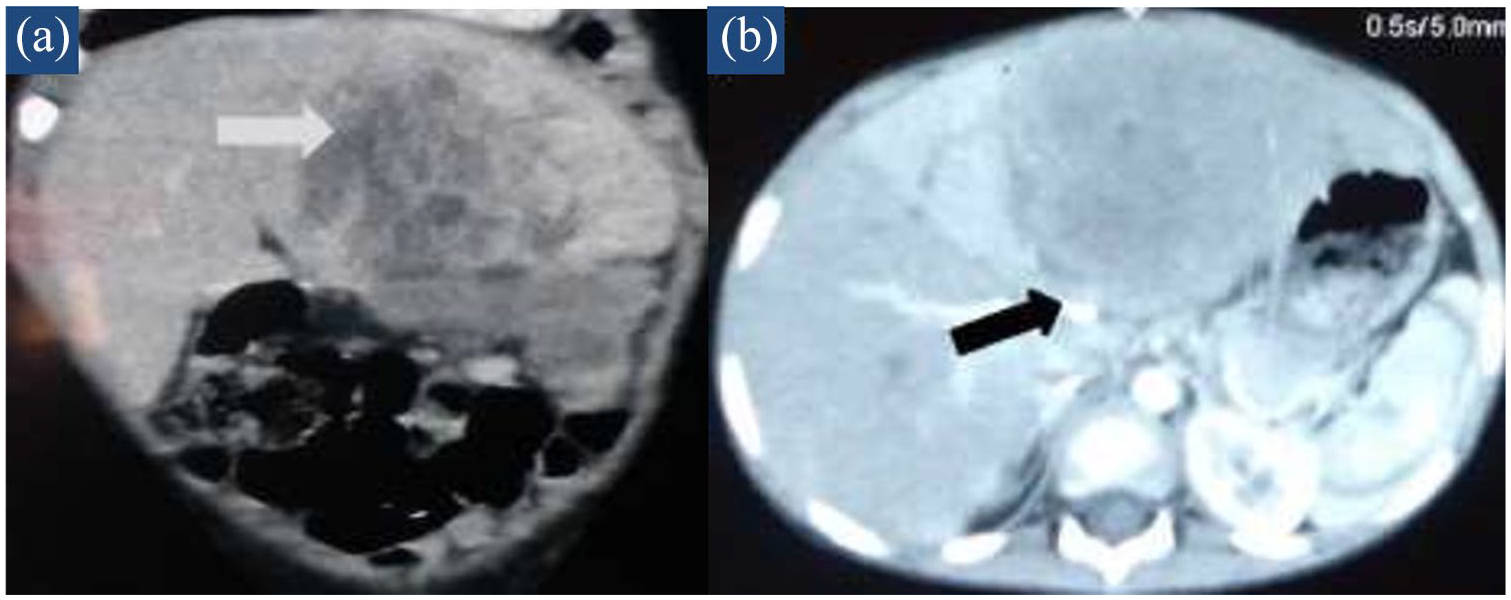
(a) Coronal view of CECT abdomen showing a 7.3 cm × 5.8 cm × 4.7 cm lesion involving segments II, III and IVa with large central area of necrosis and contiguous extension into greater omentum. (b) Axial view: obliteration of left portal vein (proximal; distal not visualized) and left hepatic vein.
Course and management
USG-guided tru-cut needle biopsy done from the mass was consistent with a diagnosis of entomophthoramycosis of liver. Fungal culture was negative. Paraffin sections subjected to real-time polymerase chain reaction (PCR) and direct DNA sequencing of internal transcribed spacer (ITS) regions of ribosomal DNA utilizing panfungal ITS primers were negative.
