
Abstract
The objective of this case series is the evaluation of the efficacy and visual outcomes after displacement of subretinal hemorrhage using intravitreal injection of recombinant tissue plasminogen activator, expansile gas, and in some cases an anti-vascular endothelial growth factor agent. A case series of 28 eyes of 28 patients (16 men and 12 women with age range 67–95 years) suffering from subretinal hemorrhage (duration range 1–15 days) caused by age-related macular degeneration or retinal macroaneurysm is presented. All the patients were treated with intravitreal injection of recombinant tissue plasminogen activator and gas and some of them received an anti-vascular endothelial growth factor agent between January 2013 and December 2016. The outcomes assessed were visual acuity (preoperatively 1 week, and 1 month postoperatively) with respect to duration and dimension of hemorrhage, displacement of hemorrhage, and possible complications of the procedure. Successful displacement of hemorrhage was achieved in 25 patients (89.3%), 18 of 28 patients had significant improvement in visual acuity 1 week after the treatment, and 22 of 28 patients had significant improvement in visual acuity 1 month after the treatment. The mean improvement of all patients with anatomical displacement of the hemorrhage in visual acuity was 0.7 ± 0.5 (LogMAR) in 1 month. Two patients developed vitreous hemorrhage after the procedure and one retinal detachment. Visual outcome a month after therapy displayed week correlation with duration, diameter, and thickness of hemorrhage. The results lead to the conclusion that intravitreal treatment of recombinant tissue plasminogen activator and expansible gas with or without injection of anti-vascular endothelial growth factor agent is effective in improving visual acuity and displacing submacular hemorrhage secondary to age-related macular degeneration and retinal macroaneurysm. The best functional outcomes can be expected in patients regardless of the size and duration of the hemorrhage.
Keywords
Introduction
Submacular hemorrhage (SMH) is the accumulation of blood between the neurosensory retina and retinal pigment epithelium (RPE) due to several conditions, such as ocular histoplasmosis, trauma, high myopia, retinal arterial macroaneurysm (RAM), age-related macular degeneration (ARMD), angioid streaks, and idiopathic polypoidal choroidal vasculopathy. 1
The most common cause for SMH is choroidal neovascularization, which occurs secondary to ARMD, particularly in patients taking anticoagulant medication. 2 If the hemorrhage is left untreated, it can damage irreversibly the RPE cells and the retina3,4 within 24 h, because of the direct toxicity derived from hemoglobin, the contraction of the clot which can cause mechanical damage to the outer segments, and the disturbances of diffusion between RPE and photoreceptors. 5 Despite the fact that intravitreal anti-vascular endothelial growth factor (VEGF) is the “gold standard” treatment for neovascular ARMD, monotherapy of anti-VEGF agent seems to be ineffective in restoring or improving visual acuity (VA) when large SMH is present.
RAMs are localized dilatations of a retinal arteriole, are seen in the elderly, and have a predilection for hypertensive women. Dyslipidemia and arteriosclerosis are also associated. 6 The vision may be affected in eyes with the presence of RAMs because of retinal edema with exudate formation, but occasionally RAMs can rupture and cause hemorrhages in various layers in the vitreoretinal tissues. The visual prognosis of eyes with the presence of vitreous hemorrhage or premacular hemorrhage associated with a RAM is good, in contrast to those with SMH with or without a premacular hemorrhage, which is generally poor. 7
A novel technique in order to displace SMH has been proposed by Heriot 8 in 1996, by combining a long-acting gas and an intravitreal injection of recombinant tissue plasminogen activator (r-tPA), without performing vitrectomy. tPA is a blood factor/protein in a recombinant form, which catalyzes breakdown of plasminogen to plasmin, aiding the endogenous fibrinolytic processes in dissolving blood clots. 9 Effective displacement of SMH from the fovea is achieved by mechanical (gas) effects as well as enzymatic (r-tPA) action. The final visual outcome after the displacement of the SMH though depends on additional factors such as patient’s age, underlying disease, duration, and thickness of the SMH. 10
Case section
This is a case series of 28 patients (16 males and 12 females), selected in a consecutive manner, presenting with acute submacular hemorrhage, who underwent enzymatic—mechanical treatment of SMH between 2013 and 2016 by five different surgeons. In all cases, hemorrhage, localized between the neurosensory retina and the RPE, was secondary to ARMD and retinal macroaneurysm. Written informed consent was obtained retrospectively from the patient(s) or a legally authorized representative(s) for anonymized patient information to be published in this article. The study was conducted in accordance with the Declaration of Helsinki.
