
Abstract
Pyoderma gangrenosum is an uncommon neutrophilic dermatosis that is highly associated with pathergy in the setting of trauma or surgery, systemic disease, or may be idiopathic. Herein, we present the case of a 68-year-old female with ulcerative colitis who underwent a subtotal colectomy with an end-ileostomy and presented post-operatively with large, multifocal pyoderma gangrenosum at two abdominal sites. She was managed with intralesional triamcinolone injections and high-dose systemic steroids and was transitioned to IV infliximab. Our case report illustrates the role of infliximab in the treatment of complicated multifocal pyoderma gangrenosum and contemplates the impact of systemic infliximab exposure.
Introduction
Pyoderma gangrenosum (PG) is a rare neutrophilic dermatosis that presents as a painful, necrotic ulcer.1–3 It typically occurs in the second to fifth decade of life, with females more commonly affected than males. 4 The pathogenesis is poorly understood; however, it is hypothesized that lesions occur due to impaired neutrophilic function and aberrant immune system regulation in genetically susceptible individuals. 5 It most commonly occurs in patients with inflammatory bowel disease (IBD).4,6,7 Approximately, 30% of cases are associated with pathergy defined as an iatrogenic or incidental trauma. 6 A PG diagnosis is based on history, the presence of a deep necrotic ulcer with a violaceous border, histopathology positive for dermal edema and neutrophilic inflammation, and exclusion of other diagnoses.8,9 To date, there is limited data systematically evaluating the efficacy of therapy; however, small randomized control trials (RCTs) have described a role for systemic ciclosporin or prednisolone, with infliximab commonly reported as beneficial in patients with IBD.10–12 Despite the increasing report of infliximab concentrations associated with remission in luminal IBD, little to nothing is known regarding the required infliximab exposure for remission of PG.
Herein, we report the case of a 68-year-old female with ulcerative colitis (UC), who presented with large, multifocal PG of the abdomen associated with pathergy treated with infliximab with relatively low drug exposure. Written informed consent for patient information and images to be published was provided by the patient.
Case report
A 68-year-old female with UC presented to the hospital with a colonic perforation and underwent a subtotal colectomy with creation of an end-ileostomy. At her post-operative clinic visit, she reported diffuse abdominal pain with significant skin breakdown at her midline laparotomy incision and around her ostomy site.
On physical examination, she was afebrile but tachycardic. She had a large 10 × 10 cm2 purulent wound in her mid-lower abdomen adjacent to her ileostomy, with a 4-cm depth. The ulcer had violaceous edges with associated necrosis and granulation tissue in the inferior portion of her midline laparotomy incision with visible rectus abdominis (Figure 1(a)). In addition, she had 1.5 × 2 cm2 circumferential peri-stomal ulceration. Intact skin separated the lesions on general inspection; however, there was clear communication between the lesions.