He was started on oral itraconazole at a dose of 5 mg/kg BD and was evaluated for an underlying immunodeficiency. HIV serology was negative. Immunoglobulin profile, lymphocyte subsets and Nitrobluetetrazolium (NBT) assay were normal. He underwent a left hepatectomy. Fever defervesced after surgery. An USG abdomen done 2 months later did not show any residual lesion. He received itraconazole for 8 months and tolerated the drug without any adverse effects. His liver function tests were initially monitored twice a week for a month and then monthly while on itraconazole. The liver functions remained normal throughout therapy. At 12 months of follow-up, he was doing well.
Histopathology
Tru-cut needle biopsy revealed extensive areas of necrotizing inflammation with occasional epithelioid granulomas (Suppurative granulomas). Many broad, thin walled, aseptated fungal hyphae exhibiting classic Splendore–Hoeppli phenomenon were noted within the granulomas and few were phagocytosed within the giant cells. The morphology of fungal hyphae was consistent with entomophthoramycosis. The resected specimen of liver measured 15 cm × 13 cm × 7 cm. The cut surface on gross examination revealed multi-nodular exophytic mass with focal areas of necrosis measuring 7 cm × 6 cm × 5.5 cm mimicking hepatoblastoma. The adjoining liver parenchyma was essentially normal (Figure 2(a)).

(a) Gross slice of liver showing greyish white nodules with focal necrosis. (b) Areas of geographic necrosis in the liver (H&E 40×). (c) Interface region showed histiocytes, foreign body type giant cells (H&E 200×). (d) Giant cells containing multiple fungal profiles (H&E 400×).
Microscopically, multiple large areas of geographic necrosis bordered by multiple foreign body giant cell granulomas composed of plump epithelioid cells, histiocytes, eosinophils, and lymphomononuclear cells (Figure 2(b) and (c)). Additionally, many suppurative granulomas were seen within which multiple short and broad pauci-septated hyphae bordered by eosinophilic granular material (Splendore–Hoeppli phenomenon) were noted (Figure 2(d)). The characteristic obtuse-angle branching of fungal hyphae was highlighted by Periodic acid Schiff (PAS) and Grocott’s silver methanamine stains (Figure 3(a)–(d)).

(a and b) Broad pauci-septate fungal hyphae surrounded by eosinophilic granular material (Splendore–Hoeppli phenomenon) (H&E 400×). (c) PAS stain (arrow) highlights the fungal profile (400×). (d) Grocott’s stain (arrow) highlights the fungal profile (400×).
Discussion
Entomophthoramycosis occurs predominantly in children and usually follows a trivial trauma or insect bites to the skin or has a transepidermal route secondary to contaminated vegetable matter. The organism gets inoculated into subcutaneous planes and often disseminates. 5 The loco-regional disease has a predilection for areas with adipose tissue like thighs, buttocks and trunk. It presents as two forms such as subcutaneous zygomycosis (basiodiobolomycosis) and rhino-facial zygomycosis (conidiobolomycosis). Systemic forms may affect any visceral organ like lungs, liver and gastrointestinal (GI) system.5,6
The initial diagnostic investigation for a case of abdominal lump is imaging. In a suspected entomophthoramycosis, USG might help in identifying GI wall thickening, tumour-like intra-abdominal mass lesions and rarely kidney or liver lesions. There are no described diagnostic radiological features of entomophthoramycosis. However, CT/magnetic resonance imaging (MRI) scans will aid in determining the exact location and delineating the extent of the disease. A diagnosis can be confirmed only by histopathology, culture or molecular typing. 7
Our case is a systemic form of entomophthoramycosis with a speculative origin in the GI system and subsequent spread to the liver causing a tumefactive lesion. Classical cases of GI basidiobolomycosis usually present with abdominal pain, mass, fever, vomiting, diarrhoea, constipation, bloody mucus discharge and weight loss. The initial working diagnosis with such a presentation is invariably a neoplasm which includes a lymphoma, rhabdomyosarcoma, GI stromal tumours or chronic granulomatous infections like tuberculosis, schistosomiasis and Crohn’s disease. 4 A similar type of tumefactive presentation of basidiobolomycosis in the descending colon and liver was described in a 61-year-old man. Silva et al. 8 described entomophthoramycosis presenting as a tumefactive liver lesion where the patient, though treated with amphotericin B, succumbed to the illness. In a large autopsy series on visceral mycosis, systemic form of entomophthoramycosis was noted in only one out of 610 cases. 9 In a review of 44 cases of GI basiodiobolomycosis which includes both children and adults, liver/gall bladder involvement was seen in 30% of cases, intra-abdominal malignancy being the provisional diagnosis in 43% of cases. The common clinical manifestations were abdominal pain (84%), abdominal mass (43%) and eosinophilia (76%). 10