At presentation, a comprehensive ophthalmic assessment was performed, including best corrected visual acuity (BCVA), biomicroscopic examination of the anterior segment of the eye, fundus photography, detailed dilated fundus examination, intraocular pressure (IOP) measurement, and spectral domain optical coherence tomography (OCT) scans. Patients with small SMH (less than 1 disk diameter) were not included in the study. Furthermore, patients with pre-existing retinal tears, diabetic retinopathy, retinal vein occlusion pathology, intravitreal hemorrhage, and history of previous photodynamic or laser therapy were excluded from the study. None of our patients had been diagnosed with massive subretinal hemorrhage.
All patients were examined before the treatment, 1 week and 1 month after surgery. The follow-up after the treatment with r-tPA, expansible gas, and anti-VEGF agent lasted at least 6 months. Postoperative VA, complications, dimensions, and displacement of SMH were recorded during follow-up visits.
The procedure protocol slightly varied between five surgeons. Treatment was performed in the operating theater under topical anesthesia and sterile conditions. Periocular region was cleaned with povidone-iodine and an eyelid speculum was positioned. We used a two-step surgical procedure to inject r-tPA (50 mcg in 0.1 mL) and gas (⩾0.3 mL of 100% SF6/C2 F6/C3 F8) through the pars plana into the vitreous cavity using a 30-gauge needle. Paracentesis of the anterior chamber was performed, when deemed necessary. Intravitreal injection of anti-VEGF was administered in all ARMD patients provided that they were not under any anti-VEGF treatment protocol. None of the RAM patients received anti-VEGF treatment. Oral acetazolamide was administrated as needed, based on the presence of increased IOP. Face-down posturing was advised to the patients for 3 days. Patients were re-examined and continuation of anti-VEGF therapy was advised according to the clinical need.
The following statistical methods were used for the analysis of the provided data. The significance in differences was set at p value < 0.05 with the qualitative variables analyzed with the chi-square (χ2) method assuming independent samples, 11 while the quantitative variables were not complied with the criteria of normality (Kolmogorov–Smirnov test) and were compared using Mann–Whitney test. In addition, the correlation between the variables was measured by Spearman’s correlation coefficient. All analyses were performed using IBM SPSS Statistics Ver. 24. Snellen VA was transformed to LogMAR for statistical analysis and comparison with previous studies.
Results
Regarding patient demographics (Table 1), 28 eyes of 28 patients are presented in this case series. The patients consisted of 16 men and 12 women with an average age of 82.5 years. The mean age of the patients who had anatomical displacement was 87.2 ± 9.2 years, while of those who did not have anatomical displacement was 88.3 ± 0.6 years. The SMH was due to neovascular AMD in 25 patients, while only 3 patients suffered from RAM. In 3 out of 28 patients, anatomical displacement of the SMH was unsuccessful. All of these three cases were patients with ARMD. In this case series, 17 out of 25 patients with ARMD received anti-VEGF treatment at the time of intervention. The rest 8 patients were already under an anti-VEGF regime before SMH occurred and their treatment protocol was continued as initially planned.
Patients with submacular hemorrhage secondary to age-related macular degeneration (ARMD) or retinal macroaneurysm who were treated with intravitreal injection of r-tPA, gas, an anti-VEGF agent, and face-down positioning.

VA: visual acuity; HG: hemorrhage; M: male; F: female; w: week; m: month; d: days; OCT: optical coherence tomography; VH: Vitreous Hemorrhage; RD: Retinal Detachment.