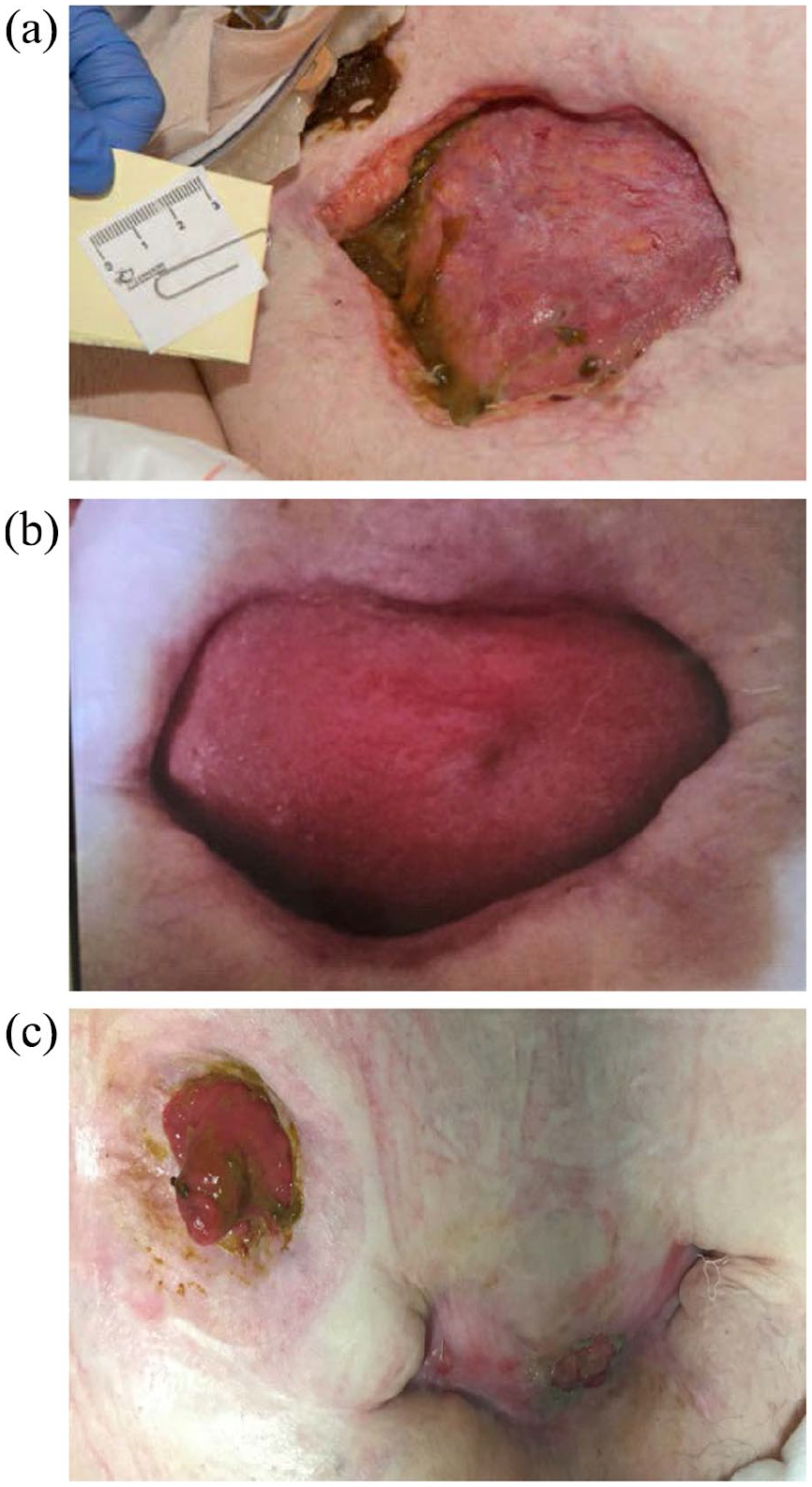
(a) Large 10 × 10 cm2 wound located in the mid-lower abdomen adjacent to the ileostomy after 2 months of regular wound care, high-dose systemic glucocorticoid therapy, and local injections with triamcinolone at 4 week intervals. (b) Abdominal wounds reduced to approximately 5 × 10 cm2 after 1 month of induction doses of infliximab (5 mg/kg) were given at week 0 and week 2. (c) Abdominal wounds 5 months after induction therapy with infliximab were given. Wounds significantly improved with near-complete closure compared to previous.
Biopsy results of the 10 × 10 cm2 abdominal wound showed “deep ulceration with acute subcutaneous inflammation and pustular dermatosis,” which supported a diagnosis of PG. She was initiated on high-dose methylpredni solone at her local hospital. There was lack of interval improvement in her lesions after 1 month and she was transferred to a tertiary care facility for management.
Local injections with triamcinolone were given at 4-week intervals. She was transitioned to daily oral prednisone 40 mg with a taper lasting 4 months. Given the lack of response to steroid therapy after 2 months, infliximab was initiated. Induction doses of infliximab (5 mg/kg) were given at week 0, week 2, and week 6, followed by a high-dose maintenance regimen (10 mg/kg every 8 weeks). Her infliximab drug concentration at week 14 of therapy was 5 µg/mL.