The diagnosis of entomophthoramycosis requires a high index of suspicion by the clinician and histopathologist. Histological examination and mycological culture are the gold standard for confirmation of diagnosis. 1 However, in the absence of supportive culture and molecular techniques, sole histological diagnosis of entomophthoramycosis can be made with context. Subtle histological clues include short and broad septated hyphae with right or wide angle branching in a suppurative granulomatous inflammation, Splendore–Hoeppli phenomenon and relative lack of angio-invasion. Splendore–Hoeppli phenomenon is a result of antigen–antibody precipitate to the organism’s antigens; however, it is not specific and is also observed in other mycotic infections (Sporotrichosis, Pityrosporum folliculitis, Candidiasis, Aspergillosis and Blastomycosis), bacterial infections (Nocardiosis and Actinomycosis), Pythium insidiosum, Lagenidium giganteum, Paralagenidium species and parasitic conditions (strongyloidiasis, schistosomiasis and cutaneous larva migrans).5,11
In the index case, though we could not characterize the exact species as both fungal culture and molecular techniques (real-time PCR) were negative, diagnosis and timely intervention was based on the histo-morphological characterization alone. In the index case, plausibly the probable etiologic agent is Basidiobolus ranarum, epidemiologically this being the commonest entomophthoramycota responsible for human infections, and can affect GI tract without systemic dissemination. We postulate the route of infection to be the GI tract. Systemic/GI tract involvement is extremely rare with Conidiobolus species, and isolated liver involvement has not been described with Conidiobolus coronatus species. 7 In immunocompromised patients, Conidiobolus incongruus primarily involves lungs followed by rare secondary dissemination to other viscera like liver. Liver involvement has not been described with Conidiobolus lamprauges. In the absence of appropriate culture or molecular characterization, the possible etiological agent remains conjectural and is postulated by the clinical presentation of the disease.
Treatment of entomophthoramycosis is both medical and surgical. Prolonged systemic antifungal therapy coupled with surgical debridement is the cornerstone of treatment.1,2,12 Potassium iodide, co-trimoxazole, amphotericin B, various azoles and combinations of these agents have been tried with a varying degree of success. 13 Amphotericin B has shown resistance in a majority of cases. Potassium iodide was most successful in subcutaneous forms of the disease. Voriconazole and posaconazole have also been used successfully.1,12 Itraconazole is the most commonly used azole with promising clinical efficacy. Owing to the organism’s relative resistance to antifungals, prolonged therapy for 3–6 months at higher doses of 5 mg/kg twice daily is required.
Conclusion
Entomophthoroamycosis, an emerging disease in tropical and subtropical regions, usually affects immunocompetent hosts. It warrants physicians’ awareness owing to an exponential rise in this entity with global travel and a high index of suspicion in the setting of an unusual subcutaneous tissue swelling, abdominal masses with associated eosinophilia. Early diagnosis with biopsy, rapid institution of antifungals and complete surgical resection offer the best chance for cure. In the index case, though we could not characterize the exact species, diagnosis and intervention was based on the histopathological characterization of the organism.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
This study was approved by Department Review Board for abstract and publication submissions, Department of Paediatrics, Advanced Pediatric Centre, Postgraduate Institute of Medical Education and Research, Chandigarh, India (DRB-09-20).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.