No OCT available or duration unknown due to patient reporting.
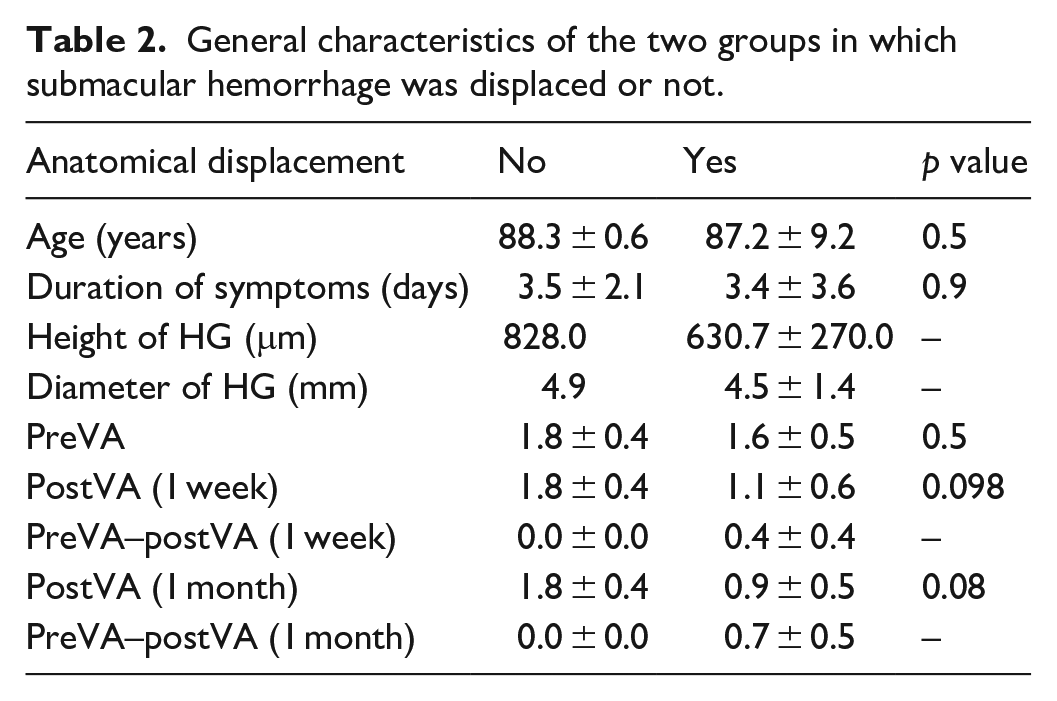
The mean duration of SMH was 3.5 ± 2.1 days in patients with no anatomical displacement and 3.4 ± 3.6 days in patients with anatomical displacement. The mean diameter of SMH was 4.9 mm in patients with no anatomical displacement, while the mean height of SMH was 828.0 μm. In patients with anatomical displacement the mean diameter of SMH was 4.5 ± 1.4 mm, while the mean height of SMH was 630.7 ± 270.0 μm (Table 2).
General characteristics of the two groups in which submacular hemorrhage was displaced or not.
Correlation analysis was carried out to establish an association between duration of SMH and the final visual outcome. We found no statistically significant correlation between postoperative VA gain on the first week and duration of SMH (r = −0.18, p = 0.40), as well as between postoperative VA gain on the first month and duration of SMH (r = −0.40, p = 0.06).
We also noticed that dimensions of the hemorrhage had no prognostic value for the postoperative visual outcome. In our study, no statistically significant relationship was revealed between VA gain on the first week and the height of the hemorrhage (r = 0.29, p = 0.21), as well as between VA gain on the first month and the height of the hemorrhage (r = −0.04, p = 0.85). Moreover, the correlation between diameter of the hemorrhage and VA gain on the first week was also considered as insignificant (r = − 0.40, p = 0.07), as well as regarding the postoperative VA gain on the first month (r = −0.26, p = 0.27).