One month after receiving two doses of induction therapy with IV infliximab, her abdominal wounds reduced to approximately 5 × 10 cm2 (Figure 1(b)). Five months after induction therapy, her abdominal wounds significantly improved with near-complete closure compared to previous (Figure 1(c)).
Discussion
We present a case of PG in a patient with UC whereby large, abdominal, and multifocal communicating lesions occurred secondary to pathergy. In patients with IBD, the most common site of involvement is the lower extremities, though other sites are reported. 13 There are no guidelines for the treatment of PG. 14 Management consists of a combination of routine wound care and local and/or systemic immunosuppressant therapies. 10 A literature review by Reichrath et al. 12 attempted to provide guidance on this topic. They noted that systemic glucocorticoids and cyclosporine are first-line treatments for PG with the exception of individuals with co-morbid Crohn’s disease (CD), where infliximab should be considered first-line.12,14 Unfortunately, the majority of the infliximab studies included in this review were case reports, with only a limited number of small observational studies included. 12
An RCT of 30 patients (63% IBD) with PG involving the lower limbs (50%), the peri-stomal region (33%), and perineum (17%) demonstrated that 69% of patients who received a single dose of infliximab (5 mg/kg) had a clinical response by 6 weeks, with 21% achieving complete remission, though follow-up may have been premature.15,16 Another retrospective cohort study assessed 13 infliximab-exposed IBD patients with refractory PG, with 100% of patients having complete healing of their skin lesions. 17 A recent case-control study in 164 IBD patients found that infliximab was associated with a resolution rate of 63% in peri-stomal PG. 18 Of note, none of these studies reported the infliximab concentrations in individuals achieving remission.
Even with multifocal and deep PG, the patient described herein had an excellent response to infliximab therapy, despite a lack of improvement with systemic glucocorticoids. Interestingly, her serum infliximab concentration following induction therapy was relatively low (5 μg/mL). Given her extensive PG, one might expect that she would require a higher infliximab exposure as was described by Yarur et al. 19 in patients with fistulizing CD. No studies have documented the infliximab concentrations that are associated with PG healing in IBD. This lower infliximab concentration may suggest a more active contribution of the ancillary treatments used for PG resolution (wound care, glucocorticoids, intralesional injections). The co-administration of multiple treatments is a confounding factor in the majority of published reports on PG and limits the objective evaluation of infliximab in these cases. Conversely, low systemic infliximab exposure may suggest accumulation of infliximab within the affected compartment (PG wound) as being of primary importance. 20 This concept, was suggested by Teich and Klugmann, 20 whereby the direct application of an infliximab gel to the affected lesion resulted in a “rapid improvement” in PG. Thus, measures of systemic exposure may not be as meaningful. Further studies evaluating infliximab concentration are warranted in this population. Overall, the presented case highlights various concepts that are not well described in the contest of PG. Specifically, the role of therapeutic drug monitoring, the value of infliximab-dose escalation, and the target infliximab trough concentration in PG have not been meaningfully explored.
In conclusion, PG is a neutrophilic dermatosis that commonly occurs as an extra-intestinal manifestation in patients with underlying IBD. Based on limited randomized data, infliximab has been shown to increase wound healing and induce remission, particularly in refractory PG. Herein, we presented the case of a 68-year-old female with UC who presented with large, multifocal refractory PG which was successfully treated with infliximab therapy despite a low systemic drug exposure. Despite a long history of use in IBD-associated PG, little is known about the pharmacokinetics of infliximab in PG and the extent and nature of drug exposure needed to achieve healing. Gastroenterologists are reliant on trough concentrations to guide the use of infliximab in the management of luminal disease; however, this concept has not been assessed in IBD-associated PG. This case report highlights the need for further studies in this area.
Footnotes
Author contributions
Each author takes responsibility and accountability for the published work and has met the conditions listed in the ICMJE criteria for authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Dr Maria Mikail.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.