Mean VA was improved from 1.6 ± 0.5 (LogMAR) at presentation to 1.1 ± 0.6 (LogMAR) during the first week in the patients with anatomical displacement. The mean gain in VA was 0.4 ± 0.4 (LogMAR) during the first week. The statistical analysis of patients’ data with anatomical displacement also revealed considerable improvement of final VA during the first month in the majority of patients compared with the preoperative VA with mean gain in VA 0.7 ± 0.5 (LogMAR) (Figures 1 and 2).

The change in best corrected visual acuity in different time points in patients with and no anatomical displacement.

The change in best corrected visual acuity in different time points in all patients.
Correlation analysis was also carried out to establish an association between the type of gas that was used and the outcome of successful or unsuccessful displacement. The statistical analysis did not display statistical differentiation (χ2 = 0.603, p = 0.704).
In these cases, we achieved successful displacement of the hemorrhage in 25 patients/eyes (25/28 patients—89.3%). An example of hemorrhage displacement and complete macular reconstruction in a patient is shown in Figure 3. Another example of complete clearance of subretinal blood with persistent sub-RPE blood is illustrated in Figure 4.

Complete displacement of SMH secondary to AMD in a patient treated with intravitreal r-tPA, gas, and anti-VEGF agent preoperatively and postoperatively. The figure represents Case 11 from Table 1.

Preoperative and postoperative OCT images of a patient with AMD, who was treated with intravitreal r-tPA, gas, and anti-VEGF agent. Displacement of extensive subretinal hemorrhage without successful removal of sub-RPE blood. The figure represents Case 6 from Table 1.
Postoperative complications were few and were observed in 3 patients (10.7%). In one patient retinal detachment developed, which was immediately repaired with retinal detachment surgery. Vitreous hemorrhage developed in 2 patients (13%). Of the 2 patients, 1 patient also had anterior chamber hemorrhage and vitreous to the wounds, while vitreous hemorrhage occurred in the other patient during the follow-up period, 3 months postoperatively.
Discussion
The objective of this case series was the assessment of the structural and functional outcomes of intravitreal injection of r-tPA and gas in the management of SMH. Long-standing SMH causes damage to retinal photoreceptors and pigment epithelium by various mechanisms, resulting in permanent visual loss. 5
The best visual outcomes may be expected in patients treated at an earlier stage. Hattenbach et al. 12 underlined the significance of the short treatment interval. Thus, the best final visual outcome was achieved when the duration of SMH was less than 14 days, while no visual improvement was noticed when treatment was delayed by more than 21 days. Sobolewska et al. 13 revealed that a combination of the intravitreal injection of r-tPA and gas seems to be more effective when it is applied within the first 4 days from the beginning of acute SMH. In addition, Tsymanava and Uhlig 14 suggest that, in patients with SMH associated with ARMD, the early treatment with 50–100 Lg r-tPA and gas application the next day is more beneficial for the development of BCVA, than in patients who did not received gas application the next day.
Various surgical techniques have been described to displace the blood and preserve macular function. The structural and functional outcomes of r-tPA and gas injection compare favorably with other surgical techniques described for the displacement of SMH. This method has the advantage of being minimally invasive, quick, cost-effective, and its relative accessibility may facilitate earlier intervention.
De Jong et al. 15 compared intravitreal injection of r-tPA, gas (C3F8), and bevacizumab with vitrectomy, subretinal injection of r-tPA, gas (C3F8), and bevacizumab. The median relative volume reduction of the hemorrhage was 97% and 100%, respectively, with no statistical significant difference between both the treatment groups. Moreover, the median VA improvement between these groups did not differ significantly.
A recent review of the literature on this topic classified the postoperative results between less invasive methods (r-tPA + Gas ± anti-VEGF—Group 1) and more invasive techniques (vitrectomy + subretinal r-tPA ± anti-VEGF—Group 2). Successful hemorrhage displacement was similar in both the groups (50%–100% in Group 1% and 53%–100% in Group 2), while more complications were reported in the more invasive group. 16 Hillenkamp et al. 17 also reported that intravitreal injection of r-tPA was associated with less complications compared with subretinal injection.
Abboud et al. 18 reported the favorable results of 4 patients who were treated with a protocol that combined the vitrectomy, the subretinal injection of r-tPA 0.025 mg/0.3 mL, the intravitreal injection of 0.05 mL of bevacizumab, and the retinal tamponade with 20% SF6 gas. Ozkaya et al. 19 also suggested the beneficial combination of vitrectomy, r-tPA, and gas for the outcome of the treatment, and they also revealed a correlation between the duration and area of SMH and the success of the displacement.
On the contrary, de Silva et al. presented a case series of patients with subfoveal macular hemorrhage, who received treatment with intravitreal tPA, C3F8, and anti-VEGF, irrespective of the severity and extent of hemorrhage. De Silva and Bindra 20 reported significant improvement of VA following treatment with similar benefits to more invasive therapies and therefore suggested early treatment with this triple therapy as a considerable firstline treatment for these patients. Araújo et al. 21 also suggest the intravitreal injection of r-tPA (50 μg/0.05 mL), which is followed by gas injection (0.3 mL SF6) as a minimally invasive procedure with few related complications, which is characterized by simplicity and few expenses.
Fujikawa et al. 22 compared the efficacy, safety, and visual outcomes of pneumatic displacement with or without tissue plasminogen activator (tPA) in 68 eyes with SMHs. In both groups similar displacement of SMH, visual improvement, and complication rates at 1 month were reported. On the contrary, Mizutani et al. 23 reported that the treatment of SMH secondary to AMD with intravitreal SF(6) gas in addition to tPA may be well-accepted, with good visual outcomes and no remarkable complications. However, they suggest that tPA is not recommended as a treating option for ruptured RAMs, due to a higher incidence of subsequent vitreous hemorrhage. Good visual outcomes with less re-bleeding could be provided by treatment without tPA. On the contrary, Mayer et al. 24 showed that r-tPA in combination with gas seems to be more effective than bevacizumab regarding the adverse effects such as vitreous hemorrhage.
Our work clearly has some limitations. First, there is a limited number of patients. Other limitations of our research were the absence of a control group and the difficulty in randomization of variables, such as diameter and height of SMH. Despite these limitations, the results of this case series are very indicative of the usefulness of intravitreal r-tPA and gas injection in the final visual outcome. In our sample, in two cases the treatment was offered a week after the hemorrhage occurred. Thus, it should be noted that even the belated intervention (more than a week) might offer an advantage to the improvement or stabilization of the final VA. More importantly, we can conclude that among early intervention (less than 1 week), the timing of surgery does not appear to change the final visual outcome.
Conclusion
Intravitreal r-tPA and gas injection seems to be relatively safe and effective for displacement of SMH due to exudative AMD and RAMs. However, multiple therapeutic approaches and lack of specific treatment guidelines highlight the need for larger randomized controlled trials in order to assess different treatment options. As demonstrated in our case series among early intervention (less than 1 week), the timing of surgery does not appear to change the final visual outcome.
Footnotes
Author contributions
Conceptualization of the paper was done by A.K., V.P., T.I., D.C., K.S., and R.H.; methodology by A.K., V.P., T.I., D.C., K.S., and R.H.; validation by A.K., V.P., T.I., D.C., K.S., and R.H.; formal analysis by A.K., V.P., T.I., D.C., K.S., R.H., S.K., and S.C.; investigation by A.K., V.P., T.I., D.C., K.S., and R.H.; writing and original draft preparation by A.K., S.K., and S.C.; writing, reviewing, and editing by A.K., S.K., and S.C.; visualization by A.K., S.K., and S.C.; supervision by A.K., N.Z., T.P., and R.H.; and project administration by A.K.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained retrospectively from the patient(s) or a legally authorized representative(s) for anonymized patient information to be published in this article.